Pulmonary mechanics full details for md exams
Reading File
search_medical_text
pulmonary mechanics lung volumes capacities compliance resistance work of breathing
search_medical_text
airway resistance flow-volume loops spirometry FEV1 FVC obstructive restrictive lung disease
search_medical_image
lung volumes capacities spirometry flow volume loop diagram
GradeResponse
GradeResponse
GradeResponse
Good results retrieved. Now I have strong foundational content. Let me synthesize a comprehensive MD exam review on pulmonary mechanics from the retrieved sources and my own knowledge.
Pulmonary Mechanics — Complete MD Exam Review
1. Lung Volumes & Capacities
These are the cornerstone of understanding pulmonary mechanics. Memorize the values and what changes them.
| Volume/Capacity | Definition | Normal Value |
|---|---|---|
| Tidal Volume (TV) | Air moved per normal breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Extra air above TV that can be inhaled | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Extra air below TV that can be exhaled | ~1200 mL |
| Residual Volume (RV) | Air remaining after maximal exhalation | ~1200 mL |
| Inspiratory Capacity (IC) | TV + IRV | ~3500 mL |
| Functional Residual Capacity (FRC) | ERV + RV | ~2400 mL |
| Vital Capacity (VC) | IRV + TV + ERV | ~4700 mL |
| Total Lung Capacity (TLC) | All volumes combined | ~6000 mL |
Key Rule: RV, FRC, and TLC cannot be measured by spirometry alone — they require helium dilution, nitrogen washout, or body plethysmography.
FRC: The Equilibrium Point
FRC is the resting lung volume where the inward elastic recoil of lung = outward recoil of chest wall. This is the key balance point.
| FRC changes | Cause |
|---|---|
| ↑ FRC | Emphysema (loss of elastic recoil), aging, asthma |
| ↓ FRC | Obesity, supine position, pregnancy, pulmonary fibrosis, ARDS |
2. Compliance
Compliance (C) = ΔVolume / ΔPressure
It measures the distensibility (stretchability) of the lung or chest wall.
Types of Compliance
| Type | What it measures |
|---|---|
| Static compliance | Compliance at zero flow; reflects elastic properties only |
| Dynamic compliance | Compliance during breathing; affected by both elastance AND airway resistance |
Pressure-Volume (P-V) Curve
- The lung P-V curve is sigmoid-shaped
- Hysteresis: The inflation and deflation curves do not overlap — the lung inflates at a higher pressure than it deflates at any given volume
- Hysteresis occurs due to surfactant and recruitment of collapsed alveoli
Clinical Correlations
| Condition | Compliance | Mechanism |
|---|---|---|
| Emphysema | ↑↑ | Destruction of elastic tissue |
| Pulmonary fibrosis | ↓↓ | Stiff, scarred lung |
| Pulmonary edema | ↓ | Fluid fills alveoli |
| ARDS | ↓↓ | Alveolar damage + surfactant loss |
| Normal aging | Slight ↑ | Gradual loss of elastic recoil |
Surfactant
- Produced by Type II pneumocytes
- Composition: mainly dipalmitoylphosphatidylcholine (DPPC)
- Function: reduces surface tension → increases compliance → prevents alveolar collapse
- LaPlace's Law: P = 2T/r — in small alveoli (small r), pressure would be very high WITHOUT surfactant → small alveoli would empty into large ones (atelectasis)
- Surfactant lowers T disproportionately in small alveoli → equalizes pressure → prevents collapse
- Neonatal RDS: surfactant deficiency in premature infants (<34 weeks) → stiff lungs, atelectasis
3. Airway Resistance
Resistance (R) = ΔPressure / Flow
- Major site: medium-sized bronchi (NOT the smallest airways — they have large total cross-sectional area)
- Airways contribute ~80% of total resistance; tissue viscance ~20%
Poiseuille's Law
$$R = \frac{8\eta L}{\pi r^4}$$
- Resistance is inversely proportional to the 4th power of radius → small changes in radius cause enormous changes in resistance
- Doubling the radius → 16× decrease in resistance
Factors Affecting Airway Resistance
| Factor | Effect on Resistance |
|---|---|
| Bronchospasm (asthma) | ↑↑↑ |
| Mucus/secretions | ↑ |
| Lung inflation (high lung volumes) | ↓ (airways dilated by radial traction) |
| Low lung volumes / dynamic compression | ↑ |
| Sympathetic stimulation (β₂) | ↓ (bronchodilation) |
| Parasympathetic stimulation | ↑ (bronchoconstriction) |
| Histamine, leukotrienes | ↑ |
Dynamic Airway Compression (Forced Expiration)
During forced expiration, pleural pressure becomes positive. At a critical point along the airway — the equal pressure point (EPP) — airway pressure equals pleural pressure. Downstream of EPP, airways collapse → flow limitation.
- In emphysema: EPP moves upstream (peripherally), worsening collapse → air trapping, ↑ RV
- This is why pursed-lip breathing helps COPD patients — raises back-pressure, delays airway collapse
4. Spirometry & Pulmonary Function Tests
Key Spirometric Values
| Parameter | Definition | Normal |
|---|---|---|
| FVC | Forced vital capacity | ~80% predicted |
| FEV₁ | Vol expelled in 1st second of FVC | ~80% predicted |
| FEV₁/FVC ratio | Key diagnostic ratio | ≥0.70 (≥70%) |
| FEF 25–75% | Mid-expiratory flow rate | Sensitive for small airway disease |
| PEFR | Peak expiratory flow rate | Effort-dependent |
Obstructive vs. Restrictive Pattern
| Feature | Obstructive | Restrictive |
|---|---|---|
| FEV₁ | ↓ | ↓ |
| FVC | Normal or ↓ | ↓↓ |
| FEV₁/FVC | ↓ (<0.70) | Normal or ↑ |
| TLC | ↑ (air trapping) | ↓ |
| RV | ↑↑ | ↓ or normal |
| Examples | COPD, asthma, bronchiectasis | IPF, sarcoidosis, obesity, kyphoscoliosis |
Flow-Volume Loops (Harrison's, p. 7860)
According to Harrison's Principles of Internal Medicine (p. 7860), flow-volume loops have characteristic shapes:
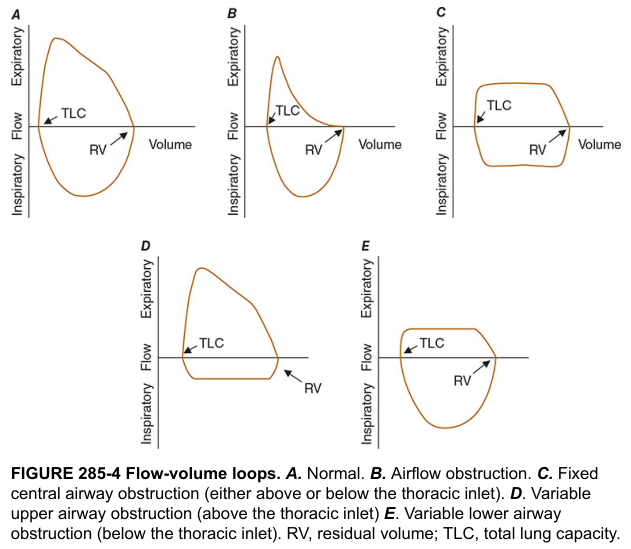
| Loop Pattern | Shape | Diagnosis |
|---|---|---|
| Normal (A) | Broad rounded expiratory limb | Normal |
| Obstruction (B) | Scooped-out (concave) expiratory limb | COPD, asthma |
| Fixed central obstruction (C) | Plateauing of BOTH inspiratory & expiratory limbs | Tracheal stenosis, goiter |
| Variable extrathoracic (D) | Inspiratory limb plateau only | Vocal cord paralysis, subglottic stenosis |
| Variable intrathoracic (E) | Expiratory limb plateau only | Tracheomalacia |
Memory Aid — Variable lesions:
- Extrathoracic → Inspiratory plateau (E-I mnemonic)
- Intrathoracic → Expiratory plateau (I-E mnemonic)
- During inspiration: negative pleural pressure opens intrathoracic airways but narrows extrathoracic segment → extrathoracic obstruction worsens on inspiration
5. Work of Breathing
Work = Pressure × Volume
Work is done against:
- Elastic recoil (compliance work) — dominant at normal breathing rates
- Airway resistance (resistive work) — dominant at high flow rates
- Tissue viscance (minor)
Optimal Breathing Rate
- Elastic work ↑ with larger tidal volumes (slow deep breathing)
- Resistive work ↑ with faster flow
- The body adopts a breathing pattern that minimizes total work
- Patients with stiff lungs (↑ elastic work) breathe rapidly and shallowly
- Patients with high resistance (↑ resistive work) breathe slowly and deeply
Oxygen Cost of Breathing
- Normal: ~2% of total VO₂
- In respiratory failure: can rise to 40–50% → respiratory muscles steal O₂ from other organs → a key indication for mechanical ventilation
6. Mechanics During Mechanical Ventilation
According to Harrison's Principles of Internal Medicine (p. 8183), during volume-controlled ventilation:
- Peak airway pressure = determined by airway resistance + respiratory system compliance
- Plateau pressure (end-inspiratory pause) = determined by compliance ONLY (no flow, so resistance doesn't contribute)
- Peak − Plateau pressure difference = reflects airway resistance
| Scenario | Peak Pressure | Plateau Pressure |
|---|---|---|
| Bronchospasm / mucus plug | ↑↑ | Normal |
| ARDS / pulmonary edema (↓ compliance) | ↑↑ | ↑↑ |
| Both (intubated COPD with mucus) | ↑↑ | ↑ |
7. Ventilation–Perfusion (V/Q) Relationships
Regional Differences (Upright Lung)
- Gravity causes both ventilation (V) and perfusion (Q) to be greater at the base than the apex
- Q increases more steeply than V from apex to base
- Therefore:
- Apex: V/Q > 1 (relative dead space — wasted ventilation)
- Base: V/Q < 1 (relative shunt — wasted perfusion)
- Overall mean V/Q ≈ 0.8
| Zone | V/Q Ratio | Clinical Equivalent |
|---|---|---|
| V/Q = 0 | Pure shunt (perfused, unventilated) | Lobar pneumonia, ARDS |
| V/Q = ∞ | Pure dead space (ventilated, unperfused) | PE |
| V/Q normal | 0.8 | Healthy alveolus |
Dead Space
- Anatomical dead space (~150 mL): conducting airways that don't participate in gas exchange
- Alveolar dead space: ventilated but unperfused alveoli (negligible in health)
- Physiological dead space = anatomical + alveolar dead space
- Bohr equation: VD/VT = (PaCO₂ − PECO₂) / PaCO₂
8. Key Equations Summary Table
| Equation | Formula | Clinical Use |
|---|---|---|
| Compliance | C = ΔV/ΔP | Stiffness of lung |
| Resistance | R = ΔP/Flow | Airway obstruction |
| Poiseuille's Law | R = 8ηL/πr⁴ | Radius critical for resistance |
| LaPlace's Law | P = 2T/r | Surfactant physiology |
| Bohr equation | VD/VT = (PaCO₂−PECO₂)/PaCO₂ | Dead space calculation |
| Alveolar gas equation | PAO₂ = PiO₂ − (PaCO₂/RQ) | A-a gradient |
| A-a gradient | PAO₂ − PaO₂ | Normal <10–15 mmHg (young) |
9. High-Yield Exam Buzzwords
| Finding | Diagnosis |
|---|---|
| Scooped-out expiratory loop | Obstructive lung disease |
| Bilateral plateau on flow-volume loop | Fixed central airway obstruction |
| ↑ TLC + ↑ RV + ↓ FEV₁/FVC | Emphysema |
| ↓ TLC + ↓ RV + normal FEV₁/FVC | Pulmonary fibrosis |
| Peak >> Plateau on vent | ↑ Airway resistance (bronchospasm) |
| Peak ≈ Plateau (both ↑) on vent | ↓ Compliance (ARDS, pulmonary edema) |
| Rapid shallow breathing | Stiff lung (minimize elastic work) |
| Slow deep breathing | High resistance (minimize resistive work) |
| Pursed-lip breathing | COPD — prevents dynamic airway collapse |
| Grunting in neonate | Functional PEEP — prevents alveolar collapse |
10. Quick Mnemonics
- "COPD Blows Out" → ↑ RV, ↑ TLC, ↑ FRC (air trapped, can't blow it out)
- "Fibrosis Shrinks" → ↓ TLC, ↓ RV, ↓ FVC, normal FEV₁/FVC
- "FEF 25–75 = Small Airways" → earliest marker in smokers
- "Type II makes surfactant" → remember: Two = Too much surface tension without it
- EPP = Equal Pressure Point → where dynamic collapse begins; moves peripherally in emphysema
Sources: Harrison's Principles of Internal Medicine, 21st Ed., pp. 7850, 7860, 8183; supplemented from standard physiology references (West's Respiratory Physiology).
This is a shared conversation. Sign in to Orris to start your own chat.