Defecation reflex Guyton
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is the complete account of the defecation reflex as described in Guyton and Hall Textbook of Medical Physiology (Ch. 64).
Defecation Reflex - Guyton & Hall
Background: The Rectum is Normally Empty
Most of the time the rectum contains no feces. A weak functional sphincter at the sigmoid-rectal junction (~20 cm from the anus), combined with a sharp angulation at that junction, prevents premature filling. When mass movements (powerful propulsive contractions of the colon) drive feces into the rectum, the urge to defecate arises immediately, along with reflex contraction of the rectum and relaxation of the anal sphincters.
Anal Sphincters
Two sphincters maintain continence:
| Sphincter | Composition | Control |
|---|---|---|
| Internal anal sphincter | Several-cm thickening of circular smooth muscle, immediately inside the anus | Involuntary (autonomic) |
| External anal sphincter | Striated voluntary muscle; surrounds and extends distal to internal sphincter | Voluntary/subconscious - via pudendal nerve (somatic) |
The external sphincter is tonically constricted at all times unless conscious signals override it.
The Two Defecation Reflexes
Guyton describes two reflexes that work together:
1. Intrinsic Myenteric (Enteric) Defecation Reflex
- Triggered when feces distend the rectal wall
- Afferent signals spread through the myenteric plexus
- Peristaltic waves are initiated in the descending colon, sigmoid, and rectum, pushing feces toward the anus
- As the peristaltic wave reaches the anus, inhibitory signals from the myenteric plexus relax the internal anal sphincter
- If the external sphincter is also voluntarily relaxed, defecation occurs
- By itself, this reflex is relatively weak - normally insufficient to cause effective defecation
2. Parasympathetic Defecation Reflex (the fortifying reflex)
- Involves the sacral segments (S2-S4) of the spinal cord
- When rectal nerve endings are stimulated, signals travel up to the spinal cord, then return via parasympathetic fibers in the pelvic nerves to the descending colon, sigmoid, rectum, and anus
- These parasympathetic signals greatly intensify peristaltic waves and relax the internal anal sphincter
- This converts a weak intrinsic reflex into an effective one
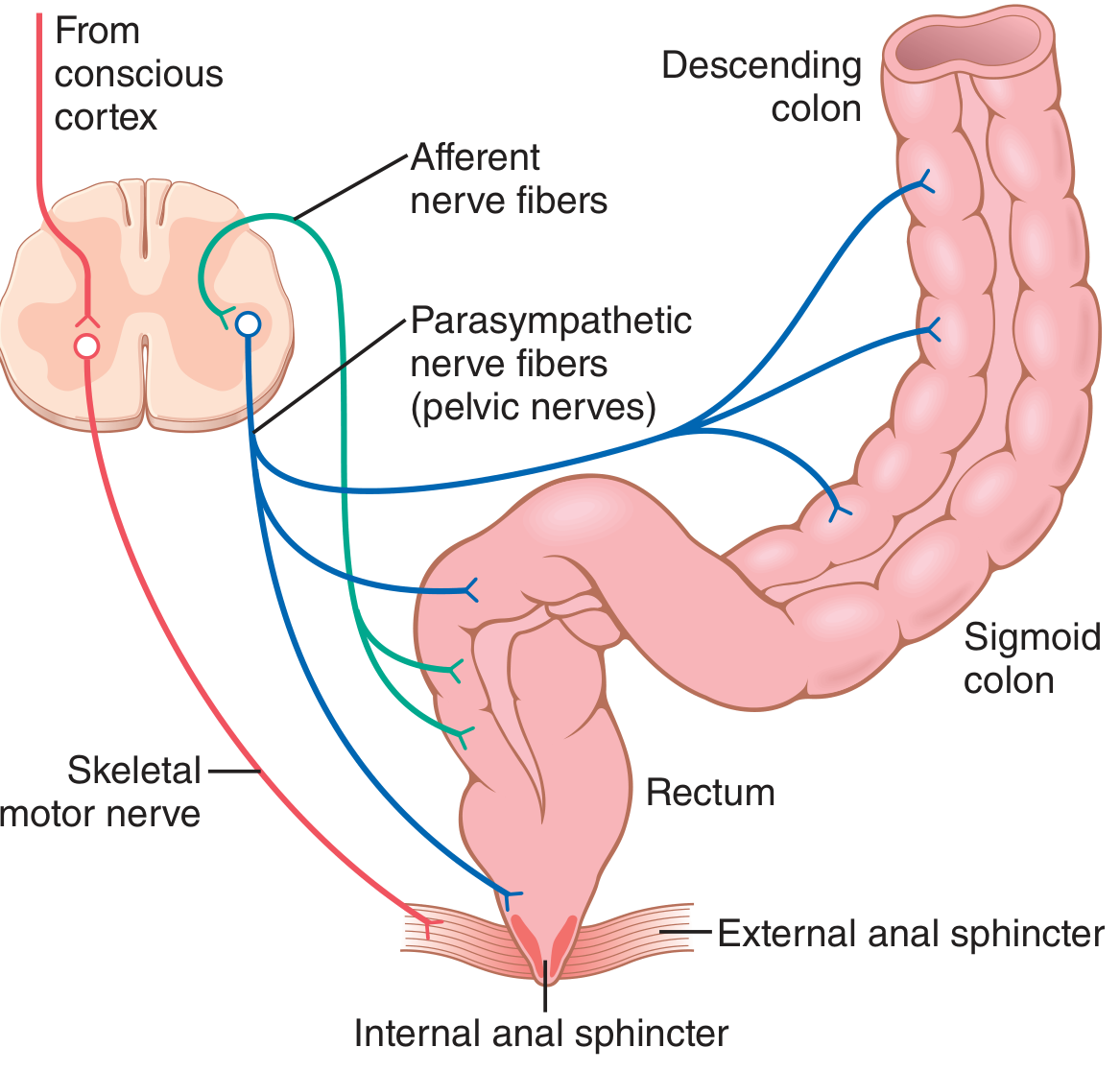
Fig. 64.6 - Afferent nerve fibers carry signals to the sacral cord; parasympathetic fibers (via pelvic nerves) return to the descending colon, sigmoid, rectum, and sphincters. The skeletal motor nerve (pudendal) from the conscious cortex controls the external sphincter.
Accessory Maneuvers During Defecation
Signals entering the spinal cord also trigger:
- Deep inspiration - diaphragm descends
- Closure of the glottis
- Contraction of abdominal wall muscles - raises intra-abdominal pressure, forcing feces caudally
- Pelvic floor relaxation with outward pull on the anal ring - evaginates feces
Voluntary Initiation
When convenient, the defecation reflexes can be deliberately activated by:
- Taking a deep breath (diaphragm moves down)
- Contracting abdominal muscles (raises abdominal pressure)
- This forces fecal contents into the rectum, triggering new reflexes
However, voluntarily-initiated reflexes are never as effective as naturally-arising ones. Habitual suppression of the natural urge leads to constipation.
Clinical Correlates
- Newborns and spinal cord transection: The defecation reflex causes automatic emptying at inconvenient times because the conscious voluntary control of the external sphincter (via the cortex and pudendal nerve) is absent.
- Constipation from suppression: Repeatedly inhibiting natural reflexes weakens their effectiveness over time.
- Spinal cord injuries (discussed in Ch. 64): Normal spinal cord-mediated defecation reflex from the conus medullaris can be disrupted, leading to bowel paralysis.
Source: Guyton and Hall Textbook of Medical Physiology, Chapter 64 - Propulsion and Mixing of Food in the Alimentary Tract, pp. 794-796
This is a shared conversation. Sign in to Orris to start your own chat.