Explain me Scott brown’s chapter 10 soft tissue repair in creative manner. It is difficult for me to memorise everything in it, give me some brilliant ideas to memorise it thoroughly
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent! Now I have everything I need. Let me craft a creative, memorable explanation of the entire chapter:
Scott-Brown's Chapter 10: Soft Tissue Repair - The Complete Creative Guide
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, Chapter 10
THE STORY: "THE CITY AFTER AN EARTHQUAKE"
Think of your skin as a city. When a wound happens, it's an earthquake. The repair is the city's emergency response and reconstruction. Every phase has its team, its timeline, its tools. Here's the whole drama.
PART 1 - TYPES OF WOUND HEALING: "HOW DO YOU SEAL THE CRACK?"
Use the mnemonic "1-2-3 SEAL":
| Type | Nickname | When | Key Detail |
|---|---|---|---|
| 1st Intention | "Zip it shut" | Clean cut, edges touching | Closed within 12-24 hrs (sutures/glue/steri-strips). Least scarring |
| 2nd Intention | "Let it fill" | Large gap, infected | Granulation tissue fills the cavity; myofibroblasts appear at day 3; slower, risks contracture |
| 3rd Intention (delayed primary) | "Wait, then zip" | Contaminated (bite wounds, soiled abdomen) | Left open 3-4 days for host defences, THEN edges approximated |
Memory trick: Count your fingers:
- 1 finger = One cut, zipped clean (1st intention)
- 2 fingers = Two sides far apart, fill the gap (2nd intention)
- 3 fingers = Three days wait, then zip (3rd intention)
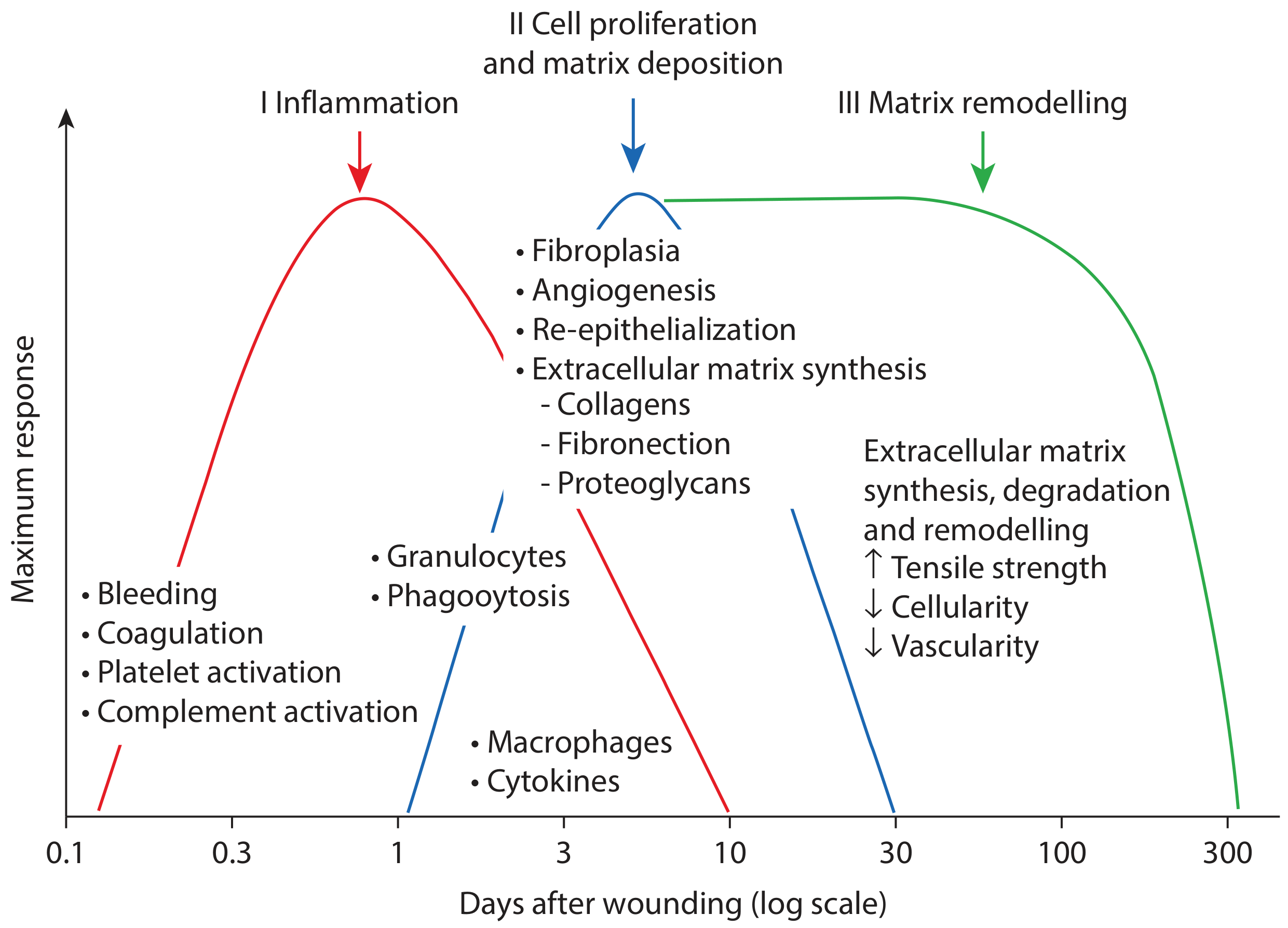
PART 2 - THE 4 PHASES: "HIRE PR FM"
The Earthquake Analogy + Mnemonic: H.I.P.R. (Haemostasis → Inflammation → Proliferation → Remodelling)
Think: "He Is Pretty Reliable"
🔴 PHASE 1: HAEMOSTASIS (Minutes to hours)
The First Responders (Fire brigade sealing the gas leak)
- Vascular endothelium disrupted → vasoconstriction
- Platelets activate, aggregate, degranulate → release the big four growth factors:
| Growth Factor | Job |
|---|---|
| PDGF | Chemotaxis (attract more workers) |
| TGF-β | ECM deposition |
| EGF | Epithelialization |
| VEGF | Angiogenesis (new blood vessels) |
Memory trick - "Please Tell Every Visitor" = PDGF, TGF-β, EGF, VEGF
🟡 PHASE 2: INFLAMMATION (Hours to Day 3)
The Cleanup Crew (Hazmat team clearing debris)
The city calls two teams in order:
- Neutrophils arrive FIRST (day 0-2) - they're the "quick responders", do phagocytosis of bacteria
- Macrophages arrive SECOND (day 2-3) - the "supervisors", they:
- Phagocytose bacteria AND necrotic debris
- Release cytokines
- Are essential for fibroblast division, collagen synthesis, angiogenesis
Memory trick: "N before M" = Neutrophils before Macrophages (alphabetical order of arrival!)
The inflammation phase has two sub-stages:
- Early inflammation (day 0-2): neutrophil dominance, vascular permeability, no collagen bridging yet
- Late inflammation (day 2-3): macrophages take over, collagen fibres appear at wound margins but don't bridge yet
🔵 PHASE 3: PROLIFERATION (Day 3 to Week 2, up to 4 weeks)
The Construction Crew (Builders rebuilding the city)
This phase has 3 sub-contractors under "Granulation Tissue Formation":
FAR = Fibroplasia + Angiogenesis + Re-epithelialization
3a. RE-EPITHELIALIZATION
- Basal cells start dividing within 12 hours of wounding
- Keratinocytes extend lamellipodia ("little feet") across the wound - called epiboly
- Migration is fastest in hyperbaric (high oxygen) conditions
- Contact inhibition stops movement when sheets meet
- In partial-thickness wounds, hair follicles and sebaceous glands act as extra epithelial sources
Memory trick: "EPIC EPIBOLY" - Epithelial cells march like an epic army with tiny feet
3b. FIBROPLASIA
- Fibroblasts arrive day 2-4, attracted by PDGF and TGF-β
- They produce the ECM: fibronectin, hyaluronan, collagen, proteoglycans
- Some fibroblasts become myofibroblasts (under influence of mechanical tension + PDGF) - these cause wound contraction
- ECM is a scaffold of:
- Fibrous proteins: collagen + elastin
- Interstitial matrix: glycoproteins in proteoglycan gel
Memory trick: "FiBRO = FIll, BRidge, Organize" - fibroblasts fill the gap, bridge the wound, organize the ECM
3c. ANGIOGENESIS
- New vessels sprout to supply the new granulation tissue
- Driven by VEGF and FGF
- The whole granulation tissue package = collagen + proteoglycans + new vessels
🟢 PHASE 4: REMODELLING (Week 3 to 1 year+)
The Interior Designers (Finishing the city after construction)
- Type III collagen (immature, "baby collagen") → replaced by Type I collagen (mature, strong)
- Tensile strength increases - wound reaches only ~80% of original strength maximum
- Cellularity decreases
- Vascularity decreases
Memory trick: "3 becomes 1, strength is won" - Type III collagen becomes Type I, and strength is regained
PART 3 - CELLS AND CYTOKINES: THE "DREAM TEAM" TABLE
The Cast of Characters (Table 10.1)
| Cell | Role | Arrival |
|---|---|---|
| Platelets | Clot + cytokine release (TGF-β, PDGF, platelet factor-4) | Immediate |
| Neutrophils | First responders, phagocytosis | Immediate-Day 2 |
| Macrophages | Phagocytosis + cytokines + activate fibroblasts + angiogenesis | Day 2-3 |
| Lymphocytes | Role unclear, some cytokines | Late |
| Fibroblasts | Build ECM, granulation tissue, myofibroblasts | Day 2-4 |
| Keratinocytes | Re-epithelialization + destroy microorganisms | Day 0.5 onwards |
Memory trick - "Please Never Make Lemon Fudge Kake" = Platelets, Neutrophils, Macrophages, Lymphocytes, Fibroblasts, Keratinocytes
PART 4 - ABNORMAL WOUND HEALING: "THE BAD NEIGHBOURS"
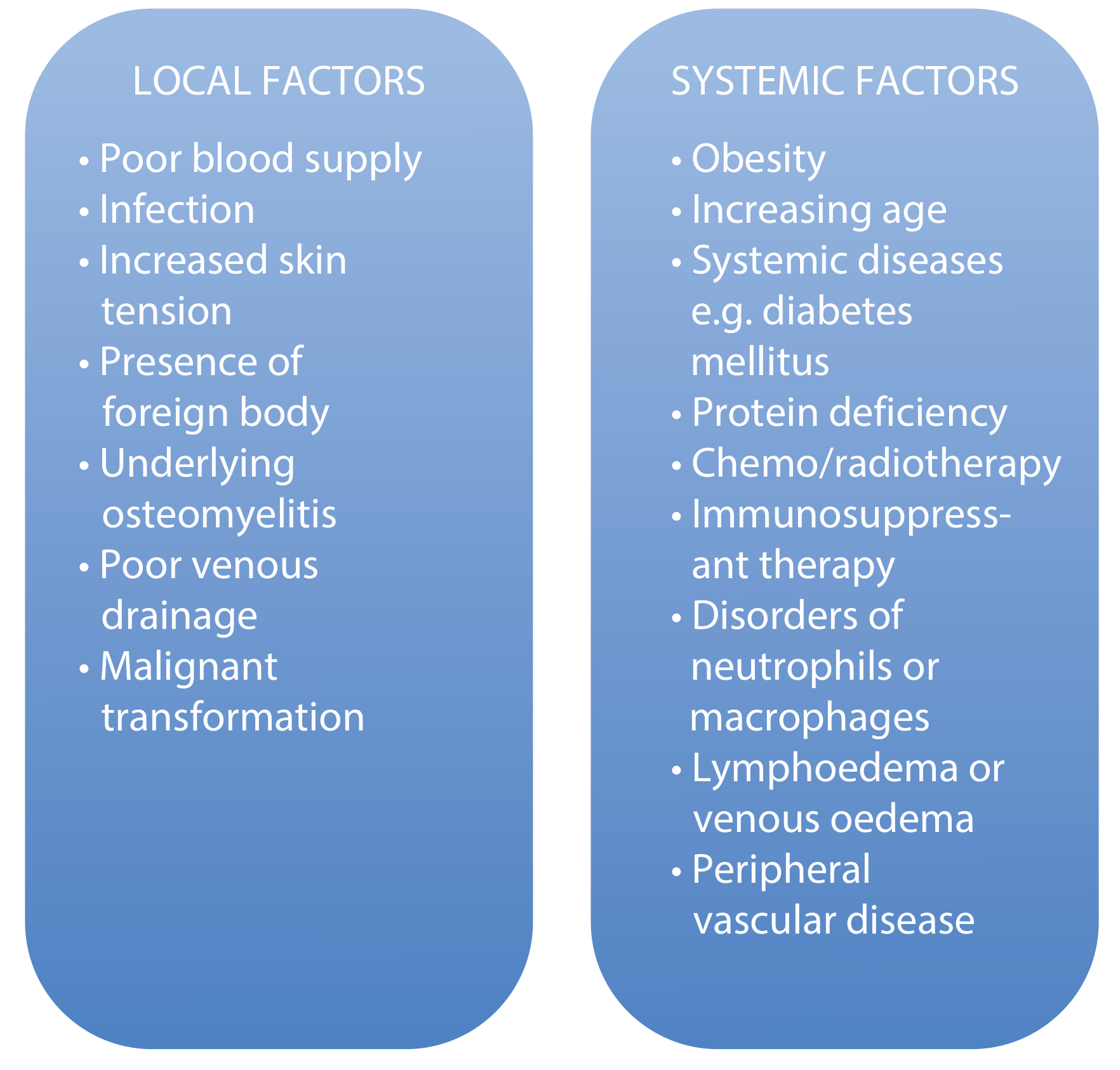
Local Factors (things AT the wound site) - "PIFPOM"
- Poor blood supply
- Infection
- Foreign body
- Poor venous drainage
- Osteomyelitis (underlying)
- Malignant transformation
-
- Increased skin tension
Systemic Factors (things in the whole body) - "OADPCILD"
- Obesity
- Age (increasing)
- Diabetes mellitus (+ other systemic diseases)
- Protein deficiency
- Chemo/radiotherapy
- Immunosuppressant therapy
- Lymphoedema/venous oedema
- Disorders of neutrophils/macrophages
-
- Peripheral vascular disease
Nutritional markers to remember - "SAT":
- Serum albumin < 30 g/L = delayed healing
- Albumin substitute: Pre-albumin < 10 mg/dL (shorter half-life, better acute marker)
- Transferrin < 1.5 g/L = delayed healing
Pro-healing nutrients - "AVAZ": Arginine, Vitamin A, Vitamin C (Ascorbic acid), Zinc
PART 5 - WOUND CLASSIFICATION: "THE TWO BIG TREES"
Tree 1: Acute vs Chronic
Acute wounds (generally heal well):
- Thermal (burns, radiation)
- Surgical (incisions, excisions, skin grafts, amputations)
- Traumatic
Burns Classification - "SePF":
- Superficial - erythema, epidermis only, no intervention needed
- Partial-thickness - blistered, epidermis + part of dermis
- Superficial PT: minimal intervention
- Mid/Deep dermal: watch carefully, may need grafting
- Full-thickness - charred/white, insensate, ALWAYS need skin grafts
Chronic wounds (>6 weeks, needs an underlying cause):
- Diabetic ulcers
- Pressure ulcers
- Venous ulcers (medial malleolus, sloping edges)
- Arterial ulcers (punched-out edges)
- Mixed ulcers
- Risk of Marjolin's ulcer (malignant transformation!)
Memory trick for chronic wound edges:
- "Venous = Valley slope" (sloping edges)
- "Arterial = Abrupt punch" (punched-out edges)
- "Rolled edges = Rule out malignancy"
Tree 2: By Tissue Type
- Granulation - pink, healthy; dark red/bleeding = infected; excess = "proud flesh"
- Epithelializing - superficial wounds
- Necrotic - slough (yellow, moist, stringy) vs eschar (black, dry, leathery post-burn)
- Infected - classical signs: "P.P.E.M.W.P.I.S" = Pyrexia, Pus, Erythema (spreading), Malodour, Wound dehiscence, Poor healing, Increased pain, Sinus formation
PART 6 - WOUND ASSESSMENT: "SIZE, EDGE, LOCATION, BED" = SELB
- Size - trace on acetate; area = length × perpendicular width
- Edge - sloping = venous; punched-out = arterial; rolled/everted = exclude malignancy
- Location - venous = gaiter region/medial malleolus; diabetic = pressure areas (hallux, 1st/5th MT heads, heel)
- Bed - pink = healthy; dark red = infected; excess = overgranulation
Assessment techniques = Invasive (biopsy, swab, doppler) + Non-invasive (photography, acetate tracing, thermometry)
Wound infection threshold: 10^5 bacteria per gram of tissue
PART 7 - WOUND DRESSINGS: "The 5 Dressing Families"
"Hype! Foam Films Agree" = Hydrogel, Hydrocolloid, Foam, Film, Alginate
| Dressing | Best For | Memory |
|---|---|---|
| Hydrogel (AquasorB) | Dry + necrotic wounds | "Gel = rehydrate the dead" |
| Hydrocolloid | Dry necrotic, sloughy, granulating | "Colloid = do-it-all" |
| Foam | Granulating wounds with medium exudate; also cavity wounds | "Foam soaks up exudate" |
| Film (OpSite) | Clean, dry, epithelializing wounds | "See-through film for healing wounds" |
| Alginate | Sloughy, granulating, highly exuding, partial-thickness burns | "Algae from the sea, soaks exudate like a sponge" |
Quick Dressing Decision Tree:
Necrotic wound? → Hydrogel or hydrocolloid (rehydrate to separate eschar)
Sloughy wound? → Hydrofibre/hydrogel/hydrocolloid/alginate + debridement
Granulating wound?
- Light-medium exudate → hydrocolloid or thin foam
- Deep cavity → alginate ribbons, foams, VAC therapy
Epithelializing wound?
- Dry → hydrocolloid or film
- Wet → alginate or foam
Burns:
- Superficial → semipermeable film, hydrocolloid, Mepitel, Aquacel
- Partial thickness → Flamazine, alginates, Mepitel, Aquacel
- Full thickness → Flamazine, hydrogels, Mepitel + refer to burns centre
The VAC system (vacuum-assisted closure) is used for deep cavity granulating wounds.
MASTER MNEMONIC SUMMARY: "WHAM PIR"
This is the whole chapter in one string:
Wound types (1-2-3 intention)
Haemostasis (platelets, "Please Tell Every Visitor")
Abnormal healing factors (PIFPOM + OADPCILD)
Macrophages = masters of inflammation phase
Phases = H.I.P.R. (He Is Pretty Reliable)
Infection signs = PPEMWPIS
Remodelling = Type III→I, ~80% strength
TIMELINE CHEAT SHEET
| Time | Event |
|---|---|
| Minutes | Haemostasis: vasoconstriction, platelets, coagulation |
| 12 hours | Neutrophils arrive; basal keratinocyte mitosis begins |
| Day 2-3 | Macrophages arrive; fibroblasts begin to appear |
| Day 3 | Myofibroblasts appear (2nd intention healing); proliferative phase starts |
| Day 2-4 | Fibroblasts arrive, attracted by PDGF/TGF-β |
| Week 3 | Remodelling phase begins |
| 1 year+ | Remodelling completes, maximum ~80% tensile strength |
ONE-LINER STORY VERSION
"A wound happens. Platelets rush in and CALL the team (PDGF, TGF-β, EGF, VEGF). Neutrophils arrive FIRST to fight bacteria. Macrophages come next as supervisors. Fibroblasts roll in to BUILD the ECM scaffold. Keratinocytes march with lamellipodia to SEAL the surface. Type III collagen is laid down as a rough draft. Then slowly, over months, the editor (remodelling) replaces it with strong Type I collagen. The wound never fully returns to 100% - only 80%. That 20% is the scar's price."
This is the complete Chapter 10 of Scott-Brown's Vol. 1. All mnemonics, stories, and tables are drawn directly from the textbook. Good luck with your exam!
This is a shared conversation. Sign in to Orris to start your own chat.