Harrison 22 edition 131 pnemonia and 132 lung abscess
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from both chapters. Let me compile the full structured summary.
Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Chapter 131 - Pneumonia
Lionel A. Mandell, Michael S. Niederman
Definition
Pneumonia is infection of the pulmonary parenchyma. It is classified as:
- Community-acquired (CAP)
- Hospital-acquired (HAP)
- Ventilator-associated (VAP)
The former category "healthcare-associated pneumonia (HCAP)" has been discontinued - it did not reliably predict resistant pathogens and drove overuse of broad-spectrum antibiotics. Individual patient risk assessment is now preferred.
Aspiration pneumonia accounts for 5-15% of CAP cases and is best viewed as a continuum with CAP/HAP, not a separate category.
Pathophysiology
Pneumonia is not simply invasion of a sterile space. The lung has its own microbiota, and pneumonia is an emergent phenomenon from disruption of this homeostasis:
- An inflammatory trigger (often viral infection + microaspiration) causes epithelial/endothelial injury
- Released cytokines, chemokines, and catecholamines selectively promote growth of specific bacteria (e.g., S. pneumoniae, P. aeruginosa)
- A positive feedback loop forms: inflammation → nutrient availability → bacterial overgrowth → more inflammation
- If innate/adaptive immunity cannot contain this, full pneumonia develops
Key mediators:
- IL-6, TNF → fever
- IL-8, G-CSF → neutrophil recruitment
- Capillary leakage → alveolar edema (basis of infiltrate on imaging)
Community-Acquired Pneumonia (CAP)
Etiology
| Setting | Common Pathogens |
|---|---|
| Outpatient | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, respiratory viruses |
| Inpatient (non-ICU) | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, viruses, aspiration, Legionella |
| ICU | S. pneumoniae, S. aureus, Legionella, gram-negative rods, H. influenzae |
MRSA and P. aeruginosa are uncommon in typical CAP but must be considered in patients with prior respiratory isolates or recent hospitalization + antibiotics.
Clinical Diagnosis
- Requires: compatible symptoms (cough, sputum, fever, dyspnea) + new infiltrate on CXR
- Physical exam sensitivity/specificity: only ~58%/67%
- CT useful for: cavitation, loculated effusion, post-obstructive pneumonia
- Severity scores: PSI (Pneumonia Severity Index) and CURB-65 (Confusion, Urea >7, RR ≥30, BP <90/60, age ≥65) guide site-of-care decisions
Criteria for ICU admission (major criteria):
- Septic shock requiring vasopressors
- Respiratory failure requiring mechanical ventilation
Minor criteria (≥3 = severe): RR ≥30, PaO2/FiO2 ≤250, multilobar infiltrates, confusion, BUN ≥20, WBC <4,000, platelets <100,000, temp <36°C, hypotension requiring IV fluids.
Etiologic Diagnosis
- Sputum Gram stain/culture: recommended only for hospitalized patients, especially severe CAP or risk of MRSA/P. aeruginosa; valid specimen requires >25 neutrophils and <10 squamous cells per LPF
- Blood cultures: only 5-14% positive; most common isolate is S. pneumoniae
- Urinary antigens: S. pneumoniae (sensitive + specific) and Legionella (detects serogroup 1 only, ~80% of community cases)
- Procalcitonin: may help guide antibiotic duration (not initiation)
- Multiplex PCR panels: approved for respiratory pathogen detection
Treatment - CAP
Fig. 131-1 Algorithm: Assessment of MRSA/P. aeruginosa risk
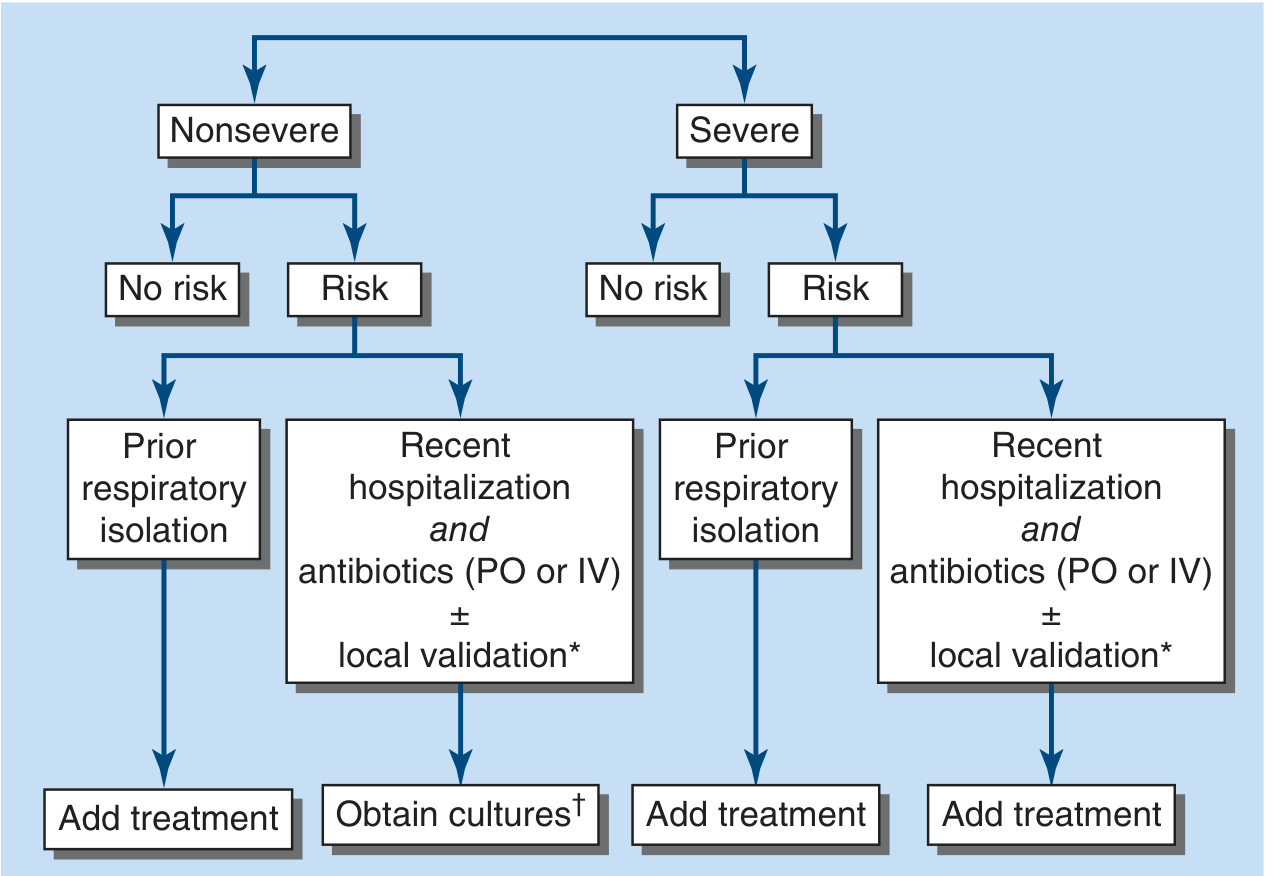
Outpatients (no comorbidities):
- Amoxicillin alone OR doxycycline (covers atypicals too)
Outpatients (with comorbidities - cardiac, pulmonary, renal, liver, DM, alcoholism, asplenia, malignancy):
- Respiratory fluoroquinolone (levofloxacin, moxifloxacin) OR
- Beta-lactam + macrolide
Inpatients (non-severe):
- Beta-lactam + macrolide OR respiratory fluoroquinolone
Inpatients (severe CAP - ICU):
- Beta-lactam + macrolide OR beta-lactam + respiratory fluoroquinolone
- If MRSA risk: add vancomycin or linezolid
- If P. aeruginosa risk: use anti-pseudomonal beta-lactam
Aspiration pneumonia: Routine anaerobic coverage is unnecessary unless poor dentition, lung abscess, or necrotizing pneumonia is present.
Duration: Typically 5 days for CAP (if clinical stability achieved and afebrile for 48-72h). Procalcitonin-guided protocols may shorten courses further.
Switch from IV to Oral
Criteria: improving cough/dyspnea, afebrile on ≥2 measurements 8h apart, WBC trending down, functioning GI tract, no concern for non-oral pathogens.
Failure to Respond
Consider: wrong diagnosis, resistant organism, unusual pathogen, non-infectious cause (PE, malignancy, vasculitis), empyema, metastatic infection. Repeat imaging and bronchoscopy as needed.
Antimicrobial Resistance
- Penicillin-resistant pneumococcus: MIC ≥2 µg/mL; respiratory fluoroquinolones, vancomycin, or linezolid for high-level resistance
- Macrolide-resistant M. pneumoniae: up to 95% in China, 5-13% in US/France; due to 23S rRNA domain V mutation
- ESBL gram-negatives: use carbapenem
Ventilator-Associated Pneumonia (VAP)
Epidemiology
- Affects 6-52% of ventilated patients; ~10% of ICU patients on any given day
- Highest hazard ratio in the first 5 days; cumulative rate up to 70% for patients ventilated ≥30 days
- COVID-19 has increased VAP frequency after years of decline
Pathogenesis (3 critical factors)
- Colonization of oropharynx with pathogens
- Aspiration into lower respiratory tract (microaspiration around cuff)
- Compromise of host defenses (immunoparalysis in sepsis/trauma)
The endotracheal tube is the most important risk factor: bypasses normal mechanical defenses, promotes biofilm formation on its surface, and microaspiration is worsened by secretions pooling above the cuff.
Clinical Manifestations
Nonspecific: fever, leukocytosis, increased secretions, pulmonary infiltrate, declining oxygenation. New or worsening infiltrate + ≥2 of: fever (>38°C) or hypothermia (<36°C), leukocytosis (>10,000) or leukopenia (<4,000), purulent secretions.
Diagnosis
- Clinical Pulmonary Infection Score (CPIS) adds sputum character, oxygenation, CXR, tracheal cultures to quantify likelihood
- Quantitative cultures (BAL >10⁴, mini-BAL >10⁴, protected brush >10³ CFU/mL): reduce antibiotic use but do not improve mortality vs. qualitative cultures
- Blood cultures usually negative (<15%)
Treatment
- Empirical broad-spectrum initially; de-escalate based on cultures at 48-72h
- Duration: 7-8 days (even for gram-negatives); short courses reduce resistance without increasing mortality
- For P. aeruginosa and Acinetobacter: combination not superior to monotherapy in non-neutropenic patients, but often used empirically
Prevention
- Avoid or minimize intubation duration - most effective strategy
- Elevate head of bed ≥30° (preferably 45°)
- Daily sedation holds + formal weaning protocols
- Subglottic secretion drainage via specialized endotracheal tubes
- Closed-suction catheter systems
- Ventilator circuits changed only when soiled, not on schedule
- Hand hygiene emphasized to reduce cross-infection
Hospital-Acquired Pneumonia (HAP)
- Similar to VAP but lower frequency of MDR pathogens (better outcomes)
- Anaerobes slightly more common (macroaspiration risk)
- Diagnosis harder: lower respiratory samples difficult to obtain from non-intubated patients
- Blood cultures positive in <15%
- Monotherapy feasible more often than in VAP
Chapter 132 - Lung Abscess
Rebecca M. Baron, Beverly W. Baron, Miriam Baron Barshak
Definition
Lung abscess = necrosis and cavitation of lung following microbial infection, usually a single dominant cavity >2 cm.
Classification
| Type | Details |
|---|---|
| Primary (~80%) | Aspiration-related, anaerobic bacteria, no underlying condition |
| Secondary (~20%) | Underlying condition (post-obstructive, immunocompromise, septic emboli) |
| Acute | <4-6 weeks duration |
| Chronic | ~40% of cases; >4-6 weeks |
Etiology and Microbiology (Table 132-1)
| Clinical Setting | Pathogens |
|---|---|
| Primary (aspiration) | Anaerobes (Peptostreptococcus, Prevotella, Bacteroides, milleri group streptococci), microaerophilic streptococci |
| Secondary (immunocompromised) | S. aureus, P. aeruginosa, Enterobacteriaceae, Nocardia, Aspergillus, Mucorales, Cryptococcus, Legionella, Rhodococcus equi, P. jirovecii |
| Septic emboli | S. aureus (endocarditis), Fusobacterium necrophorum (Lemierre's syndrome) |
| Endemic infections | M. tuberculosis, M. avium, M. kansasii, Coccidioides, Histoplasma capsulatum |
Key microbiology points:
- Primary abscesses often polymicrobial; no pathogen isolated in up to 40% (termed "nonspecific lung abscess")
- Putrid lung abscess (foul-smelling breath/sputum) = essentially diagnostic of anaerobic infection
- Right lung more commonly affected due to less angulated right mainstem bronchus
- Dependent segments most common location: posterior upper lobes and superior lower lobes
Epidemiology and Risk Factors
- Incidence decreased since antibiotic era
- Middle-aged men more commonly affected
- Major risk factor: aspiration
- High-risk patients: altered mental status, alcoholism, drug overdose, seizures, bulbar dysfunction, CVA, neuromuscular disease, esophageal dysmotility/lesions, GERD, recumbent position
- Gingivitis/periodontal disease critical: anaerobic colonization of gingival crevices + aspiration risk = abscess formation. Lung abscess is considered extremely rare in edentulous patients.
Historical note: The incidence dropped sharply in the late 1940s when oral surgery changed from seated (no ETT) to supine with cuffed ETT, and again when penicillin was introduced.
Pathology
- Lemierre's syndrome: pharyngeal infection (F. necrophorum) → septic thrombophlebitis of internal jugular vein → septic emboli → multiple lung abscesses
- Septic emboli from tricuspid valve endocarditis (IVDU + S. aureus)
Clinical Manifestations
- Acute presentation: fever, cough, sputum production, chest pain (similar to pneumonia initially)
- Chronic/indolent presentation: night sweats, fatigue, weight loss, hemoptysis (especially in secondary abscesses or those with underlying malignancy)
- Foul-smelling sputum = anaerobic etiology
- Chest exam: may reveal signs of consolidation or pleural effusion
- CXR/CT: cavity with air-fluid level is classic
Diagnosis
- CXR: cavity with air-fluid level, usually in dependent segments
- CT chest: better characterization of cavity, wall thickness, associated findings; helps exclude endobronchial lesion or malignancy
- Sputum Gram stain/culture (aerobic + anaerobic)
- Bronchoscopy (early): for patients with possible bronchial obstruction (foreign body, tumor), atypical presentation, or immunocompromised hosts
- CT-guided needle aspiration: in patients with risk factors for malignancy or atypical features
- Induced sputum for AFB: in patients from TB-endemic areas or with HIV risk factors
Approach:
- Low malignancy risk + aspiration risk factors → empirical treatment first, further workup if no response
- High malignancy risk or immunocompromised → early bronchoscopy + biopsy or CT-guided aspiration
Treatment
Medical therapy (mainstay):
- Amoxicillin-clavulanate or clindamycin (historically gold standard for anaerobes; but clindamycin now second-line due to C. diff risk)
- Beta-lactam/beta-lactamase inhibitors are first-line for anaerobic coverage
- Moxifloxacin has shown efficacy comparable to ampicillin-sulbactam in aspiration pneumonia/primary lung abscess
- Duration: prolonged - typically 3-6 weeks or until radiographic resolution (cavity closure or small stable residual lesion)
- Secondary abscesses: culture-directed therapy essential
Drainage:
- Most primary abscesses drain spontaneously via the tracheobronchial tree
- Percutaneous catheter drainage: indicated for abscesses not responding to medical therapy; a systematic review (Lee et al, 2022) supported this approach
- Bronchoscopic drainage: useful when associated with obstructing lesion
- Surgical resection (lobectomy): reserved for failure of medical/percutaneous therapy, complications (massive hemoptysis, bronchopleural fistula), or when malignancy cannot be excluded
Complications
- Pneumatoceles or bronchiectasis (persistent cystic changes, especially with large cavities)
- Empyema (extension to pleural space)
- Life-threatening hemoptysis
- Massive aspiration of abscess contents
Prognosis
| Type | Mortality |
|---|---|
| Primary abscess | As low as 2% |
| Secondary abscess | Up to 75% (case series) |
Poor prognostic factors:
- Age >60
- Malignancy-related abscess
- Aerobic bacteria as cause
- Sepsis at presentation
- Symptom duration >8 weeks
- Abscess size >6 cm
Prevention
- Airway protection in at-risk patients
- Oral hygiene (treat periodontal disease)
- Minimize sedation; elevate head of bed
- Antimicrobial prophylaxis in highly immunocompromised patients (BMT, solid organ transplant, advanced HIV)
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill Medical) - Chapters 131 and 132
This is a shared conversation. Sign in to Orris to start your own chat.