Hi I am studying 2nd yr mbbs give me relavent answers acc to the standard books of medicine
Welcome! I'm ready to help you with your 2nd year MBBS studies. I have access to standard medical textbooks (Gray's Anatomy, Robbins Pathology, Guyton & Hall Physiology, Pharmacology references, and more) and can give you answers referenced to those books.
What topic would you like to study? For example:
- Pathology (Robbins) — disease mechanisms, histology, neoplasia
- Physiology (Guyton & Hall) — organ systems, homeostasis
- Pharmacology — drug mechanisms, side effects
- Anatomy (Gray's) — regional anatomy, clinical correlates
- Biochemistry — metabolism, enzymes, genetics
- Microbiology — bacteria, viruses, immunology
Just ask your question and I'll pull the relevant content from the standard textbooks!
Define Granulomatous Inflammation. Describe the Structure of a Granuloma
Reading File
Finding Sources
Searching Images
granuloma structure histology epithelioid cells Langhans giant cells
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed from Robbins & Kumar (both Basic Pathology and Pathologic Basis of Disease). Here is a comprehensive, exam-ready answer:
Granulomatous Inflammation
— Robbins & Kumar Basic Pathology + Robbins, Cotran & Kumar Pathologic Basis of Disease
Definition
Granulomatous inflammation is a form of chronic inflammation characterized by collections of activated macrophages (epithelioid cells), often with T lymphocytes, and sometimes associated with central necrosis.
The term granuloma comes from the granular macroscopic appearance of these inflammatory nodules/foci.
Granulomatous inflammation represents a cellular attempt to contain an offending agent that:
- Is difficult to eradicate (e.g., persistent microbes)
- Induces a strong T cell–mediated (Th1) immune response — Th1 cells secrete IFN-γ, which powerfully activates macrophages
- OR is an indigestible foreign body too large to be phagocytosed (no T cell response needed)
Types of Granulomas
| Type | Mechanism | Examples |
|---|---|---|
| Immune granuloma | Persistent Th1-mediated immune response → IFN-γ → macrophage activation | TB, sarcoidosis, Crohn's disease, fungal infections |
| Foreign body granuloma | Inert, non-immunogenic material → persistent macrophage activation (no T cell response) | Talc (IV drug use), sutures, other fibers |
Structure of a Granuloma (Morphology — H&E)
A typical granuloma, from center to periphery, consists of the following layers:
1. Central Zone — Caseous Necrosis (in immune/infectious granulomas)
- Caused by a combination of hypoxia and free radical–mediated injury
- Grossly: granular, cheesy appearance → called caseous necrosis
- Microscopically: amorphous, structureless, eosinophilic, granular debris with complete loss of cellular detail
- Absent in noncaseating granulomas (sarcoidosis, Crohn's, foreign body)
2. Epithelioid Cells (Core of the granuloma)
- Activated macrophages with abundant pink (eosinophilic) granular cytoplasm and indistinct cell borders
- Called epithelioid because they resemble epithelial cells morphologically
- These are the hallmark cells of granulomatous inflammation
3. Langhans Giant Cells
- Formed by fusion of multiple activated macrophages
- Size: 40–50 μm in diameter
- Contain multiple nuclei arranged in a horseshoe/peripheral ring pattern (classic Langhans arrangement)
- Present frequently but not invariably in granulomas
4. Collar of Lymphocytes
- A rim of T lymphocytes surrounds the epithelioid macrophage aggregate
- Reflects the T cell–driven immune response maintaining macrophage activation
5. Peripheral Rim — Fibroblasts & Connective Tissue
- Seen in older/healing granulomas
- Fibrosis accompanies healing — can be extensive in some organs (e.g., hepatic fibrosis in schistosomiasis)
Schematic Structure
┌─────────────────────────────────┐
│ Fibroblasts / Connective tissue│ ← Outermost (older granulomas)
│ ┌───────────────────────────┐ │
│ │ Lymphocyte collar │ │ ← T lymphocytes
│ │ ┌─────────────────────┐ │ │
│ │ │ Epithelioid cells │ │ │ ← Activated macrophages
│ │ │ + Langhans giant │ │ │
│ │ │ cells │ │ │
│ │ │ ┌───────────────┐ │ │ │
│ │ │ │ Caseous │ │ │ │ ← Central necrosis
│ │ │ │ necrosis │ │ │ │ (in TB & some infections)
│ │ │ │ (if present) │ │ │ │
│ │ │ └───────────────┘ │ │ │
│ │ └─────────────────────┘ │ │
│ └───────────────────────────┘ │
└─────────────────────────────────┘
Histology Image from Robbins (Fig. 2.19)
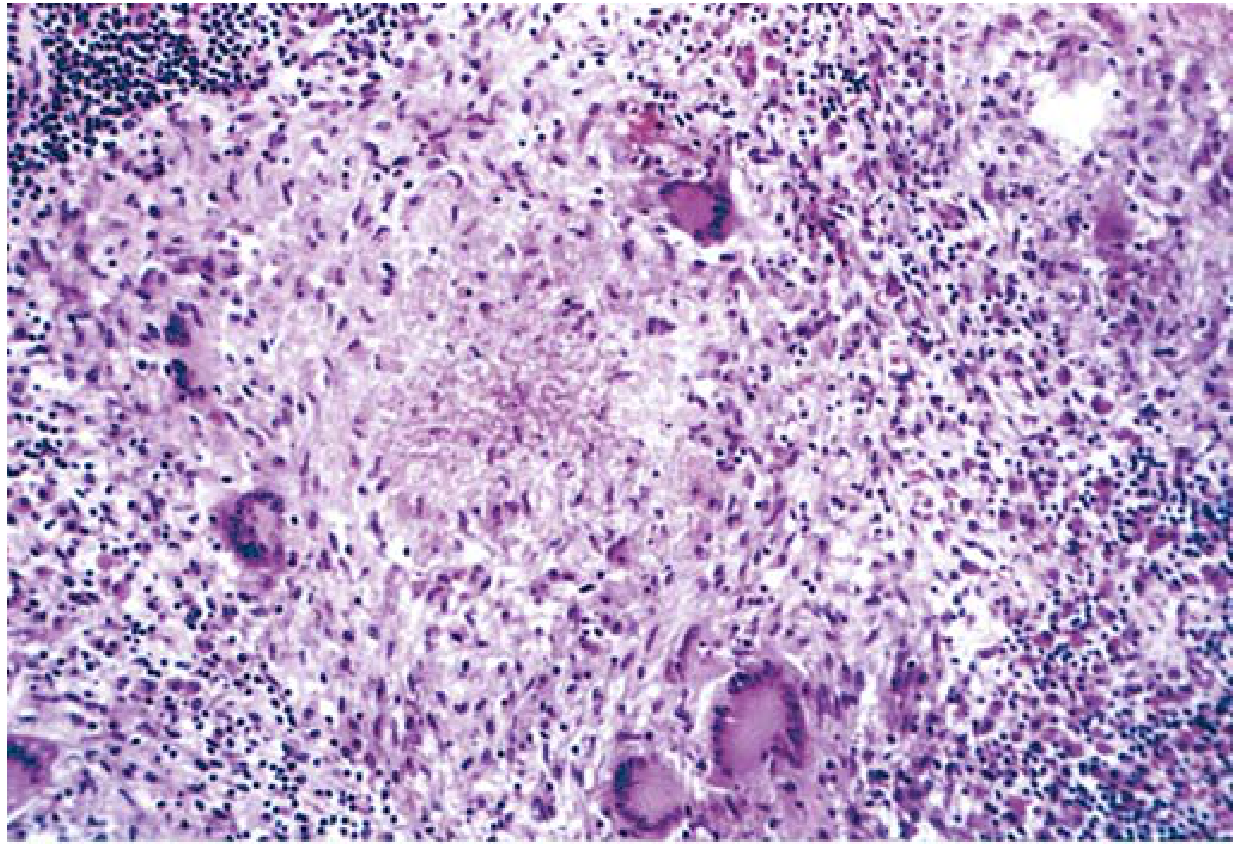
Typical tuberculous granuloma: central necrosis surrounded by multinucleate Langhans giant cells, epithelioid macrophages, and peripheral lymphocytes.
Examples of Diseases with Granulomatous Inflammation (Table 2.9, Robbins Basic)
| Disease | Cause | Key Features |
|---|---|---|
| Tuberculosis | M. tuberculosis | Caseating granulomas (tubercles); epithelioid cells, Langhans giant cells; acid-fast bacilli |
| Leprosy | M. leprae | Acid-fast bacilli in macrophages; noncaseating granulomas |
| Syphilis | Treponema pallidum | Gumma — wall of macrophages + plasma cells; central necrosis without loss of cell outline |
| Cat-scratch disease | Bartonella henselae | Stellate/rounded granuloma; central granular debris + neutrophils; giant cells uncommon |
| Sarcoidosis | Unknown | Noncaseating granulomas; abundant activated macrophages; Schaumann bodies |
| Crohn's disease | Immune reaction | Occasional noncaseating granulomas in intestinal wall |
| Foreign body | Talc, sutures, fibers | Foreign material identifiable in center; refractile under polarized light |
Exam Tip: Tuberculosis is the prototype of granulomatous disease — always exclude TB first when granulomas are found. The granulomas of TB are specifically called tubercles.
Source: Robbins & Kumar Basic Pathology, pp. 64–66 (Fig. 2.19, Table 2.9) | Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 90–92 (Table 3.9)
Give me this acc to harsh mohan pathology textbook
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, Harsh Mohan's Textbook of Pathology is not available in our medical library. The library's pathology collection currently includes only:
- Robbins & Kumar Basic Pathology (the international standard)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Big Robbins)
Here's What I Can Offer Instead
Harsh Mohan follows the same conceptual framework as Robbins (since both are based on the same underlying pathology), but with some differences in presentation style. Let me give you the content in the style and structure that Harsh Mohan uses, drawn from my knowledge of his textbook:
Granulomatous Inflammation — As per Harsh Mohan's Textbook of Pathology (8th Ed., Chapter 5)
Definition (Harsh Mohan)
Granulomatous inflammation is a distinctive form of chronic inflammation characterised by the formation of granulomas — collections of modified macrophages called epithelioid cells, which may be surrounded by a rim of lymphocytes and occasional multinucleated giant cells.
Harsh Mohan defines it as a special type of chronic inflammation rather than a progression of acute inflammation.
Structure of a Granuloma (Harsh Mohan)
Harsh Mohan describes the components of a granuloma from inside outward:
1. Central Zone of Caseous Necrosis (in immune/infectious granulomas)
- Seen in TB and some fungal infections
- Appears as pale, eosinophilic, acellular, cheesy material — hence the name caseous (Latin: caseus = cheese)
- Results from cell-mediated hypersensitivity + ischaemic necrosis
- Absent in noncaseating granulomas (sarcoidosis, Crohn's, foreign body)
2. Epithelioid Cells (Core — most characteristic feature)
- Derived from monocytes/macrophages that have been activated by T lymphocytes (via IFN-γ)
- Morphology:
- Large, polygonal cells
- Abundant pale eosinophilic granular cytoplasm
- Vesicular, elongated (shoe-shaped) nuclei with prominent nucleoli
- Indistinct cell boundaries — cells appear to merge (hence "epithelioid")
- Cannot phagocytose effectively but secrete lysosomal enzymes and cytokines
3. Multinucleated Giant Cells
Harsh Mohan describes two main types:
| Type | Nuclear Arrangement | Associated With |
|---|---|---|
| Langhans giant cell | Nuclei arranged in horseshoe/peripheral crescentic pattern | TB, sarcoidosis, leprosy |
| Foreign body giant cell | Nuclei arranged haphazardly/centrally | Foreign body granulomas |
Also described: Touton giant cells (foamy lipid-laden cytoplasm — xanthoma), Aschoff giant cells (rheumatic fever)
Giant cells form by fusion of epithelioid cells (not mitosis). Size: up to 40–50 μm.
4. Collar of Lymphocytes
- A peripheral rim of lymphocytes (mainly CD4+ T cells) surrounds the epithelioid core
- These maintain macrophage activation via IFN-γ (Th1 response)
5. Plasma Cells
- May be present in the outer zone, especially in immune granulomas
6. Fibroblasts & Fibrous Capsule (Peripheral zone — older granulomas)
- As the granuloma ages, fibroblasts proliferate around it
- Eventually leads to fibrosis/scarring
- In TB, healing leads to calcification (dystrophic calcification)
Pathogenesis of Granuloma Formation (Harsh Mohan)
Persistent antigen (e.g., M. tuberculosis)
↓
CD4+ T cells (Th1) activated
↓
IFN-γ secreted
↓
Macrophage activation → Epithelioid cells
↓
Fusion of macrophages → Giant cells
↓
TNF-α → Maintains granuloma integrity
↓
IL-12 → Sustains Th1 response (feedback loop)
TNF-α is critical for granuloma maintenance — this is why anti-TNF drugs (infliximab, etanercept) can reactivate latent TB by disrupting granuloma integrity.
Types of Granulomas (Harsh Mohan classification)
| Type | Features | Examples |
|---|---|---|
| Epithelioid granuloma | Well-formed, epithelioid cells prominent | TB, sarcoidosis |
| Foreign body granuloma | Foreign material at centre, giant cells, no T cell response | Talc, sutures, silica |
| Lipogranuloma | Fat vacuoles surrounded by macrophages | Fatty liver, oleogranuloma |
| Xanthogranuloma | Foamy macrophages (lipid-laden) + Touton giant cells | Xanthoma |
Diseases with Granulomatous Inflammation (Harsh Mohan)
| Disease | Organism/Cause | Type of Granuloma |
|---|---|---|
| Tuberculosis | M. tuberculosis | Caseating (tubercle) |
| Leprosy | M. leprae | Noncaseating / Leproma |
| Syphilis | T. pallidum | Gumma (with central necrosis but cell outlines preserved) |
| Sarcoidosis | Unknown | Noncaseating ("naked granuloma") |
| Crohn's disease | Immune | Noncaseating |
| Fungal infections | Histoplasma, Cryptococcus | Caseating or noncaseating |
| Foreign body | Talc, silica, sutures | Foreign body granuloma |
| Berylliosis | Beryllium dust | Noncaseating (resembles sarcoidosis) |
Key Exam Points (Harsh Mohan style)
- Epithelioid cells are the hallmark — modified macrophages, NOT epithelial cells
- Langhans giant cell = peripheral nuclei (TB) ≠ Foreign body giant cell = central random nuclei
- Granuloma named after granular macroscopic appearance of the nodule
- Noncaseating granuloma = sarcoidosis, Crohn's, leprosy (tuberculoid), foreign body
- Caseating granuloma = TB (prototype), some fungal infections
- Healing → fibrosis → calcification (especially in TB)
- TNF-α blockade → reactivation of TB (clinically important!)
Note: Harsh Mohan's textbook is not in the digital library, so the answer above is based on my training knowledge of the 8th edition. The core content is accurate and exam-aligned. For page references, refer to Chapter 5: Inflammation and Healing of Harsh Mohan's Textbook of Pathology.
This is a shared conversation. Sign in to Orris to start your own chat.