Hi
Explain me parkosnsesom
"Parkinsonism" AND "review"
Parkinsonism
What Is It?
| Feature | Description |
|---|---|
| Tremor | Resting "pill-rolling" tremor, typically 4-6 Hz, reduces with movement |
| Rigidity | "Lead-pipe" or "cogwheel" stiffness of muscles |
| Akinesia/Bradykinesia | Slowness and poverty of movement |
| Postural instability | Loss of balance reflexes, tendency to fall |
- Flexed posture - stooped, forward-bent stance
- Freezing - sudden motor blocks, especially when initiating movement or turning
Pathology - What Goes Wrong in the Brain
- Degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNc) - the dark-pigmented area of the midbrain. Motor symptoms appear once >40% of these neurons are lost.
- Reduced striatal dopamine - dopamine normally facilitates smooth, coordinated movement via the nigrostriatal pathway.
- Lewy bodies - abnormal protein clumps of alpha-synuclein that accumulate inside neurons and are the pathological hallmark.
- Cholinergic neurons (nucleus basalis of Meynert) - causing dementia
- Norepinephrine neurons (locus coeruleus)
- Serotonin neurons (raphe nuclei)
- Peripheral autonomic nervous system - causing non-motor features
Causes of Parkinsonism
1. Primary/Idiopathic
- Parkinson's Disease (PD) - most common; cause often unknown
- Genetic mutations: SNCA, LRRK2, PINK1, Parkin (PARK2) genes
2. "Parkinsonism-Plus" (Atypical Parkinsonism)
| Condition | Key Extra Features |
|---|---|
| Progressive Supranuclear Palsy (PSP) | Gaze palsy, early falls, dementia |
| Multiple System Atrophy (MSA) | Dysautonomia, ataxia |
| Corticobasal Syndrome (CBS) | Limb apraxia, alien limb |
| Dementia with Lewy Bodies (DLB) | Early dementia, hallucinations |
3. Secondary Parkinsonism
- Drug-induced - antipsychotics (D2 receptor blockade), metoclopramide, reserpine (most common reversible cause)
- Vascular - multi-infarct disease ("lower-body parkinsonism")
- Toxins - MPTP, manganese, carbon monoxide
- Post-encephalitic
- Trauma - pugilistic encephalopathy (boxers)
- Structural - normal pressure hydrocephalus, brain tumors
Motor Features in Detail
Early Signs (often missed)
- Reduced arm swing while walking
- Facial masking (reduced expression, misread as depression)
- Micrographia (small handwriting)
- Soft voice (hypophonia)
- Painful/frozen shoulder
Classic Signs
- Shuffling gait with short steps
- Difficulty initiating movement (freezing)
- Stooped forward posture
- Reduced eye blinking
- Drooling
Late Signs
- Severe postural instability - frequent falls
- Dysphagia
- Dysarthria
Non-Motor Features
- Anosmia (loss of smell) - often one of the earliest signs
- REM sleep behavior disorder (RBD) - acting out dreams
- Autonomic dysfunction - orthostatic hypotension, constipation, urinary problems, sexual dysfunction
- Depression and anxiety
- Cognitive impairment/dementia (later stages)
- Pain and sensory disturbances
Diagnosis
- Presence of TRAP features
- Response to levodopa (supports PD diagnosis)
- Exclusion of secondary causes
- Dopamine imaging (DaTscan) to confirm dopamine neuron loss
Treatment
Dopaminergic Therapies (main approach)
- Levodopa + Carbidopa - gold standard; carbidopa prevents peripheral conversion
- Dopamine agonists (pramipexole, ropinirole) - used especially in younger patients
- MAO-B inhibitors (selegiline, rasagiline) - slow dopamine breakdown
- COMT inhibitors (entacapone) - extend levodopa effect
- Amantadine - treats both parkinsonism and dyskinesias
Non-Dopaminergic / Symptomatic
- Anticholinergics (benztropine, trihexyphenidyl) - useful for tremor, but cause confusion in elderly
- Deep Brain Stimulation (DBS) - surgical option for advanced PD
Drug-Induced Parkinsonism
- Stop or reduce the offending drug (antipsychotic, metoclopramide)
- Symptoms are often reversible
Key Differential Points
| Feature | PD | Drug-Induced | MSA | PSP |
|---|---|---|---|---|
| Tremor | Yes (rest) | Yes | Mild/absent | Absent |
| L-dopa response | Good | Variable | Poor | Poor |
| Symmetry | Asymmetric | Often symmetric | Symmetric | Symmetric |
| Autonomic features | Mild | No | Prominent | Mild |
| Dementia | Late | No | Mild | Yes |
- Harrison's Principles of Internal Medicine, 22nd Ed., Chapter 446 - Parkinson's Disease and Related Disorders
- Bradley and Daroff's Neurology in Clinical Practice - Chapter 24: Parkinsonism
- Katzung's Basic and Clinical Pharmacology, 16th Ed. - Pathogenesis of PD
- Recent review: Drug-induced parkinsonism: diagnosis and treatment (Conn & Jankovic, 2024)
Can i give me my anfo to help u while giving me amswers
- Who you are - e.g., medical student, nurse, doctor, patient, curious learner
- Your level - beginner, intermediate, advanced/professional
- Your field or specialty - e.g., neurology, pharmacy, general medicine
- Your purpose - studying for an exam, clinical practice, personal health question
- Your preferences - do you want simple explanations or detailed clinical depth?
My personal answer instructions are: 1. Language Style: Use simple English words that are easy to understand. Write full sentences like a human, not short phrases. Keep explanation at GNM 2nd year level. 2. Writing Format (Exam Style): Always follow proper nursing headings: Introduction, Definition, Causes (5 points only), Types/Stages (if applicable), Symptoms (5 points only), dignostic evaluvation , Management (Medical, Pharmacological, Nursing, Pre-operative care (if needed), Post-operative care (if needed)), Health Education, Conclusion. 3. Point Writing Style: Each point should have a Heading + full sentence explanation. 4. Medical Terms Rule: Always use medical terms with meaning in brackets. 5. Image Rule: Give images in every section. Images should help in understanding (diagram, clinical picture, etc.). 6. Video Rule: Give 1 YouTube video at the end for better understanding. 7. Content Style: Use scientific and correct information. Make answers suitable for writing in exams. Avoid wrong or incomplete points. 8. Structure Preference: Write point-wise (not paragraph) except Introduction & Definition. Keep answers clear, neat, and easy to revise
📋 Your Answer Format - Confirmed
| Setting | Your Preference |
|---|---|
| Language | Simple English, full sentences, GNM 2nd year level |
| Format | Exam-style with proper nursing headings |
| Headings | Introduction → Definition → Causes → Types/Stages → Symptoms → Diagnostic Evaluation → Management → Health Education → Conclusion |
| Point Style | Heading + full sentence explanation |
| Medical Terms | Always with meaning in brackets |
| Images | In every section |
| Video | 1 YouTube video at the end |
| Content | Scientific, correct, exam-ready |
| Structure | Point-wise (except Intro & Definition) |
Ccf
congestive cardiac failure CCF nursing management symptoms diagnosis
CCF congestive cardiac failure nursing health education YouTube video explanation
Congestive Cardiac Failure (CCF)
1. Introduction

2. Definition
"Heart failure is a complex clinical syndrome that results from structural or functional impairment of ventricular filling or ejection of blood."
- Braunwald's Heart Disease, Textbook of Cardiovascular Medicine
3. Causes

4. Types / Classification
A. Based on Side of the Heart Affected
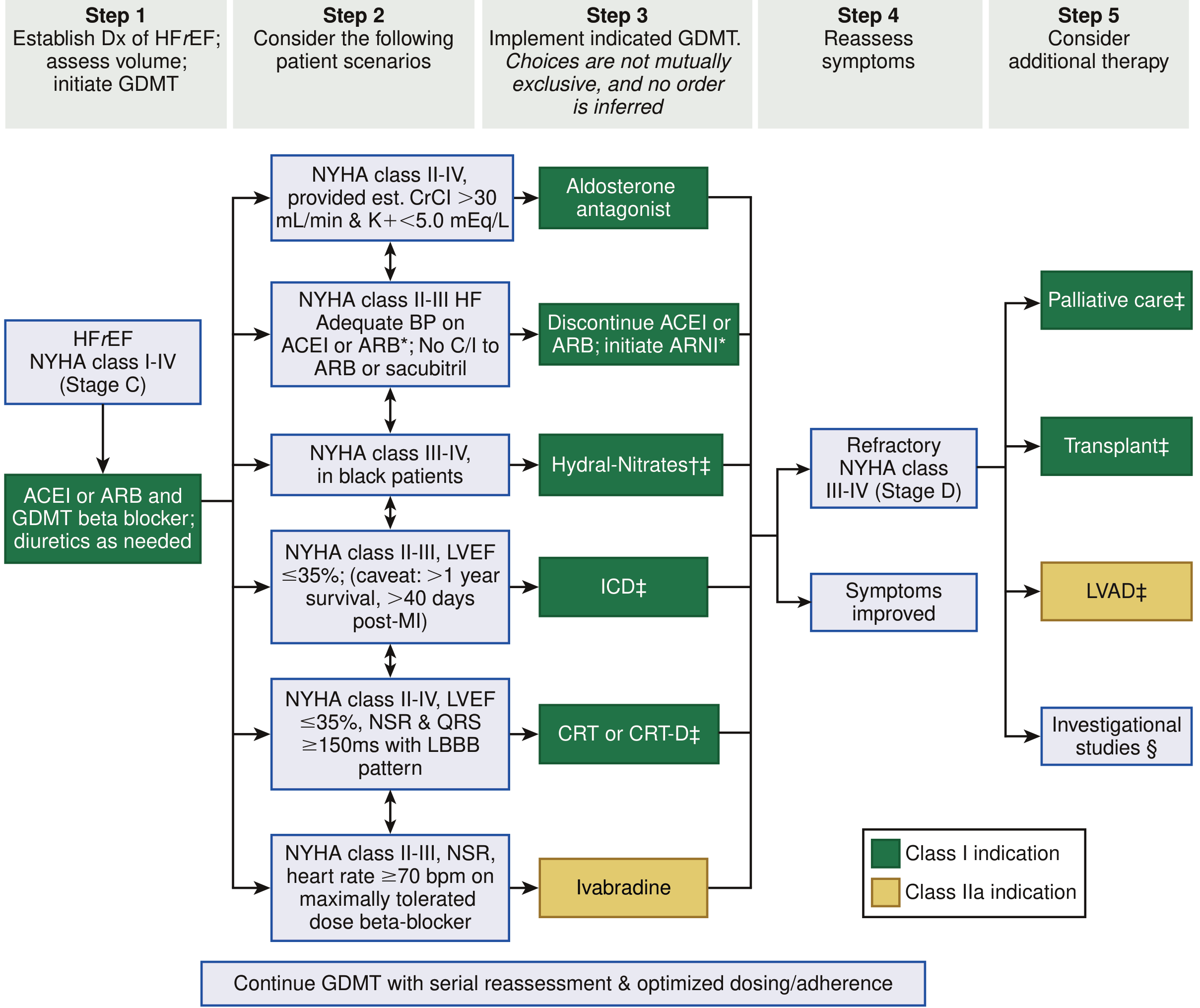
B. NYHA Functional Classification (New York Heart Association)
| NYHA Class | Description |
|---|---|
| Class I | No symptoms during ordinary activity |
| Class II | Slight limitation - symptoms with ordinary activity |
| Class III | Marked limitation - symptoms with less than ordinary activity |
| Class IV | Symptoms at rest - unable to do any activity |
C. Based on Pumping Function
| Type | Meaning |
|---|---|
| Systolic (HFrEF) | Heart cannot squeeze (contract) properly - Ejection Fraction (EF) is low |
| Diastolic (HFpEF) | Heart cannot relax and fill properly - EF is preserved (normal) |
5. Signs and Symptoms
Other symptoms include: cough (especially at night), jugular venous distension (JVD), weight gain, reduced urine output (oliguria), and cold extremities.

6. Diagnostic Evaluation
- Blood tests: Complete Blood Count (CBC), kidney function tests (serum creatinine, urea), liver function tests, electrolytes (sodium, potassium)
- Coronary Angiography: To check for blocked coronary arteries
- Cardiac MRI: For detailed heart structure assessment
7. Management
A. Medical Management
B. Pharmacological Management
- Example: Furosemide (Lasix)
- Diuretics increase urine output, removing excess fluid from the body and reducing congestion in the lungs and legs. They give quick relief from breathlessness and edema.
- Example: Enalapril, Ramipril
- ACE inhibitors relax and widen blood vessels, reducing the workload on the heart. They also prevent further damage to the heart muscle and reduce mortality (death) in CCF patients.
- Example: Carvedilol, Metoprolol
- Beta-blockers reduce the heart rate and blood pressure, decreasing the heart's workload. They improve the heart's pumping function over time and reduce the risk of sudden cardiac death.
- Digoxin strengthens the contractions of the heart muscle (positive inotropic effect), helping the heart pump more effectively. It is also used to control the heart rate in patients with atrial fibrillation (irregular heartbeat).
- Spironolactone is a potassium-sparing diuretic that also reduces fluid retention. It prevents harmful changes in the heart muscle (cardiac remodeling) and is used in moderate to severe CCF.
C. Nursing Management
D. Surgical Management (Advanced Cases)
8. Health Education
9. Conclusion
📹 Watch This Video for Better Understanding
Sources: Braunwald's Heart Disease (Textbook of Cardiovascular Medicine) | Fuster and Hurst's The Heart, 15th Edition | Harrison's Principles of Internal Medicine 22nd Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics
Can you make it short?This question is only 5 marks
Congestive Cardiac Failure (CCF)
Introduction & Definition
Causes (5 Points)
Symptoms (5 Points)
Management (Brief)
- Semi-Fowler's position to ease breathing
- Oxygen therapy to maintain SpO2 above 94%
- Sodium and fluid restriction in diet
- Diuretics (Furosemide) - removes extra fluid
- ACE Inhibitors (Enalapril) - reduces heart workload
- Digoxin - strengthens heart contractions
- Monitor vital signs and oxygen saturation
- Maintain strict Intake-Output (I/O) chart
- Daily weight monitoring - report gain of more than 1 kg