Now I have solid foundational results. Let me compile the full comprehensive answer from my medical knowledge, supplemented by these sources.
🔪 NEPHRECTOMY — The Complete Master Guide
Easy Memory Hook: Think of nephrectomy types by HOW MUCH kidney is removed and WHY
- Radical = Remove ALL + surroundings (Cancer, aggressive)
- Simple = Remove ALL kidney only (Benign disease)
- Partial = Remove PART of kidney (Small tumors, save nephrons)
- Donor = Remove healthy kidney to GIVE to someone else
🧠 THE BIG PICTURE — ONE-LINER EACH
| Type | Nickname | What's Removed | Why Done |
|---|
| Radical | "The Big One" | Kidney + Gerota's fascia + adrenal + lymph nodes ± IVC thrombus | Renal cell carcinoma |
| Simple | "Clean Sweep" | Kidney only (within Gerota's fascia) | Benign non-functioning kidney |
| Partial | "Kidney Sparing" | Only the tumor + margin | Small RCC, solitary kidney, bilateral tumors |
| Donor | "Gift Surgery" | Healthy kidney for transplant | Living kidney donation |
1️⃣ RADICAL NEPHRECTOMY
🎯 Definition
Removal of the entire kidney along with Gerota's fascia, ipsilateral adrenal gland, and regional lymph nodes — all in one en-bloc resection.
✅ Indications
- Renal cell carcinoma (RCC) — primary indication
- Large tumors (>7 cm, T2 stage)
- Tumor invading adrenal or perinephric fat
- Renal vein / IVC thrombus (extended radical)
- When partial nephrectomy is not feasible
🗂️ Types of Radical Nephrectomy
| Type | Details |
|---|
| Open Radical | Flank, transperitoneal, or thoracoabdominal incision |
| Laparoscopic Radical | Most common today; ports-based; faster recovery |
| Robotic-Assisted Radical | Robotic platform; complex cases |
| Hand-Assisted Laparoscopic | Surgeon's hand inside through small incision |
| Extended Radical | + IVC thrombectomy, + contralateral LN dissection |
📐 Surgical Approaches
| Approach | When Used |
|---|
| Flank (retroperitoneal) | Most common open approach |
| Transperitoneal | Large tumors, IVC involvement |
| Thoracoabdominal | Upper pole tumors, T3b/T4 |
🔑 Key Clinical Points
- Gerota's fascia must be kept intact — do NOT breach it (prevents tumor spillage)
- Adrenal spared if imaging shows normal adrenal + upper pole tumor not involved
- Renal vein secured FIRST before artery (prevents renal engorgement)
Actually: Artery ligated FIRST → then vein → prevents venous engorgement
- IVC thrombus levels (Neves classification):
- Level I: Infrarenal IVC
- Level II: Infrahepatic IVC
- Level III: Retrohepatic IVC
- Level IV: Supradiaphragmatic (requires cardiopulmonary bypass)
- Lymph node dissection is staging, not always therapeutic
2️⃣ SIMPLE NEPHRECTOMY
🎯 Definition
Removal of the kidney alone, within or outside Gerota's fascia, without adrenal or lymph node dissection.
✅ Indications (Benign — remember "CHPTR")
- Chronic pyelonephritis / xanthogranulomatous pyelonephritis
- Hydronephrosis (non-functioning kidney)
- Pyonephrosis
- Trauma (irreparable kidney)
- Renovascular hypertension (non-correctable stenosis)
- Also: Renal TB, polycystic kidney disease, calculus disease with destruction
🗂️ Types of Simple Nephrectomy
| Type | Details |
|---|
| Open Simple | Flank approach most common |
| Laparoscopic Simple | Standard of care for most benign cases |
| Retroperitoneoscopic | Retroperitoneal laparoscopic; less bowel handling |
| Subcapsular | Removes kidney within its capsule; used in dense adhesions (e.g., xanthogranulomatous pyelonephritis) |
🔑 Key Clinical Points
- Subcapsular nephrectomy = capsule left behind; used when perirenal adhesions make dissection dangerous
- No need to remove adrenal gland or lymph nodes
- Gerota's fascia may be left — no oncologic concern
- Always confirm contralateral kidney function beforehand
- In xanthogranulomatous pyelonephritis: classic "bear paw" on CT; subcapsular approach preferred due to dense adhesions
3️⃣ PARTIAL NEPHRECTOMY (Nephron-Sparing Surgery)
🎯 Definition
Removal of only the tumor with a surrounding margin of normal parenchyma, preserving maximum functioning kidney tissue.
✅ Indications — Absolute vs Relative vs Elective
| Category | Examples |
|---|
| Absolute (must do) | Solitary kidney, bilateral RCC, hereditary RCC (VHL), CKD/renal insufficiency |
| Relative (should consider) | Contralateral kidney with disease (stones, HTN, DM) |
| Elective (can do) | Normal contralateral kidney + tumor ≤4 cm (T1a) |
🗂️ Types of Partial Nephrectomy
| Type | Details |
|---|
| Open Partial | Gold standard for complex/hilar tumors |
| Laparoscopic Partial | Technically demanding; for peripheral tumors |
| Robotic-Assisted Partial (RALPN) | Most commonly used minimally invasive approach today |
| Polar nephrectomy | Removal of entire upper or lower pole |
| Wedge resection | Excision of tumor with wedge of parenchyma |
| Transverse resection | For tumors at the midportion |
🔑 Key Clinical Points — The "Trifecta" Goal
Trifecta of Partial Nephrectomy:
- Negative surgical margins (no tumor at cut edge)
- No urologic complications (urine leak, fistula)
- Preserved renal function (warm ischemia <25 min)
- Warm ischemia time (WIT): Keep <25 minutes — prolonged WIT = nephron loss
- Cold ischemia: Ice slush used in open surgery if WIT expected >30 min
- RENAL nephrometry score guides complexity:
- R = Radius (size)
- E = Exophytic/endophytic
- N = Nearness to collecting system
- A = Anterior/posterior
- L = Location (polar line)
- Renorrhaphy (closing the kidney) — use bolster sutures
- Urine leak is the most common complication (1–7%)
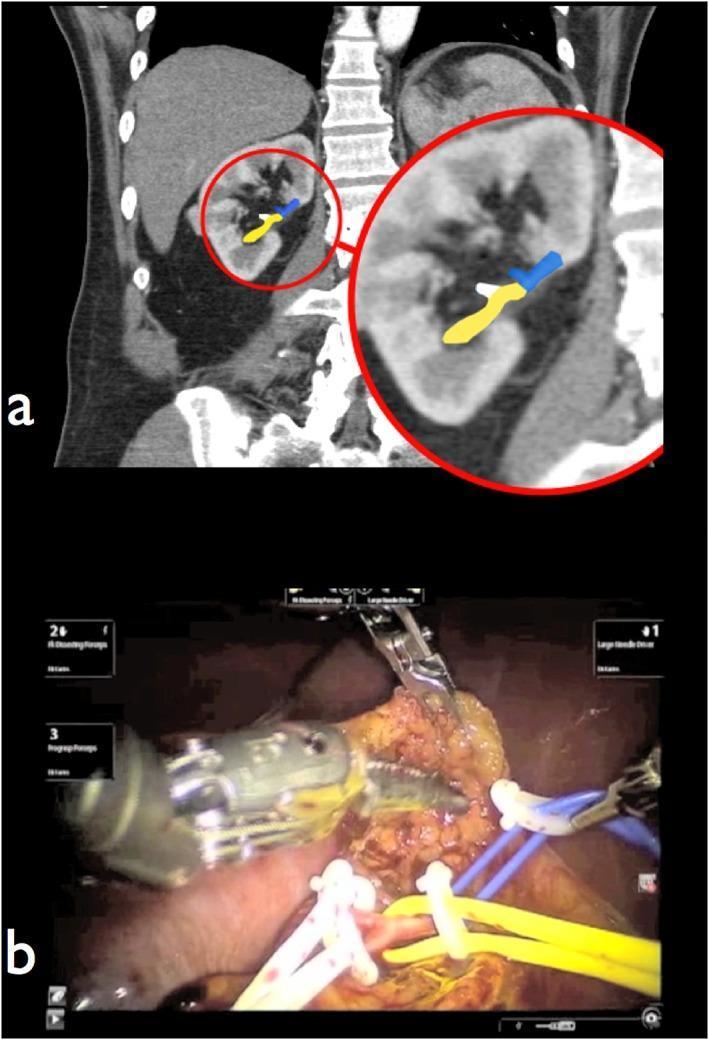
- Robotic partial nephrectomy = CT angiography beforehand for vascular mapping (as shown below)
Preoperative CT angiography arterial roadmap (a) translated to intraoperative robotic field (b) — primary artery in blue, secondary in yellow, tertiary in white. This selective clamping minimizes ischemic injury during tumor excision.
4️⃣ DONOR NEPHRECTOMY
🎯 Definition
Removal of a healthy kidney from a living donor for transplantation to a recipient with end-stage renal disease.
✅ Indications
- Living related donor (LRD) — blood relative
- Living unrelated donor (LURD) — emotionally related (spouse, friend)
- Altruistic/anonymous donor
🗂️ Types of Donor Nephrectomy
| Type | Details |
|---|
| Open Donor Nephrectomy | Flank or midline; historical standard |
| Laparoscopic Donor Nephrectomy (LDN) | Standard of care; faster donor recovery |
| Hand-Assisted Laparoscopic (HALDN) | Surgeon's hand-port; optimal approach per guidelines |
| Mini-open Laparoscopy | Small incision; good outcomes |
| Retroperitoneoscopic Donor | Less common; for right side |
| Robotic Donor | Generally NOT recommended (guideline recommendation) |
🔑 Key Clinical Points (per Living Kidney Donors Guidelines, p.90)
- LEFT kidney preferred over right — longer renal vein = easier anastomosis for recipient
- Right kidney taken if: vascular anomaly on left, fibromuscular dysplasia, left is smaller
- Renal artery must be transfixed by suture ligature or anchor staple — NOT with nontransfixing clips (Weck Hem-o-lok clips are CONTRAINDICATED for renal artery)
- CT angiography mandatory before any donor nephrectomy (anatomy assessment)
- 3+ renal arteries → only experienced surgeon should operate
- Contraindications to donation:
- Atherosclerotic disease of both renal artery orifices
- Fibromuscular dysplasia of both renal arteries
- Uncontrolled hypertension, DM, obesity
- Solitary kidney
- Warm ischemia time must be minimized — kidney packed in cold preservative solution immediately
- Cold ischemia time for transplant ideally <24 hours
🗃️ MASTER COMPARISON TABLE
| Feature | Radical | Simple | Partial | Donor |
|---|
| What's removed | Kidney + Gerota's fascia + adrenal + LN | Kidney only | Tumor + margin only | Healthy kidney |
| Main Indication | RCC (malignant) | Benign non-functioning kidney | Small RCC / nephron-sparing | Living kidney transplant |
| Gerota's fascia | Removed (en bloc) | May be left | Preserved | Preserved |
| Adrenal gland | Usually removed | Not removed | Not removed | Not removed |
| Lymph nodes | Removed (staging) | Not removed | Not removed | Not removed |
| Contralateral function needed? | Yes (must be adequate) | Yes | Yes | Must have 2 healthy kidneys |
| Oncologic margin | Wide (en bloc) | Not required | Narrow margin (1–2 mm) | N/A |
| Warm ischemia | Not an issue | Not an issue | <25 minutes critical | Minimize; cold perfusion used |
| Most common approach | Laparoscopic | Laparoscopic | Robotic-assisted | Laparoscopic (HALDN) |
| Key complication | IVC injury, tumor spillage | Subcapsular adhesion injury | Urine leak, hemorrhage | Ureteral injury, donor morbidity |
| Special scoring/staging | IVC thrombus level (Neves) | None | RENAL score | — |
| Key contraindication | Bilateral tumors → prefer partial | Normal kidney → don't remove | Unresectable large tumor | Single kidney, bilateral renal disease |
🔑 SURGICAL APPROACHES — ALL NEPHRECTOMIES
| Approach | Description | Used In |
|---|
| Flank | Through 11th/12th rib space; retroperitoneal | Simple, radical, donor |
| Transperitoneal | Through abdominal cavity; better exposure | Radical (large tumors, IVC) |
| Thoracoabdominal | Opens chest + abdomen; best for upper pole | Radical T3b/T4 |
| Laparoscopic (transperitoneal) | Port-based, pneumoperitoneum | All types |
| Retroperitoneoscopic | Retroperitoneal laparoscopic | Simple, partial, donor |
| Robotic-assisted | Robot-controlled instruments | Partial (most common), radical |
| Hand-assisted laparoscopic | Hand-port + laparoscope | Donor (preferred), radical |
⚡ HIGH-YIELD CLINICAL PEARLS (Exam Favorites)
| Fact | Detail |
|---|
| Gerota's fascia breached = tumor spillage | Stage changes to T3 if breached |
| Adrenal spared in radical if... | Imaging normal + tumor not in upper pole |
| Artery ligated before vein in radical | Prevents renal venous engorgement |
| Warm ischemia limit in partial | <25 minutes (some say <20 min) |
| Left kidney for donor | Longer left renal vein → easier venous anastomosis |
| Hem-o-lok clips banned | For renal artery in donor nephrectomy only |
| Nephron-sparing absolute indication | Solitary kidney or bilateral RCC |
| RENAL score >10 | High complexity → open preferred |
| Subcapsular nephrectomy for... | Dense perirenal adhesions (xanthogranulomatous PN, TB) |
| IVC level IV thrombus needs... | Cardiopulmonary bypass (CPB) |
| Most common complication partial | Urine leak → drain amylase/creatinine to diagnose |
| Trifecta of partial nephrectomy | Negative margins + no complications + preserved function |
🧠 MEMORY AIDS
Radical = "R-A-D-I-C-A-L"
- Remove everything en bloc
- Adrenal included (usually)
- Diagnosis = RCC
- IVC thrombus managed by levels
- Cancer indication
- Artery first, then vein
- Lymph nodes for staging
Partial = "SPARE"
- Solitary kidney = absolute indication
- Preserve >25% function
- Arteries mapped pre-op (CT angiography)
- RENAL score guides approach
- Exposed warm ischemia <25 min
Donor = "LEFT GIFT"
- Left kidney preferred
- Experience required for 3+ arteries
- Forbid Hem-o-lok clips on artery
- Transfixing suture for renal artery
This covers all four nephrectomy types with their subtypes, indications, surgical approaches, key clinical pearls, and the full master comparison table. Each type is clearly differentiated by what is removed, why, and the critical intraoperative considerations.