Tumors of Salivary GLAND. MS ENT university Exam format for 20 marks. with relevant diagrams as per standard textbooks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive content from the textbooks. Let me compile the full MS ENT exam answer:
TUMORS OF SALIVARY GLAND
MS ENT University Examination Answer - 20 Marks
INTRODUCTION
Salivary gland neoplasms are uncommon, representing less than 4% of all head and neck neoplasms. The WHO 4th edition (2017) classification recognizes 18 benign and multiple malignant subtypes. Understanding the distribution principle is foundational:
"The smaller the gland, the higher the probability of malignancy."
| Gland | % Tumors Arising Here | % Malignant |
|---|---|---|
| Parotid | 80% | 20% |
| Submandibular | 10-15% | 50% |
| Sublingual | Rare | 80% |
| Minor salivary glands | 5-10% | 80% |
(Cummings Otolaryngology, Schwartz's Surgery)
CLASSIFICATION (WHO 2017)
A. Benign Tumors
- Pleomorphic adenoma (Benign Mixed Tumor) - most common
- Warthin's tumor (Papillary cystadenoma lymphomatosum/Adenolymphoma)
- Oncocytoma
- Basal cell adenoma
- Canalicular adenoma
- Myoepithelioma
- Cystadenoma
- Ductal papillomas
- Sebaceous adenoma / sebaceous lymphadenoma
- Lymphadenoma
B. Malignant Tumors
- Mucoepidermoid carcinoma - most common malignant
- Adenoid cystic carcinoma
- Acinic cell carcinoma
- Carcinoma ex pleomorphic adenoma
- Adenocarcinoma NOS
- Polymorphous low-grade adenocarcinoma (PLGA)
- Squamous cell carcinoma (primary)
- Salivary duct carcinoma
- Myoepithelial carcinoma
- Small cell carcinoma
HISTOGENESIS
Two main theories:
- Bicellular stem cell (Reserve cell) theory - currently favored. Tumors arise from two undifferentiated stem cell populations: the excretory duct reserve cell (gives rise to squamous and mucoepidermoid carcinoma) and the intercalated duct reserve cell (gives rise to pleomorphic adenoma, Warthin's, acinic cell carcinoma, adenoid cystic carcinoma).
- Multicellular theory - different tumor types arise from different mature cell types already present in the gland.
BENIGN TUMORS
1. PLEOMORPHIC ADENOMA (Benign Mixed Tumor)
Most common salivary gland neoplasm overall.
Epidemiology:
- 60-70% of all parotid tumors
- Peak incidence: 4th-6th decade; slight female preponderance
- Can arise in any salivary gland; 80% occur in parotid (superficial lobe)
Clinical Features:
- Slowly growing, painless, firm swelling in the parotid region
- Mobile, non-tender, lobulated surface
- NO facial nerve palsy (absence of palsy does NOT exclude malignancy)
- Long history (years to decades)
Imaging:
The classic "dumbbell" configuration occurs when the tumor extends from the superficial to the deep lobe of the parotid through the stylomandibular tunnel, giving a narrow isthmus on imaging.
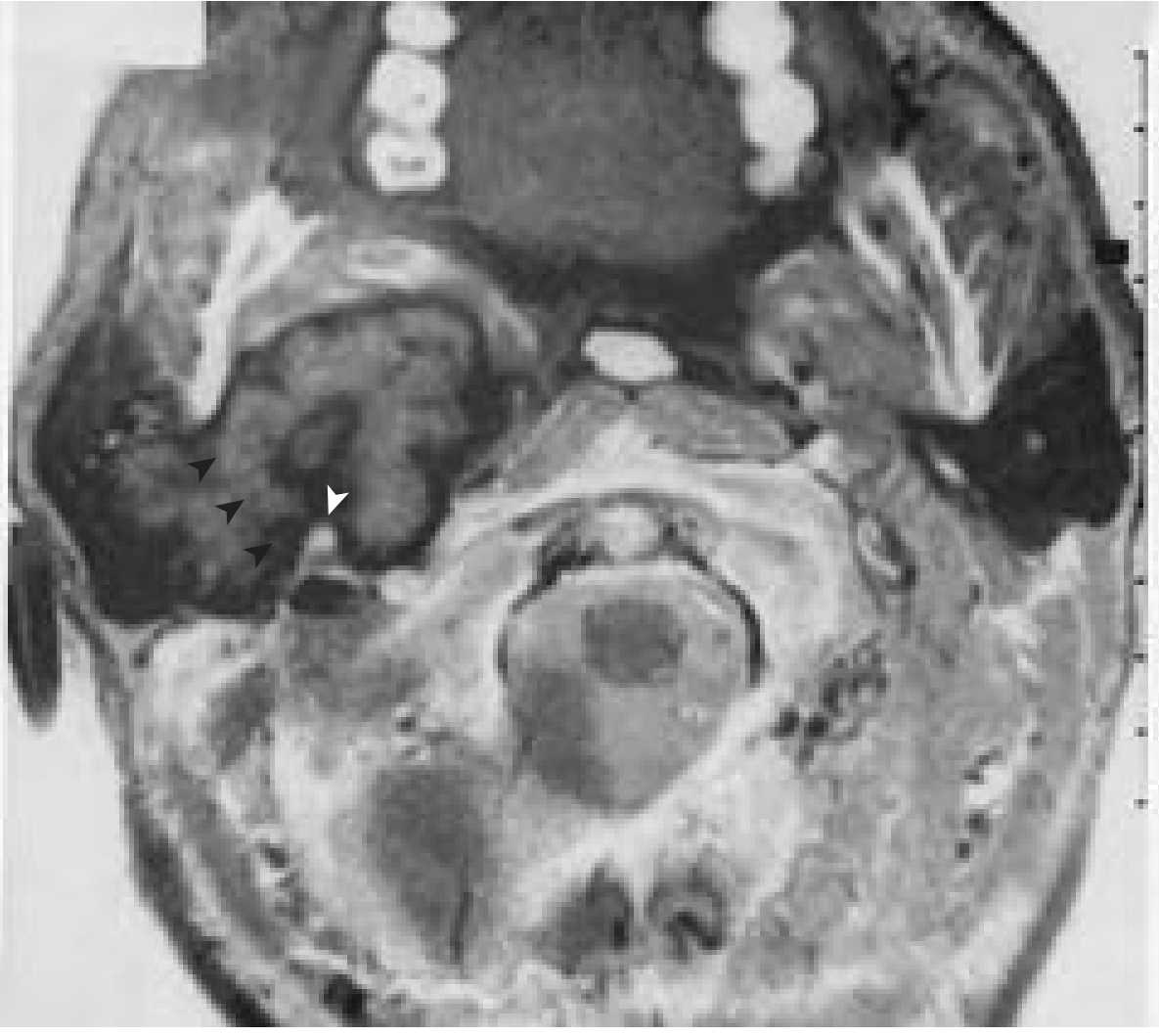
Fig. 84.10 (Cummings Otolaryngology) - Axial CT gadolinium: Large pleomorphic adenoma. The narrow isthmus through the stylomandibular space creates the classic "dumbbell" appearance.
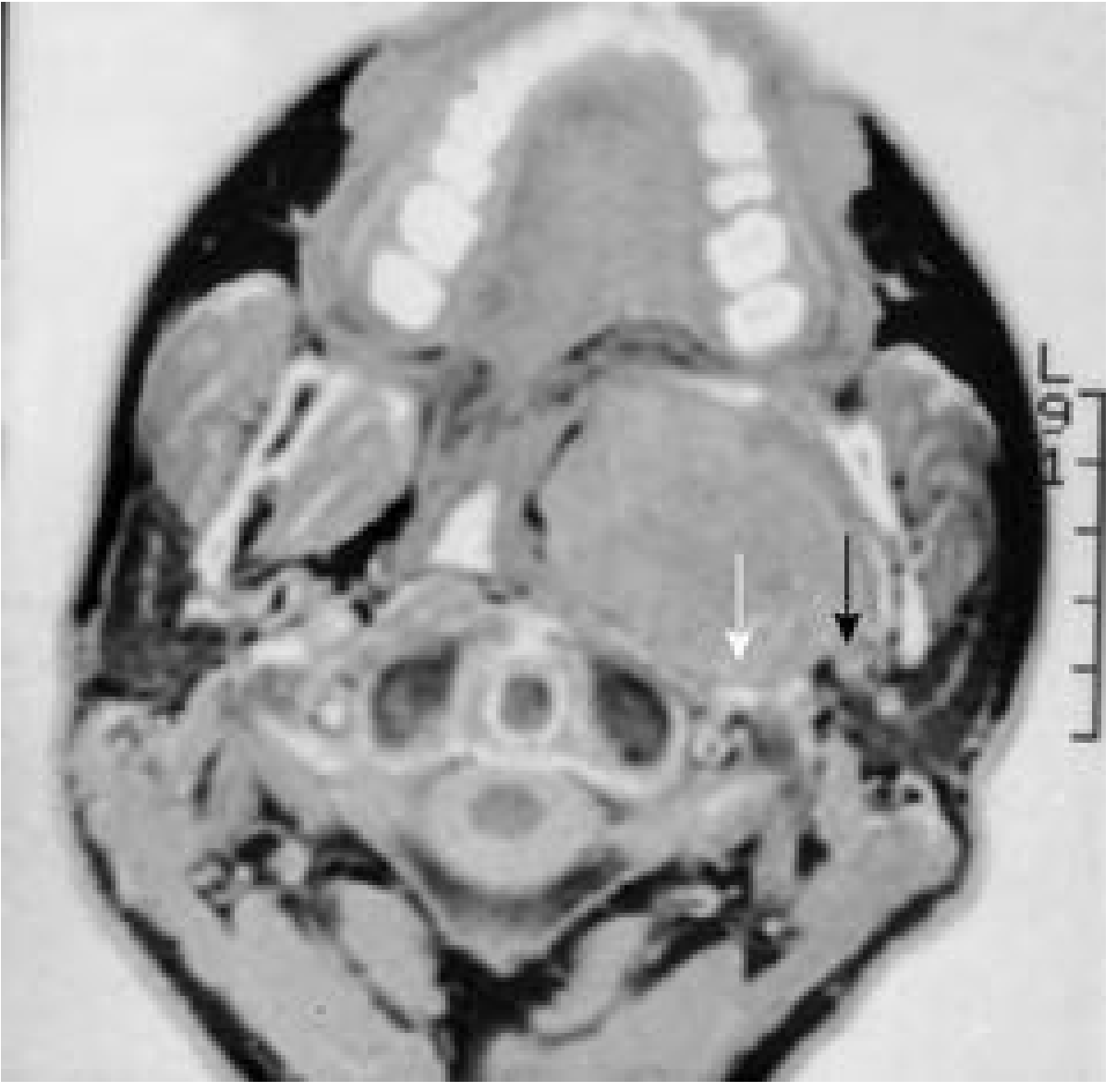
Fig. 84.11 (Cummings Otolaryngology) - Pleomorphic adenoma originating entirely from the deep lobe, displacing the carotid posteriorly.
Pathology:
- Gross: Well-encapsulated, bosselated/lobulated mass. Cut section shows firm gray-white tissue, with chondromyxoid areas and occasional cysts.
- Micro: Mixture of epithelial cells (forming ducts, nests) + myoepithelial cells in a chondromyxoid stroma - the hallmark. Capsule may be incomplete (pseudocapsule) - basis for recurrence.
Key Points:
- Recurrence rate: 2-5% (simple enucleation gives ~20-45% recurrence)
- Malignant transformation (carcinoma ex pleomorphic adenoma): 5-10% if untreated long-term; risk increases after 15 years
- LIPO (Lateral Isolated Parotidectomy Obstruction) rule: never enucleate
Treatment:
- Superficial parotidectomy with facial nerve identification and preservation
- Deep lobe tumors: Total parotidectomy with facial nerve preservation
- Minor salivary gland: Wide local excision with cuff of normal tissue
- Simple enucleation is contraindicated - high recurrence rate
2. WARTHIN'S TUMOR (Papillary Cystadenoma Lymphomatosum / Adenolymphoma)
Second most common benign salivary gland tumor.
Epidemiology:
- ~10% of all parotid tumors
- Male preponderance; Caucasians > other racial groups
- Age: >40 years; strongly associated with cigarette smoking
- 5-12% are bilateral; multifocality in up to 20% - unique among salivary tumors
- Occurs almost exclusively in the parotid gland (lower pole/tail)
Clinical Features:
- Soft, fluctuant, slowly growing mass at the angle of jaw/lower parotid
- Usually asymptomatic; occasional pain and swelling from inflammatory episodes
- "Hot" on Tc-99m pertechnetate scan (characteristic - due to oncocytic cells)
Pathology:
- Gross: Ovoid, encapsulated, cystic; cut section shows papillary cysts with brown mucoid fluid + gray lymphoid tissue
- Micro (PATHOGNOMONIC): Papillary projections of bilayered eosinophilic epithelium (oncocytes - large columnar with abundant mitochondria-rich granular cytoplasm) projecting into cystic spaces, surrounded by lymphoid stroma with germinal centers
Diagram - Warthin's Tumor Histology:
┌─────────────────────────────────┐
│ CYSTIC LUMEN (mucoid fluid) │
│ │
│ ████ Papillary projections │
│ ████ Bilayered oncocytic │
│ ████ epithelium (2 rows): │
│ - Tall columnar (luminal) │
│ - Cuboidal (basal) │
│ │
│ [Lymphoid stroma with │
│ germinal centers around] │
└─────────────────────────────────┘
Treatment: Surgical excision (superficial parotidectomy); enucleation acceptable in elderly given benign nature
MALIGNANT TUMORS
3. MUCOEPIDERMOID CARCINOMA (MEC)
Most common malignant salivary gland tumor (35-40% of all malignant salivary tumors).
Epidemiology:
- Most common in parotid gland; also most common malignant minor salivary gland tumor
- Wide age range; most common salivary malignancy in children
- Associated with radiation exposure (post-radiation)
Clinical Features:
- Low-grade: Slow-growing, painless mass; often indistinguishable from benign
- High-grade: Rapid growth, pain, skin fixation, facial nerve involvement, cervical lymphadenopathy
Grading (AFIP criteria):
| Grade | Behavior | % Cystic | Key Features |
|---|---|---|---|
| Low | Indolent | >90% | Predominantly mucous cells |
| Intermediate | Moderate | 50% | Mix |
| High | Aggressive | <10% | Predominantly epidermoid cells, necrosis, mitoses |
Pathology - Three Cell Types:
- Mucous cells - goblet-type, mucin-secreting (PAS positive)
- Epidermoid cells - squamoid, forming sheets
- Intermediate cells - small basaloid; can differentiate into either
HISTOLOGY - MUCOEPIDERMOID CARCINOMA:
┌──────────────────────────────────────┐
│ CYSTIC SPACES (mucus-filled) │
│ │
│ [Mucous cells lining cysts] │
│ [Epidermoid cells in solid sheets] │
│ [Intermediate cells - basaloid] │
│ │
│ Low grade: Large cysts >> solid │
│ High grade: Solid >> cysts, + │
│ necrosis, mitoses │
└──────────────────────────────────────┘
Treatment:
- Low/Intermediate grade: Wide local excision with adequate margins
- High grade: Wide excision + neck dissection + post-op radiotherapy
- 5-year survival: Low-grade ~90-95%; High-grade ~25-50%
4. ADENOID CYSTIC CARCINOMA (AdCC)
Most common malignant tumor of the submandibular gland and minor salivary glands (palate most common minor SG site).
Characteristics:
- Slow but relentlessly progressive course
- Notorious for perineural invasion (pathognomonic feature)
- Tendency for skip lesions along nerves
- Late distant metastasis (lung most common); survival curves do not plateau until >10 years
- 5-year survival ~70-80%; 10-year survival drops significantly
Three Histological Patterns (prognostically important):
- Cribriform (Swiss-cheese) - most common; best prognosis; "cylindromatous" pattern - pseudocysts filled with mucoid material
- Tubular - best prognosis
- Solid - worst prognosis; high-grade transformation
ADENOID CYSTIC CARCINOMA - CRIBRIFORM PATTERN:
┌────────────────────────────────────────┐
│ │
│ ○○○ ○○○ ○○○ ← Pseudocysts │
│ ●●●●●●●●●●●●●● ← Basaloid cells │
│ ○○○ ○○○ ○○○ (epithelial + │
│ ●●●●●●●●●●●●●● myoepithelial) │
│ │
│ "SWISS-CHEESE" appearance │
│ Perineural invasion: ═══◄(nerve) │
└────────────────────────────────────────┘
Treatment:
- Wide surgical excision with clear margins (often requires sacrifice of affected nerves)
- Adjuvant radiation therapy (neutron beam if available)
- Neck dissection for clinically positive nodes
- Poor response to chemotherapy
5. ACINIC CELL CARCINOMA (ACC)
- Second/third most common malignant parotid tumor
- Predominantly in parotid (90%)
- Bimodal age distribution; slight female preponderance
- Low-grade malignancy; 10-15% metastasize
- Histology: Large cells with abundant blue cytoplasmic granules (serous-type; PAS+ diastase resistant); dense lymphoid infiltrate
- Hallmark: DOG1 positive on IHC (membrane pattern)
- Survival: ~80% at 5 years, 70% at 10 years
- High-grade transformation seen in 10-20%
6. CARCINOMA EX PLEOMORPHIC ADENOMA
- Malignant transformation of a pre-existing pleomorphic adenoma
- Risk increases with duration: ~1% at 5 years, rising to 10% after 15 years
- Clinical clue: Sudden rapid growth of a previously slow-growing mass + pain + nerve involvement
- Prognosis depends on: type of carcinoma arising, grade, and extent of invasion
- Intracapsular (non-invasive): good prognosis
- Minimally invasive (<6 mm beyond capsule): intermediate
- Frankly invasive: poor prognosis
CLINICAL FEATURES SUGGESTING MALIGNANCY
| Feature | Significance |
|---|---|
| Rapid growth | High-grade malignancy |
| Pain | Perineural invasion / nerve involvement |
| Facial nerve palsy | Malignant infiltration (10-15% of parotid malignancies) |
| Skin fixation/ulceration | T4 disease |
| Hard, fixed mass | Malignant infiltration |
| Cervical lymphadenopathy | Regional metastasis |
| Paresthesia/numbness | Perineural spread |
| Trismus | Pterygoid/masticator space invasion |
INVESTIGATIONS
Fine Needle Aspiration Biopsy (FNAB/FNA)
- Investigation of choice for preoperative diagnosis
- Accuracy: 70-80% when reviewed by experienced cytopathologist
- Sensitivity for malignancy lower than specificity (i.e., more common to miss malignancy than to over-call it)
- New classification: Milan System for Reporting Salivary Gland Cytopathology (analogous to Bethesda for thyroid)
- Open biopsy is CONTRAINDICATED - risk of tumor spillage, fistula, skin implantation, and injury to facial nerve
Imaging
- MRI (preferred): Superior soft tissue delineation, extent of tumor, parapharyngeal space, perineural invasion
- CT: Useful for bone erosion, salivary duct calculi; high fat content of normal parotid makes masses stand out
- Ultrasound: First-line for superficial lesions; guides FNA
- Tc-99m pertechnetate scintigraphy: Warthin's tumor is "hot" (accumulates tracer); most other tumors are "cold"
- PET-CT: Limited role for primary; useful for distant metastases in confirmed high-grade malignancies
TNM STAGING (AJCC 8th Edition - Major Salivary Glands)
| Stage | T | N | M |
|---|---|---|---|
| I | T1 (≤2 cm, no extraparenchymal) | N0 | M0 |
| II | T2 (2-4 cm, no extraparenchymal) | N0 | M0 |
| III | T3 (>4 cm or extraparenchymal extension) | N0/N1 | M0 |
| IVA | T1-3N1, T4a any N | N1 | M0 |
| IVB | Any T N2-3, T4b any N | N2-3 | M0 |
| IVC | Any T, Any N | Any N | M1 |
T-staging:
- T1: ≤2 cm, no extraparenchymal extension
- T2: 2-4 cm, no extraparenchymal extension
- T3: >4 cm OR extraparenchymal extension
- T4a: Invades skin, mandible, ear canal, or facial nerve
- T4b: Invades skull base, pterygoid plates, or encases carotid artery
(ENE - Extranodal Extension - incorporated in N-staging in AJCC 8th Edition: any ENE(+) upstages nodal category)
SURGICAL MANAGEMENT
Parotid Surgery
Facial nerve identification - Landmarks:
- Tragal pointer - facial nerve lies 1 cm deep and inferiomedial to tragal cartilage tip (most reliable)
- Tympanomastoid suture - nerve emerges 6-8 mm deep to inferior end of suture
- Posterior belly of digastric - nerve lies just superior and lateral to posterior belly at its insertion
- Retrograde dissection - from distal branches backward (used when trunk not found)
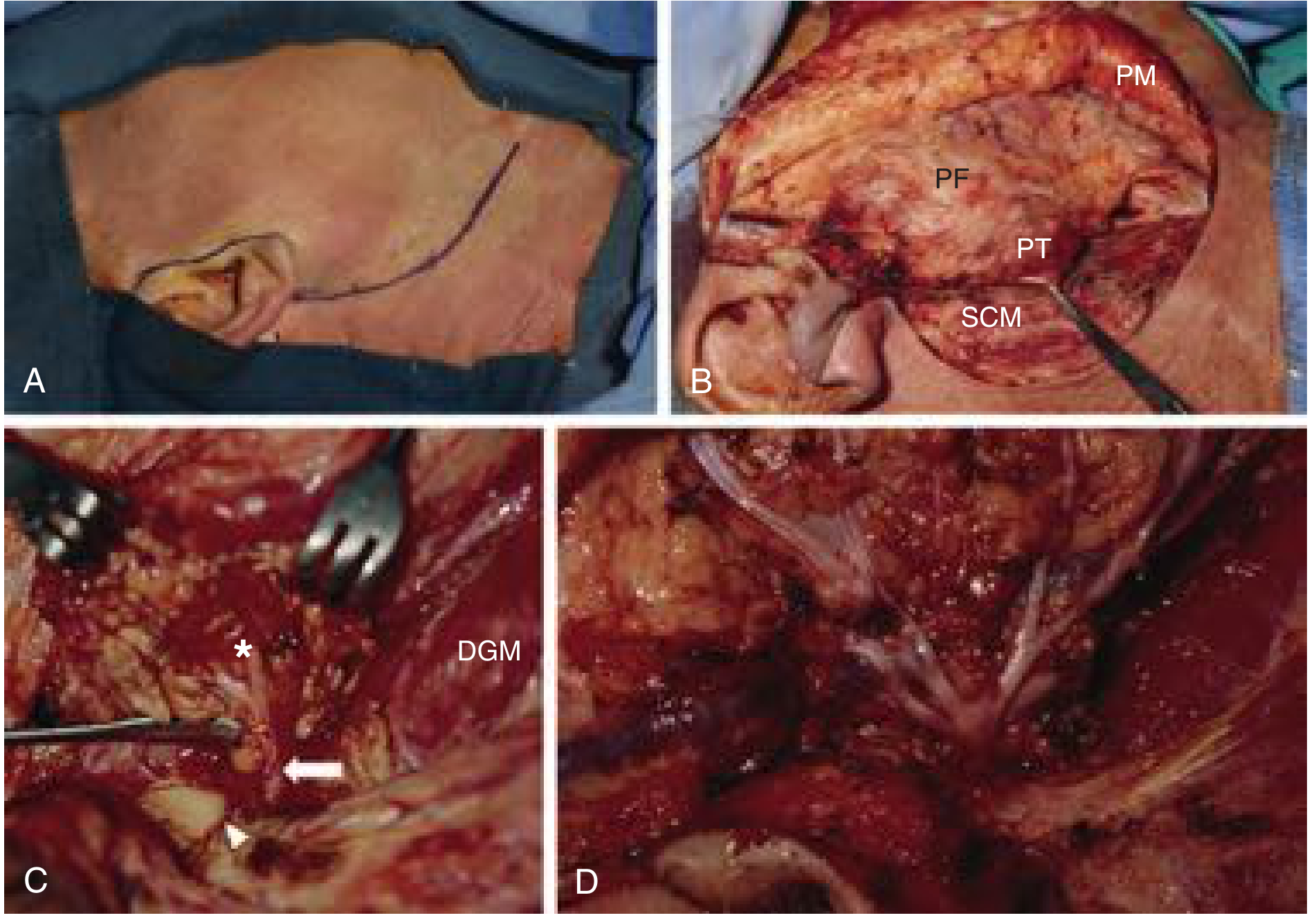
Fig. 84.25 (Cummings Otolaryngology) - Right superficial parotidectomy: (A) Modified Blair incision, (B) Exposure of parotid and SCM, (C) Facial nerve identification, (D) Fanned-out facial nerve branches dissected.
Types of Parotidectomy:
- Superficial parotidectomy: For benign superficial lobe tumors (preserves facial nerve, removes superficial lobe)
- Total parotidectomy with FN preservation: For deep lobe tumors, large tumors, malignancy without nerve involvement
- Radical parotidectomy: Sacrificing facial nerve when invaded by tumor; reconstruct with nerve graft (greater auricular / sural nerve)
Neck Dissection Indications in Parotid Malignancy:
- T3/T4 tumors
- High-grade histology
- Extraparotid extension
- Perineural invasion
- Clinically positive nodes (cN+)
- Occult nodal metastases present in ~30% of parotid malignancies
COMPLICATIONS OF PAROTIDECTOMY
| Complication | Mechanism | Notes |
|---|---|---|
| Frey's syndrome (Auriculotemporal syndrome) | Aberrant reinnervation of sweat glands by parasympathetic fibers | Gustatory sweating/flushing over cheek; treated with Botox or tympanic neurectomy |
| Facial nerve palsy | Traction/transection | Temporary palsy up to 30-40%; permanent <1% in expert hands |
| Salivary fistula / Sialocele | Parotid remnant secretion | Usually resolves with pressure dressings |
| Great auricular nerve numbness | Divided during flap elevation | Earlobe numbness |
| Hematoma | - | Early complication |
| Infection | - | Rare |
ADJUVANT RADIOTHERAPY - INDICATIONS
- High-grade malignancies
- Positive or close surgical margins
- Perineural invasion
- Lymph node metastasis with ENE
- T3/T4 disease
- Recurrent disease
PROGNOSIS SUMMARY
| Tumor | 5-Year Survival | Key Prognostic Factor |
|---|---|---|
| Pleomorphic adenoma | >95% (benign) | Recurrence if enucleated |
| Warthin's tumor | Essentially 100% | Bilaterality |
| Low-grade MEC | 90-95% | Grade |
| High-grade MEC | 25-50% | Grade + nodal status |
| Adenoid cystic CA | 70-80% (5yr), worse at 10yr | Late recurrences; perineural invasion |
| Acinic cell CA | 80% (5yr), 70% (10yr) | High-grade transformation |
| Carcinoma ex PA | Variable (15-40%) | Extent of invasion |
EXAM DIAGRAMS
Diagram 1 - "Rule of 80s" in Salivary Tumors
PAROTID SUBMANDIBULAR SUBLINGUAL/MINOR
┌──────┐ ┌──────┐ ┌──────┐
│ │ │ │ │ │
│ 80% │ │ 50% │ │ 80% │
│BENIGN│ │MALIG │ │MALIG │
│ │ │ │ │ │
└──────┘ └──────┘ └──────┘
80% of all tumors
start here
Diagram 2 - Facial Nerve Trunk Identification (Tragal Pointer)
Ear
│
Tragus ●───── Tragal pointer
│ ↓
│ 1 cm deep & inferior
│ ↓
│ ═══ FACIAL NERVE TRUNK
│ / \
Temporal Zygomatic Buccal Marginal Cervical
branch branch branch mandibular branch
Diagram 3 - Modified Blair Incision
┌─── Preauricular crease
│
│ extends to root of helix (superior)
│
[EAR]
│
└── around lobule → mastoid tip
│
└── down SCM (posterior border)
Diagram 4 - WHO 2017 Classification Summary
SALIVARY GLAND TUMORS
│
├── BENIGN (most common → most rare)
│ ├── Pleomorphic adenoma (most common overall)
│ ├── Warthin's tumor (bilateral, "hot" on scan)
│ ├── Oncocytoma
│ └── Others (basal cell adenoma, myoepithelioma...)
│
└── MALIGNANT
├── Mucoepidermoid Ca (most common malignant)
│ └── [Low / Intermediate / High grade]
├── Adenoid cystic Ca (perineural invasion, late mets)
│ └── [Cribriform > Tubular > Solid]
├── Acinic cell Ca (low-grade, 90% parotid)
├── Carcinoma ex PA (transform of PA)
└── Adenocarcinoma NOS / PLGA / others
QUICK REVISION TABLE
| Feature | Pleomorphic adenoma | Warthin's | MEC | AdCC |
|---|---|---|---|---|
| Most common in | Parotid | Parotid (tail) | Parotid | Submandibular/minor |
| Bilateral | No | 5-12% | No | No |
| Smoking link | No | Yes | No | No |
| Scan | Cold | HOT (Tc-99m) | Cold | Cold |
| Histology hallmark | Epi + myoepi + chondromyxoid stroma | Bilayer oncocytes + lymphoid stroma | 3 cell types (mucous, epidermoid, intermediate) | Swiss cheese (cribriform) |
| Perineural invasion | No | No | High-grade | YES (hallmark) |
| Distant mets | No | No | High-grade | Lung (late) |
| Treatment | Superficial parotidectomy | Superficial parotidectomy | Surgery ± RT ± ND | Surgery + RT |
Sources: Cummings Otolaryngology Head and Neck Surgery, 7th Ed. (Chs. 84-85); Schwartz's Principles of Surgery, 11th Ed.; Scott-Brown's Otorhinolaryngology, 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.