Red and white lesions of oral cavity in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"oral leukoplakia" OR "oral erythroplakia" malignant transformation
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
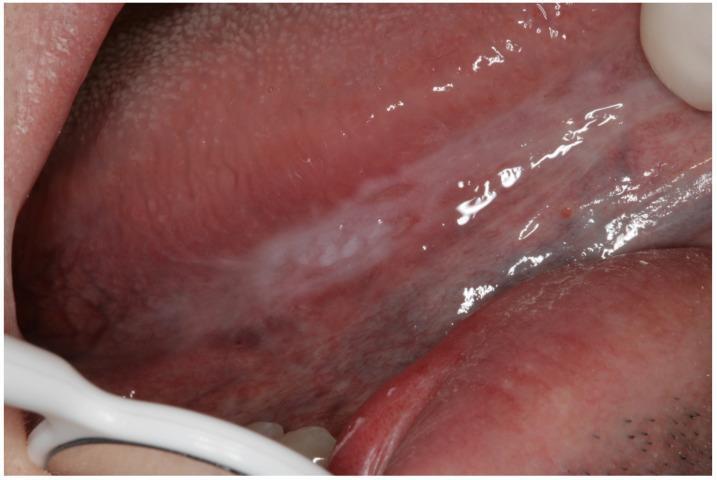
oral leukoplakia white lesion tongue
Reading File
Searching Images
oral erythroplakia red lesion floor mouth
Finding Sources
Reading File
Reading File
Reading File
Searching Images
oral lichen planus Wickham striae reticular erosive
I now have comprehensive content from multiple authoritative textbooks. Let me compile the detailed answer:
Red and White Lesions of the Oral Cavity
Overview
Oral mucosal lesions can be broadly divided into white lesions, red lesions, and mixed (erythroleukoplakic) lesions. Many are benign reactive conditions; others are potentially malignant disorders (OPMDs) requiring vigilance and biopsy. The most clinically significant white lesion is leukoplakia and the most dangerous red lesion is erythroplakia.
WHITE LESIONS
1. Leukoplakia
Definition: Leukoplakia is defined by the WHO as "a white patch or plaque that cannot be scraped off and cannot be characterized clinically or pathologically as any other disease." It is a clinical diagnosis of exclusion — white patches caused by obvious irritation, candidiasis, or lichen planus are not considered leukoplakia.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 684
- Fitzpatrick's Dermatology, p. 1906
Epidemiology:
- Most common potentially malignant oral lesion; global prevalence 0.5–3.4%
- Peak incidence age >40 years; male:female = 2:1
- 6× more common in smokers vs. non-smokers
Sites: Buccal mucosa (most common), floor of mouth, ventral tongue, palate, gingiva
Clinical Types:
| Type | Description | Malignant Risk |
|---|---|---|
| Homogeneous | Flat, uniform white plaque; smooth, wrinkled, or corrugated surface | Lower |
| Non-homogeneous (Erythroleukoplakia) | White + red areas; irregular, flat, nodular, ulcerative, or verrucous | Significantly higher |
| Proliferative Verrucous (PVL) | Rare; multifocal, verrucous; often in non-tobacco users | Highest — high transformation + recurrence |

Etiology/Pathogenesis:
- Tobacco — strongest risk factor (smoked and smokeless forms); areca/betel nut
- Alcohol — synergistic with tobacco
- HPV — detected in up to 22% of lesions; high-risk subtypes (HPV 16, 18) implicated as independent risk factors
- Chronic mechanical trauma (linea alba, morsicatio) → frictional keratosis — NOTE: these resolve when the irritant is removed and are NOT true leukoplakia
- Fitzpatrick's Dermatology, p. 1907
Histopathology:
Spectrum from:
- Simple hyperkeratosis + acanthosis (no dysplasia) → lowest risk
- Mild/moderate dysplasia → atypical mitoses, nuclear pleomorphism
- Severe dysplasia / carcinoma in situ → highest risk
- Transformation into invasive SCC occurs when dysplastic cells breach the basement membrane
- Fitzpatrick's Dermatology, p. 1907
Diagnosis:
- Clinical diagnosis of exclusion
- Eliminate causative factors (tobacco, trauma) for 2–6 weeks; if no resolution → mandatory biopsy
- Biopsy directly if no causative factor identified, or if symptomatic
Differential diagnosis (Table 110-8, Fitzpatrick's):
- Tobacco/frictional keratosis, candidiasis (pseudomembranous — can be scraped off), lichen planus, linea alba, leukoedema, white sponge nevus, hairy leukoplakia, lupus erythematosus, verrucous/squamous cell carcinoma
Malignant transformation:
- Overall rate ~2–3% per year across all subtypes
- 5–25% of leukoplakias are premalignant
- High-risk features: epithelial dysplasia, non-homogeneous clinical subtype, floor of mouth/ventral tongue location, female sex, long duration, large lesion size
- Cummings Otolaryngology, p. 1582; Robbins & Kumar, p. 684
Treatment:
- Eliminate risk factors (tobacco cessation, alcohol reduction)
- Surgical excision or CO₂ laser ablation (treatment of choice)
- Regular surveillance with biopsy of suspicious areas
- No consensus on medical therapy; topical retinoids have been used with limited evidence
2. Hairy Leukoplakia
Definition: A distinctive white oral lesion on the lateral tongue caused by Epstein-Barr virus (EBV) in immunocompromised patients. It is not premalignant but is a marker of immunosuppression.
Clinical features:
- White, confluent patches with fluffy ("hairy") corrugated/shaggy surface
- Almost always bilateral lateral borders of tongue
- Cannot be scraped off (unlike candida)
- Robbins, Cotran & Kumar, p. 683

Histology: Hyperparakeratosis, acanthosis, "balloon cells" in upper spinous layer, EBV RNA/proteins detectable; superimposed candidal infection is common.
Clinical context:
- HIV/AIDS (may portend AIDS development)
- Post-transplant immunosuppression
- Hematologic malignancies, cancer chemotherapy
Management: No specific treatment needed in most cases. In HIV+ patients, lesions resolve with effective antiretroviral therapy.
3. Oral Lichen Planus (OLP)
Definition: A chronic mucocutaneous immunologic disease mediated by T-cell lymphocytic reaction against epithelial antigens. Prevalence: 0.2–3% of the population; predominantly middle-aged women.
Clinical types:
| Variant | Description | Symptoms |
|---|---|---|
| Reticular | Classic bilateral Wickham striae — white lacy/net-like lines over buccal mucosa | Usually asymptomatic |
| Papular | White papules coalescing into striae | Minimal |
| Plaque-like | Homogeneous white plaque resembling leukoplakia | Variable |
| Atrophic/Erythematous | Thinned, reddened mucosa; faint striae; often with other forms | Mild burning |
| Erosive/Ulcerative | Irregularly marginated, intense erythema with superficial erosions; most painful form | Painful |
| Bullous | Rare; fluid-filled bullae rupturing into erosions | Painful |


Histology: Interface mucositis — band-like subepithelial lymphocytic infiltrate, basal cell liquefactive degeneration, saw-tooth rete ridges, Civatte (colloid) bodies.
Malignant potential: ~1% risk of transformation to oral SCC, particularly with erosive form. Considered an OPMD by WHO. Regular follow-up required.
Treatment: Topical corticosteroids (first line for symptomatic cases); topical calcineurin inhibitors (tacrolimus, cyclosporine); systemic steroids for severe/widespread disease.
4. Other White Lesions
| Lesion | Key Features |
|---|---|
| Leukoedema | Diffuse, grayish-white opalescence of buccal mucosa; disappears on stretching; variant of normal |
| Linea alba | Horizontal white line on buccal mucosa at occlusal plane; benign frictional lesion |
| Morsicatio (cheek/lip biting) | Ragged, shredded white patches; bilateral; resolves if habit stops |
| White sponge nevus | Autosomal dominant; diffuse, thick, folded white mucosa from childhood |
| Candidiasis (pseudomembranous) | White curd-like plaques that CAN be wiped off, leaving red/bleeding base; Candida albicans |
| Chemical burn (aspirin, etc.) | White necrotic plaque at site of local application; history is key |
| Verrucous carcinoma | White, warty, exophytic; low-grade SCC variant; strongly tobacco-associated |
RED LESIONS
1. Erythroplakia
Definition: A clinical diagnosis of exclusion for a persistent fixed red patch in the oral cavity that cannot be attributed to any other identifiable cause.
- Fitzpatrick's Dermatology, p. 1908
- Robbins, Cotran & Kumar, p. 684
Epidemiology:
- Rarest oral OPMD; prevalence 0.02–0.83%
- Middle-aged adults; male predominance
- Associated with reverse cigar smoking (chutta smokers of India)
Clinical features:
- Asymptomatic, solitary, sharply demarcated erythematous macule or patch
- Surface smooth, soft, velvety (occasionally pebbled)
- Most common sites: soft palate, floor of mouth, buccal mucosa
- Usually <1.5 cm; up to 4 cm described
- Induration = highly suspicious for invasive SCC

Etiology/Pathogenesis:
- Tobacco, alcohol, areca nut (same risk factors as leukoplakia)
- High p53 tumor suppressor gene mutation rate — explains high malignant potential
- The red color results from epithelial atrophy (thin epithelium makes underlying vasculature visible) + subepithelial vascular dilatation + inflammatory reaction
Histopathology:
- ~90% show severe dysplasia, carcinoma in situ, or minimally invasive carcinoma — the most ominous histology of any OPMD
- Rarely demonstrates orderly epithelial maturation
- Robbins, Cotran & Kumar, p. 684
Mixed lesion: When white and red components coexist: speckled erythroplakia (erythroleukoplakia) — red patches within this mixed lesion carry the highest malignant risk component.
Treatment:
- Biopsy mandatory to rule out invasive carcinoma
- Surgical excision or CO₂ laser
- Lesions >80 mm² carry significantly higher risk of recurrence post-excision
Differential diagnosis (Table 110-10, Fitzpatrick's):
Erythematous candidiasis, atrophic lichen planus, lupus erythematosus, pemphigus, cicatricial pemphigoid, Kaposi sarcoma, contact/allergic stomatitis, thermal/mechanical injury, SCC, amelanotic melanoma.
2. Erythematous Candidiasis
- Red, atrophic patches without the white pseudomembrane
- Common on hard/soft palate (denture stomatitis) and dorsal tongue (median rhomboid glossitis)
- Often asymptomatic or burning sensation
- Responds to antifungal therapy
3. Other Red Lesions
| Lesion | Features |
|---|---|
| Denture stomatitis | Diffuse erythema beneath denture base; Candida and trauma |
| Geographic tongue (benign migratory glossitis) | Smooth red patches with white borders on dorsal tongue; migrating pattern; benign |
| Median rhomboid glossitis | Smooth red rhomboid patch on midline dorsal tongue; candidal association |
| Atrophic glossitis | Smooth, bald, red tongue; B12, iron, folate deficiency; Plummer-Vinson syndrome |
| Plasma cell gingivitis | Diffuse bright red gingiva; allergic reaction (cinnamon, chewing gum allergens) |
| Kaposi sarcoma | Red-purple macular lesions, often palate; AIDS-defining; vascular neoplasm |
| Hemangioma/Vascular malformation | Red-blue lesion; blanches on pressure |
MIXED RED AND WHITE LESIONS
Speckled Erythroplakia (Erythroleukoplakia)
- Combined red and white areas; the red foci within a mixed lesion carry the highest risk of dysplasia/malignancy
- Often represents advanced disease requiring urgent biopsy
Erosive Lichen Planus
- White striae surrounding central erythematous/erosive zones
- Bilateral buccal distribution characteristic
Pemphigus/Pemphigoid
- Pemphigus vulgaris: vesicles/bullae rupturing → hyperemic erosions with exudate; positive Nikolsky sign; IgG anti-desmoglein antibodies
- Mucous membrane pemphigoid: subepidermal blistering; gingiva most commonly affected (desquamative gingivitis)
Comparative Risk of Malignant Transformation
| Lesion | Malignant Transformation Rate |
|---|---|
| Homogeneous leukoplakia | ~1–2% |
| Non-homogeneous leukoplakia | ~4–7% |
| Proliferative verrucous leukoplakia | Very high (>50%) |
| Oral lichen planus (erosive) | ~1% |
| Erythroplakia | ~50–90% |
| Speckled erythroplakia | ~28–50% |
Key Diagnostic Principles
- Cannot be scraped off → leukoplakia, hairy leukoplakia, lichen planus, white sponge nevus
- Can be scraped off → pseudomembranous candidiasis
- Bilateral, symmetric, lacy → oral lichen planus (reticular)
- Red, velvety, ≥80% dysplasia → erythroplakia (biopsy urgently)
- White + red mixed → speckled erythroplakia (highest-risk component = red areas)
- Lateral tongue, HIV/immunosuppressed, corrugated → hairy leukoplakia (EBV)
- Any white/red lesion persisting >2 weeks after removing irritant → BIOPSY
Recent Evidence
A 2025 meta-analysis (PMID: 39314164) in Oral Diseases confirmed the malignant transformation rate of oral leukoplakia using comprehensive meta-analysis. A 2024 systematic review (PMID: 39290142) in J Dent Res analyzed recurrence patterns in oral leukoplakia post-treatment, noting that non-homogeneous histology and floor-of-mouth location predict higher recurrence.
Sources: Fitzpatrick's Dermatology (9th ed.), pp. 1906–1909 | Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 683–684 | Cummings Otolaryngology Head and Neck Surgery (7th ed.) | Robbins & Kumar Basic Pathology
Explain this in a creative manner and also add oral submucous fibrosis in this
Finding Sources
Reading File
Reading File
Searching Images
oral submucous fibrosis betel nut fibrotic bands trismus
I have all the material needed. Here is the creative, comprehensive presentation:
🎭 The Oral Cavity's Silent Drama: A Story of White, Red & Fibrous Villains
Imagine the oral cavity as a stage. Most days, the pink, moist mucosa performs its routine — talking, tasting, chewing. But sometimes, uninvited characters walk on stage: white ghosts, red flames, and a slow-moving concrete wall. Each one tells a story. Learn to read their lines — because some of them are whispering about cancer.
ACT I: THE WHITE CHARACTERS 🤍
🎭 Character #1 — LEUKOPLAKIA: "The White Mask"
"I cannot be wiped away. I cannot be explained. I simply exist — white, fixed, and watching."
Leukoplakia is the most common villain of the oral OPMD (Oral Potentially Malignant Disorder) world. The word itself means nothing specific — it is literally a diagnosis of exclusion: a white patch that sticks around with no other explanation. You try to rub it off — it laughs. You look for candida — it's not that. You look for trauma — gone already.
Where does it lurk?
- Buccal mucosa (its favorite hiding spot)
- Floor of the mouth and ventral tongue (danger zones)
- Palate, gingiva
Its two personalities:
| The Calm Twin 😐 | The Dangerous Twin 😈 |
|---|---|
| Homogeneous — flat, uniform, smooth or corrugated white plaque | Non-homogeneous — white + red patches (erythroleukoplakia), verrucous, nodular, or ulcerated |
| Lower malignant risk | Significantly higher risk |
There is also a third, rarest personality — Proliferative Verrucous Leukoplakia (PVL) — the serial offender. Multifocal, aggressive, keeps coming back after treatment, and ironically appears even in people who never smoked.
What feeds it?
🚬 Tobacco — its primary fuel (6× more common in smokers)
🍺 Alcohol — pours more fire
🌿 Areca (betel) nut — especially in South/Southeast Asia
🦠 HPV 16 & 18 — a co-conspirator in up to 22% of cases
What it looks like under the microscope:
The spectrum runs from peaceful to threatening:
- Hyperkeratosis + acanthosis → just thickened, no real trouble
- Mild → moderate dysplasia → abnormal mitoses, nuclear pleomorphism begin
- Severe dysplasia → carcinoma in situ → basement membrane breach → invasive SCC
Transformation rate: ~2–3% per year. Risk is highest when: dysplasia is present, the lesion is non-homogeneous, located on the floor of mouth/ventral tongue, or in a woman.
The detective's approach:
- Remove the irritant (tobacco, sharp tooth) — wait 2–6 weeks
- Didn't resolve? → BIOPSY without further debate
- Symptomatic? → BIOPSY immediately
Treatment: Surgical excision or CO₂ laser. No magic pill exists. Recurrence is common — surveillance is lifelong.
🎭 Character #2 — HAIRY LEUKOPLAKIA: "The Shaggy Ghost"
"I haunt only the weak — those whose immune system has already surrendered."
Hairy leukoplakia is the oral calling card of immunosuppression. Its villain is Epstein-Barr virus (EBV), and it almost always appears in patients with HIV/AIDS, post-transplant immunosuppression, or hematologic malignancy.
Signature look:
- Bilateral lateral borders of the tongue — white, corrugated, shaggy/hairy ridges
- Cannot be scraped off (unlike thrush)
- Ranging from subtle white streaks to thick corrugated plaques
Microscopic signature: Hyperparakeratosis, acanthosis, "balloon cells" in the upper spinous layer (EBV replicating inside), chromatin beading along nuclear membrane. Sometimes candida crashes the party, adding to the hairiness.
The good news: It is NOT premalignant. Its clinical significance is purely as a flag for systemic immunosuppression. Once HIV is treated with antiretrovirals → lesion disappears.
🎭 Character #3 — ORAL LICHEN PLANUS: "The Lace Artist"
"I am autoimmune. My T-cells are confused, and they have turned your mucosa into a canvas of white lace — and sometimes, burning wounds."
OLP affects 0.2–3% of the population and loves middle-aged women. Its immune mechanism: T-lymphocytes attack basal epithelial cells, causing characteristic interface mucositis.
Six faces of OLP:
| Form | Visual | Symptom |
|---|---|---|
| Reticular ✨ | Classic Wickham striae — bilateral white lacy lines on buccal mucosa | Asymptomatic |
| Papular | Small white dots coalescing into striae | Minimal |
| Plaque-like | Homogeneous white patch mimicking leukoplakia | Variable |
| Atrophic/Erythematous 🔴 | Thin, red mucosa with faint striae | Burning sensation |
| Erosive/Ulcerative 🔥 | Raw, red erosions with peripheral striae; most severe | Painful |
| Bullous | Fluid-filled vesicles → rupture → erosion | Painful |
Microscopic signature: Dense band-like lymphocytic infiltrate at the epithelium-connective tissue interface, Civatte bodies (apoptotic keratinocytes), saw-tooth rete ridges. DIF: fibrinogen deposits at the basement membrane zone.
Transformation risk: 0–10%; highest in the erosive/atrophic form. OLP is an OPMD — regular monitoring mandatory.
Associated systemic conditions: Hepatitis C, primary biliary cirrhosis, Sjögren syndrome, lupus erythematosus, primary sclerosing cholangitis.
Treatment: Topical corticosteroids (first line), topical tacrolimus or cyclosporine; systemic steroids for severe flares.
🎭 Other White Supporting Characters
| Character | Personality |
|---|---|
| Candidiasis (Pseudomembranous) | White curd-like plaques that CAN be wiped off, leaving a bleeding red base — the only white villain that gives itself away |
| Linea alba | Benign horizontal white line along the occlusal plane of buccal mucosa — completely innocent |
| Leukoedema | Diffuse grayish-white opalescence; disappears when mucosa is stretched — a variant of normal |
| Morsicatio | Ragged, shredded white from habitual cheek/lip biting — vanishes when the habit stops |
| White sponge nevus | Autosomal dominant; thick, folded, white oral mucosa from childhood |
ACT II: THE RED CHARACTERS 🔴
🔥 Character #4 — ERYTHROPLAKIA: "The Silent Inferno"
"I am small. I am red. I am quiet. And I am almost always malignant."
If leukoplakia is the most common villain, erythroplakia is the most dangerous one. It is the rarest oral OPMD (prevalence 0.02–0.83%) but carries a histological malignancy rate of approximately 90% — meaning nine out of ten erythroplakias already harbor severe dysplasia, carcinoma in situ, or invasive SCC at the time of biopsy.
Why is it red?
The epithelium is atrophic (thinned) — so thin that the underlying vasculature shines through. Combined with vascular dilation and subepithelial inflammation, the result is an intensely red, velvety patch.
Clinical signature:
- Asymptomatic, solitary, sharply demarcated red velvet patch
- Soft, velvety surface (occasionally pebbled/stippled)
- Most common sites: soft palate, floor of mouth, buccal mucosa
- Usually <1.5 cm, but deceptively quiet
- Induration = invasion has likely begun
Molecular fingerprint: High mutation rate of p53 tumor suppressor gene — a molecular screaming match that explains its aggressive behavior.
Diagnosis of exclusion — must rule out: erythematous candidiasis, atrophic lichen planus, lupus, pemphigus, cicatricial pemphigoid, Kaposi sarcoma, mechanical/thermal injury, amelanotic melanoma, and invasive SCC itself.
Mixed lesion alert: When erythroplakia and leukoplakia coexist → Speckled Erythroplakia (erythroleukoplakia). The red foci within the mixed lesion are the ones most prone to transformation.
Treatment: Biopsy immediately → if confirmed, surgical excision or CO₂ laser. Lesions >80 mm² carry a significantly higher recurrence risk post-excision.
🔴 Other Red Supporting Characters
| Character | Story |
|---|---|
| Erythematous candidiasis | Red, atrophic patches (no white film); classic on palate under dentures ("denture stomatitis") or midline dorsal tongue ("median rhomboid glossitis") |
| Geographic tongue | Smooth red patches with white borders on dorsal tongue, migrating over time — benign, no treatment needed |
| Atrophic glossitis | Smooth, bald, red tongue — a screaming signal for B12, iron, or folate deficiency |
| Kaposi sarcoma | Red-purple macular patches on the palate; AIDS-defining vascular neoplasm |
ACT III: THE SLOW STRANGLER 🧱
🎭 Character #5 — ORAL SUBMUCOUS FIBROSIS (OSMF): "The Concrete Wall"
"I start as a burn in your mouth. Then I quietly build walls — fibrous, relentless, invisible at first. One day, you realize you cannot open your mouth wide enough to eat. That is when I introduce myself."
OSMF is a chronic, insidious, progressive disease unique primarily to South and Southeast Asia — the direct price paid for the widespread habit of chewing areca (betel) nut. It is classified as an oral potentially malignant disorder, quietly laying down fibrosis until the mouth becomes a fortress that imprisons its own owner.
The culprit: Areca nut (Betel nut)
The arecoline alkaloid in areca nut stimulates fibroblasts to overproduce collagen and simultaneously inhibits collagenase (the enzyme that normally breaks collagen down). The result: collagen accumulates unchecked in the submucosa — literally building walls inside the mouth.
- Common forms: paan, gutka, pan masala, mawa, supari
- Also associated with heavily chili-seasoned diets
The natural history — a slow march:
Stage 1: Burning sensation → erythema (the mouth's SOS signal)
↓
Stage 2: Mucosal pallor — the pink fades to marble-white as fibrosis builds
↓
Stage 3: Fibrous bands appear — palpable cord-like structures in buccal mucosa,
palate, tonsillar pillars, fauces
↓
Stage 4: Trismus — mouth opening progressively restricted
↓
Stage 5: Tongue fixation — speech, swallowing impaired
↓
Stage 6: Ulceration + leukoplakic patches appear
↓
Stage 7 (~7–30% of cases): Malignant transformation → ORAL SCC


Histological signature:
- Atrophic epithelium sitting directly above submucosal fibrosis — the classic "juxtaposition of atrophic epithelium to subadjacent fibrosis"
- Loss of rete ridges, homogenized collagen bundles, reduced vascularity
- Chronic inflammatory cell infiltrate in early stages
Malignant transformation risk: 7–30% — wide range, but consistently alarming. It is one of the highest malignant transformation rates among all OPMDs.
Treatment:
- 🚫 Stop the areca nut — the single most important step (but fibrosis already laid down does NOT reverse)
- 💉 Intralesional injections — triamcinolone or dexamethasone ± hyaluronidase (to break down collagen)
- 🌿 Antioxidant therapy — spirulina (shown to reduce fibrosis and malignant transformation risk in trials)
- 🏋️ Physiotherapy — jaw-opening exercises to maintain function
- 🔪 Surgery — fibrous band release ± skin/mucosal grafting in advanced trismus; CO₂ laser ablation
- Surveillance for malignant transformation is lifelong
THE FINAL SCORECARD: Who Is the Most Dangerous?
| Villain | Prevalence | Malignant Transformation |
|---|---|---|
| Homogeneous leukoplakia | Common | ~1–2% |
| Non-homogeneous leukoplakia | Less common | ~4–7% |
| Proliferative verrucous leukoplakia | Rare | >50% |
| Oral lichen planus (erosive) | Common | 0–10% |
| Oral submucous fibrosis | Common in Asia | 7–30% |
| Speckled erythroplakia | Uncommon | 28–50% |
| Erythroplakia | Rarest | ~90% 🏆 |
THE GOLDEN DIAGNOSTIC RULES 🔑
Rule 1: Any lesion that cannot be scraped off → leukoplakia, OLP, hairy leukoplakia, OSMF Rule 2: Any lesion that can be scraped off → pseudomembranous candidiasis Rule 3: Bilateral + lacy white lines → oral lichen planus (reticular) Rule 4: Red + velvety + sharply demarcated → erythroplakia — BIOPSY TODAY Rule 5: Betel nut habit + burning + pale buccal bands + trismus → OSMF Rule 6: Corrugated lateral tongue + immunosuppressed → hairy leukoplakia (EBV) Rule 7: Any white or red lesion persisting >2 weeks after removing the irritant → BIOPSY, no excuses
Sources: Andrews' Diseases of the Skin (12th ed.), p. 709 | K.J. Lee's Essential Otolaryngology (11th ed.), pp. 65–107 | Fitzpatrick's Dermatology (9th ed.), pp. 1906–1909 | Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 683–684 | Cummings Otolaryngology Head and Neck Surgery (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.