Shoulder complex detailed notes
Reading File
Finding Sources
Finding Sources
Searching the Web
shoulder complex anatomy joints muscles detailed notes
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have all the core content needed. Let me compile the comprehensive detailed notes.
The Shoulder Complex - Detailed Notes
Sources: Gray's Anatomy for Students; Rheumatology, 2-Volume Set (Elsevier 2022); Campbell's Operative Orthopaedics 15th Ed; Rockwood & Green's Fractures in Adults 10th Ed
1. Overview
The shoulder complex is the most mobile articulation in the body. It connects the upper limb to the axial skeleton and comprises four joints working in unison:
- Glenohumeral (GH) joint - the true shoulder joint
- Acromioclavicular (AC) joint
- Sternoclavicular (SC) joint - the only true bony connection of the upper limb to the axial skeleton
- Scapulothoracic (ST) joint - a "floating" or physiological joint (not a true synovial joint)
The high mobility of the shoulder comes at the expense of bony stability. Stability is instead provided by muscles, ligaments, the glenoid labrum, and joint capsule.
2. Osteology (Bones)
Clavicle
- S-shaped bone connecting the sternum to the acromion
- Only bony connection between upper limb and axial skeleton
- Most commonly fractured at the middle third
- Medial end: rounded, articulates at SC joint
- Lateral end: flat, articulates at AC joint
- Provides attachment for: trapezius, deltoid, pectoralis major, sternocleidomastoid, subclavius
Scapula
- Triangular flat bone on the posterolateral thoracic wall (ribs 2-7)
- Key features:
- Glenoid cavity - shallow, oval fossa at the lateral angle; articulates with the humeral head
- Supraglenoid tubercle - attachment for long head of biceps brachii
- Infraglenoid tubercle - attachment for long head of triceps brachii
- Coracoid process - "crow's beak" projection; attachment for pectoralis minor, short head of biceps, coracobrachialis
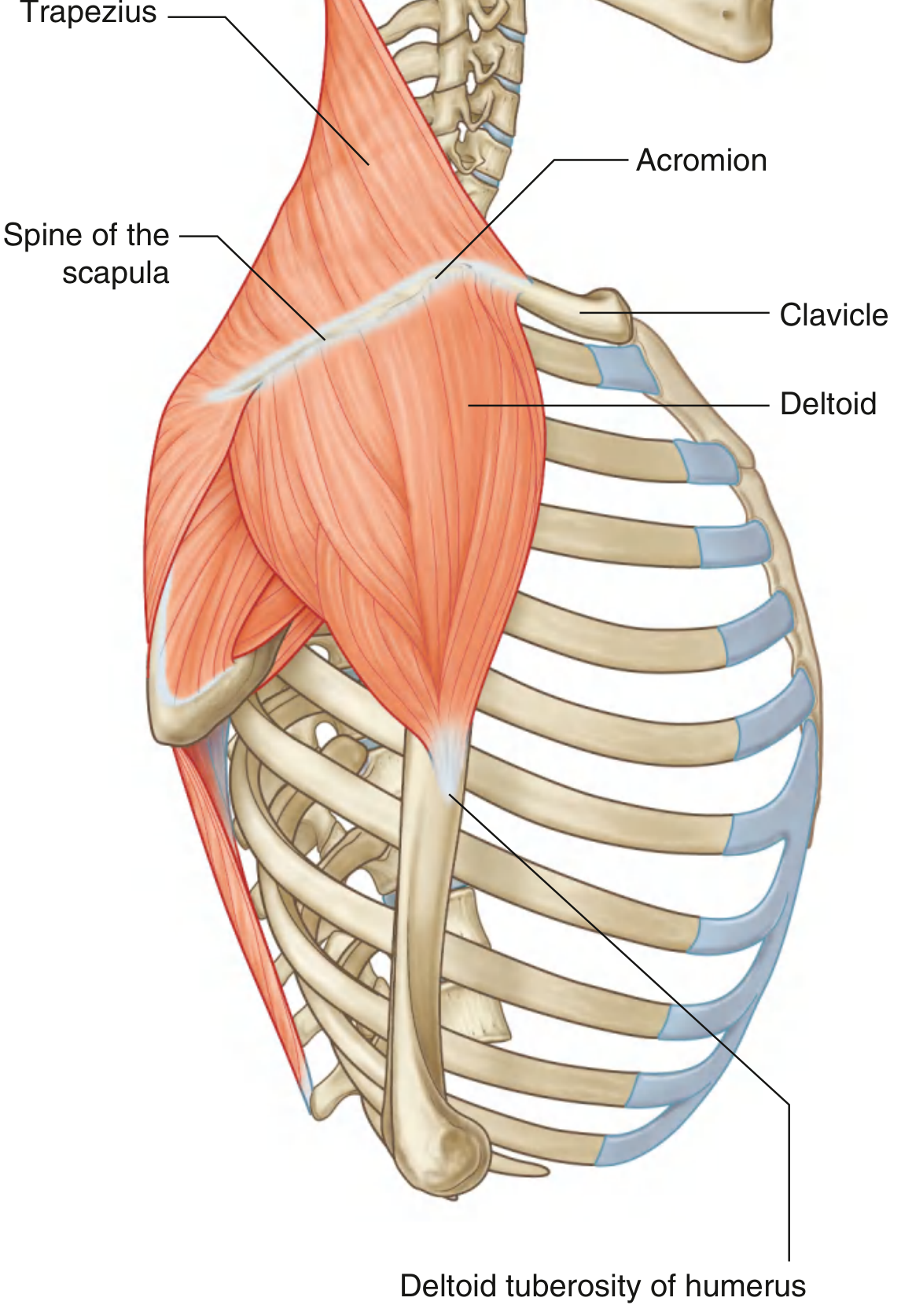
- Acromion - lateral extension of the spine; forms the AC joint
- Spine of scapula - posterior ridge; attachment for trapezius and deltoid
- Suprascapular notch - converted to foramen by superior transverse scapular ligament; transmits suprascapular nerve (artery passes above the ligament)
Humerus (Proximal)
- Head - large spherical; articulates with glenoid cavity; faces medially, superiorly, and posteriorly
- Anatomical neck - between head and tubercles; attachment for joint capsule
- Surgical neck - below the tubercles; common fracture site; axillary nerve at risk
- Greater tubercle - posterior and lateral; insertions: supraspinatus (superior facet), infraspinatus (middle facet), teres minor (inferior facet)
- Lesser tubercle - anterior; insertion: subscapularis
- Intertubercular sulcus (bicipital groove) - between tubercles; contains long head of biceps tendon held by transverse humeral ligament
3. The Four Joints of the Shoulder Complex
3.1 Glenohumeral (GH) Joint
The primary joint of the shoulder complex.
Type: Synovial ball-and-socket; multiaxial
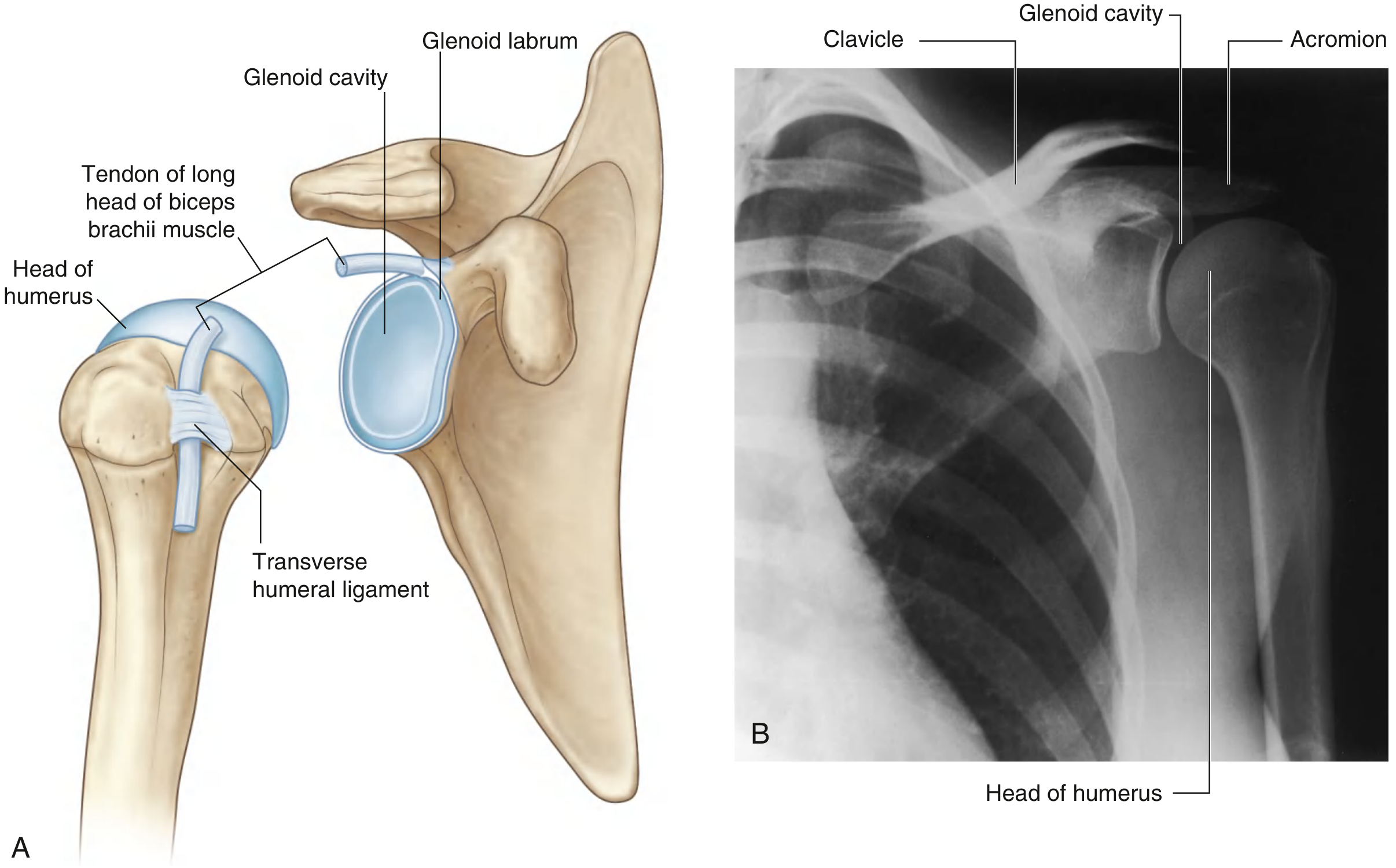
Articular surfaces:
- Head of humerus (large) - covered by hyaline cartilage
- Glenoid cavity of scapula (small, shallow) - covered by hyaline cartilage
- The glenoid is only ~1/4 the size of the humeral head
Glenoid Labrum:
- Fibrocartilaginous collar deepening and expanding the glenoid peripherally
- Attaches to the margin of the glenoid fossa
- Superiorly continuous with the tendon of the long head of biceps brachii (attaches at supraglenoid tubercle)
- Increases contact area and contributes to stability
Joint Capsule:
- Fibrous membrane attaches to glenoid margin (outside labrum) and anatomical neck of humerus
- Medially, the capsule attaches lower - extending onto the shaft of humerus
- Loose inferiorly - this redundant area accommodates abduction of the arm
- The inferior "axillary recess" is a key feature; it is taut in adduction, lax in abduction
Ligaments of the GH Joint:
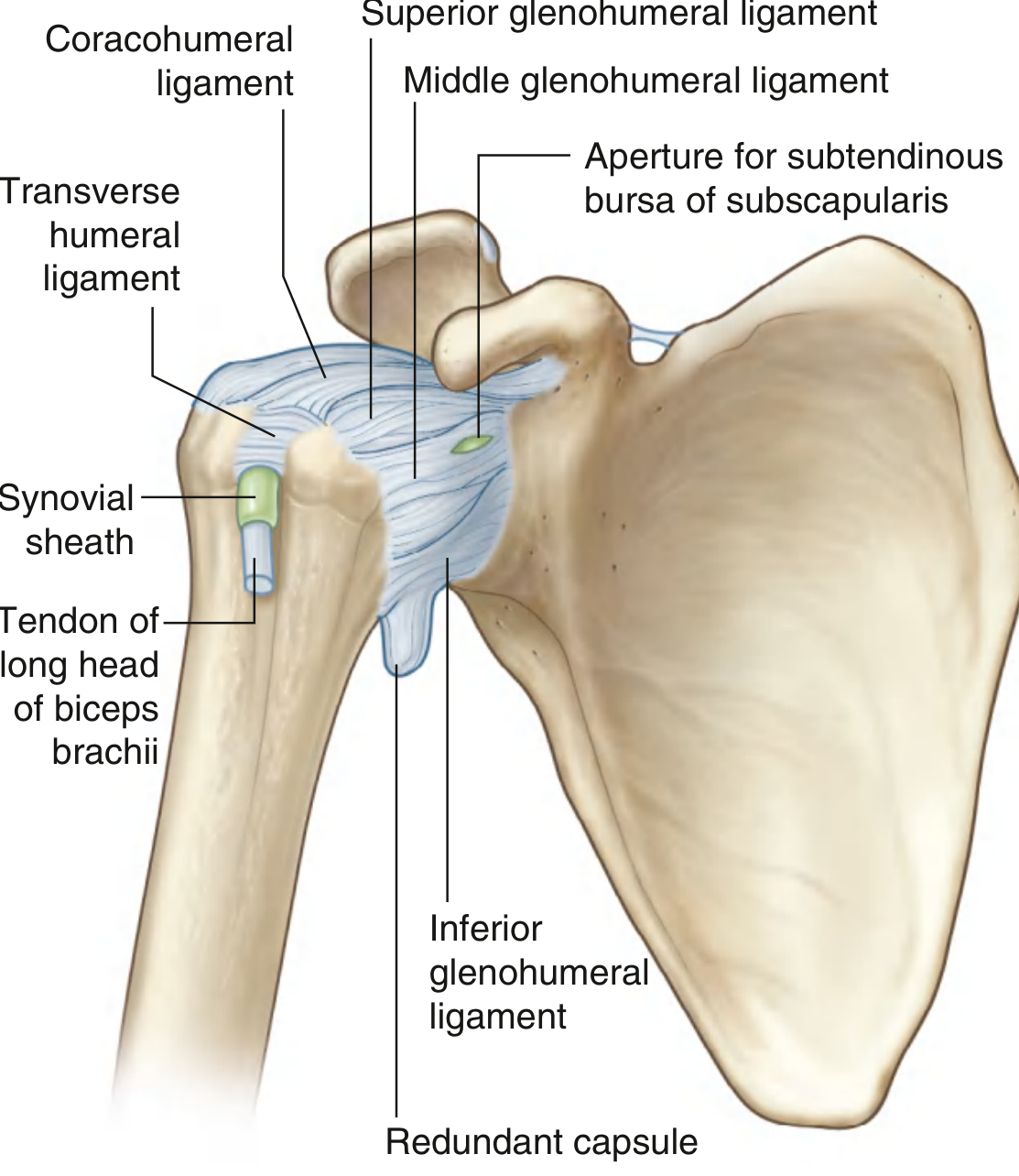
| Ligament | Attachment | Function |
|---|---|---|
| Superior glenohumeral ligament (SGHL) | Superomedial glenoid → lesser tubercle | Limits inferior translation; restrains external rotation in adduction |
| Middle glenohumeral ligament (MGHL) | Superomedial glenoid → lesser tubercle | Limits external rotation; variable in size |
| Inferior glenohumeral ligament (IGHL) | Inferior glenoid rim/labrum → anatomical neck | Primary stabilizer against anterior dislocation with arm abducted; has anterior band, axillary pouch, posterior band |
| Coracohumeral ligament | Base of coracoid → greater tubercle | Limits inferior translation; limits external rotation when arm is adducted |
| Transverse humeral ligament | Greater tubercle → lesser tubercle | Holds biceps tendon in the intertubercular sulcus |
Synovial Membrane:
- Lines the fibrous capsule; attaches to margins of articular surfaces
- Loose inferiorly
- Protrudes through apertures to form bursae:
- Subtendinous bursa of subscapularis (most consistent) - between subscapularis and fibrous membrane
- Folds around and extends along the biceps tendon into the intertubercular sulcus
Bursae of the Shoulder (not communicating with joint):
- Subacromial (subdeltoid) bursa - between acromion/deltoid and supraspinatus/joint capsule - the most clinically significant
- Subcoracoid bursa - between coracoid process and joint capsule
- Bursa between acromion and skin
- Additional bursae near coracobrachialis, teres major, long head of triceps, and latissimus dorsi
Coracoacromial Arch:
- Formed by the coracoid process, coracoacromial ligament, and acromion
- Creates a protective arch superiorly over the GH joint
- The supraspinatus tendon + subacromial bursa pass beneath this arch → site of subacromial impingement
Vascular Supply: Anterior and posterior circumflex humeral arteries + suprascapular artery (branches of axillary artery)
Innervation: Branches from posterior cord of brachial plexus; suprascapular nerve (C5,C6), axillary nerve (C5,C6), lateral pectoral nerve
Movements and Range of Motion:
| Movement | Normal ROM | Primary Muscles |
|---|---|---|
| Flexion | 0-180° | Anterior deltoid, pectoralis major (clavicular), coracobrachialis, biceps |
| Extension | 0-60° | Posterior deltoid, teres major, latissimus dorsi |
| Abduction | 0-180° | Middle deltoid + supraspinatus (0-90°), trapezius + serratus anterior (90-180°) |
| Adduction | 0-50° | Pectoralis major, latissimus dorsi, teres major |
| Internal rotation | 0-70° | Subscapularis, pectoralis major, latissimus dorsi, teres major |
| External rotation | 0-90° | Infraspinatus, teres minor, posterior deltoid |
| Circumduction | Full arc | Combination of above |
3.2 Acromioclavicular (AC) Joint
Type: Plane synovial joint (diarthrodial)
Articular surfaces: Lateral end of clavicle + medial surface of acromion - both covered by fibrocartilage
Intra-articular disc: Often present but incomplete; degenerates with age
Ligaments:
- AC ligaments (capsular): Reinforce the joint capsule; resist anteroposterior translation
- Coracoclavicular ligament (CC): Primary vertical stabilizer of the AC joint
- Conoid ligament - posterior and medial; cone-shaped; from coracoid base to conoid tubercle of clavicle
- Trapezoid ligament - anterior and lateral; from coracoid to trapezoid ridge of clavicle
Clinical - AC Joint Injuries (Shoulder Separation):
- Minor injury: tears AC capsule/ligaments → AC separation on X-ray
- Severe injury: disrupts CC ligaments (conoid + trapezoid) → elevation and upward subluxation of clavicle
- Classified by Rockwood classification (Types I-VI)
3.3 Sternoclavicular (SC) Joint
Type: Diarthrodial saddle joint (the only true joint connecting upper limb to axial skeleton)
Articular surfaces: Medial end of clavicle + manubrium of sternum + first costal cartilage
Intra-articular disc: Present; improves congruence; acts as a shock absorber
Ligaments:
- Anterior SC ligament - primary restraint against superior displacement
- Posterior SC ligament - strongest; primary restraint against anteroposterior (AP) instability
- Costoclavicular ligament - from first rib/cartilage to medial clavicle; limits elevation
- Interclavicular ligament - between medial ends of both clavicles across the jugular notch
Movements: Elevation/depression (~35°), protraction/retraction (~35°), rotation (~50°)
Clinical importance: Posterior dislocation is a surgical emergency (can compress trachea, great vessels, or esophagus)
3.4 Scapulothoracic (ST) Joint
Type: Physiological joint (not a true synovial joint) - a functional articulation between the anterior surface of the scapula and the posterior thoracic wall
Stability: Maintained entirely by muscles - serratus anterior (primary), trapezius, rhomboids, levator scapulae
Movements: Elevation, depression, protraction (abduction), retraction (adduction), upward rotation, downward rotation
Scapulohumeral Rhythm:
- The coordinated movement between GH and ST joints during arm elevation
- Classic ratio: 2:1 (for every 3° of total arm elevation, 2° occurs at GH and 1° at ST)
- In the first 30° of abduction: movement mostly at GH with ST "setting"
- Above 90°: increasing contribution of ST motion
- Disturbance of this rhythm (scapular dyskinesia) causes secondary subacromial impingement
4. Muscles of the Shoulder Complex
4.1 Scapular Stabilizers (Extrinsic Muscles)
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Trapezius | Superior nuchal line, ext. occipital protuberance, ligamentum nuchae (C-spine), spinous processes T1-T12 | Spine of scapula, acromion, posterior border of lateral 1/3 of clavicle | Accessory nerve (CN XI) + C3,C4 (sensory/proprioception) | Upper: elevates scapula; Middle: retracts; Lower: depresses; Overall: upward rotation for abduction above 90° |
| Serratus Anterior | Ribs 1-9 (outer surfaces) | Costal surface of medial border of scapula | Long thoracic nerve (C5,C6,C7) | Protracts and holds scapula against thoracic wall; upward rotation (critical for full elevation) |
| Rhomboid Major | Spinous processes T2-T5 | Medial border of scapula (inferior to spine) | Dorsal scapular nerve (C4,C5) | Retracts + elevates scapula; downward rotation |
| Rhomboid Minor | Ligamentum nuchae, C7-T1 spinous processes | Medial border of scapula (at root of spine) | Dorsal scapular nerve (C5) | Retracts + elevates scapula |
| Levator Scapulae | Transverse processes C1-C4 | Posterior surface, medial border of scapula (superior angle to spine) | C3, C4 direct + dorsal scapular nerve (C5) | Elevates scapula; downward rotation |
| Pectoralis Minor | Ribs 3-5 (outer surface) | Coracoid process | Medial pectoral nerve (C8,T1) | Protracts and depresses scapula; tilts scapula anteriorly |
Key clinical note: Serratus anterior paralysis (long thoracic nerve injury) = winged scapula (medial border protrudes away from thorax)
4.2 The Rotator Cuff (SITS)
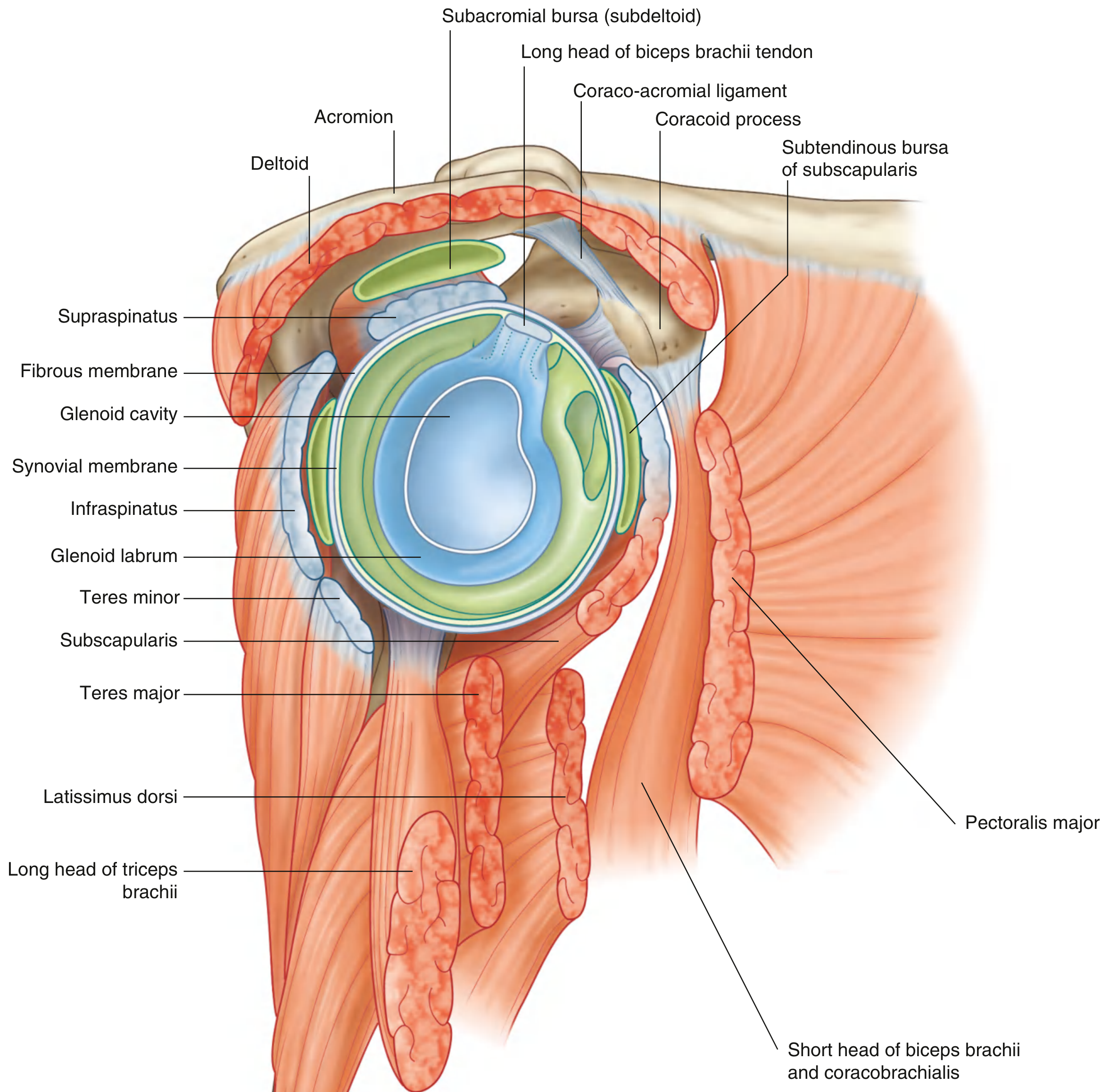
The rotator cuff tendons blend with the joint capsule, providing dynamic stability by holding the humeral head in the glenoid cavity.
| Muscle | Origin | Insertion | Nerve | Primary Action |
|---|---|---|---|---|
| Supraspinatus (S) | Supraspinous fossa of scapula | Superior facet of greater tubercle | Suprascapular nerve (C5,C6) | Initiates abduction (first 15°); holds humeral head in glenoid |
| Infraspinatus (I) | Infraspinous fossa of scapula | Middle facet of greater tubercle | Suprascapular nerve (C5,C6) | External rotation of humerus; posterior stabilizer |
| Teres Minor (T) | Posterior surface of lateral scapular border (upper 2/3) | Inferior facet of greater tubercle | Axillary nerve (C5,C6) | External rotation; inferior stabilizer |
| Subscapularis (S) | Subscapular fossa (anterior scapula) | Lesser tubercle and crest below | Upper and lower subscapular nerves (C5,C6,C7) | Medial (internal) rotation; anterior stabilizer - only anterior cuff muscle |
Mnemonic: SITS (Supraspinatus, Infraspinatus, Teres minor, Subscapularis)
Rotator Interval: The region between the anterior edge of supraspinatus and the superior edge of subscapularis, containing:
- Coracohumeral ligament
- Superior glenohumeral ligament
- Long head of biceps tendon
Clinical - Rotator Cuff Disorders:
- Subacromial impingement: Supraspinatus tendon impinges under the coracoacromial arch; fixed dimensions of the space means any swelling (tendinopathy, fluid, bone spur) causes pain with abduction (particularly 60-120° - the "painful arc")
- Supraspinatus most commonly torn - passes under the narrowest part of the arch; watershed zone of poor vascularity near its insertion
- Tears: partial (articular surface, bursal surface, or intrasubstance) or full-thickness
4.3 Deltoid and Other GH Movers
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Deltoid | Spine of scapula, acromion, anterior border of lateral 1/3 of clavicle | Deltoid tuberosity (lateral humerus) | Axillary nerve (C5,C6) | Major abductor (middle part); anterior part: flexion + medial rotation; posterior part: extension + lateral rotation |
| Pectoralis Major | Clavicle (medial 1/2), sternum, costal cartilages 1-6 | Lateral lip of intertubercular sulcus | Medial + lateral pectoral nerves (C5-T1) | Flexion, adduction, medial rotation; clavicular head flexes; sternocostal head extends from flexion |
| Latissimus Dorsi | Spinous processes T7-T12, thoracolumbar fascia, iliac crest, lower ribs | Medial lip of intertubercular sulcus (floor of bicipital groove) | Thoracodorsal nerve (C6,C7,C8) | Extension, adduction, medial rotation ("hand-behind-back") |
| Teres Major | Posterior surface of inferior angle of scapula | Medial lip of intertubercular sulcus | Lower subscapular nerve (C5,C6,C7) | Medial rotation, extension, adduction of humerus |
| Coracobrachialis | Coracoid process | Medial surface of humerus (mid-shaft) | Musculocutaneous nerve (C6,C7) | Flexion and adduction |
4.4 Long Head of Biceps Brachii
- Origin: supraglenoid tubercle (intra-articular, extra-synovial)
- Passes through the joint cavity superior to the humeral head
- Exits through the intertubercular sulcus held by the transverse humeral ligament
- Role: Restricts upward migration of humeral head (weak GH depressor); acts as humeral head stabilizer
- Innervation: Musculocutaneous nerve (C5,C6)
- Clinical: SLAP (Superior Labrum Anterior to Posterior) tears involve the biceps anchor at the supraglenoid tubercle
5. Neurovascular Supply
Brachial Plexus - Key Nerves
| Nerve | Roots | Muscles Supplied | Clinical Note |
|---|---|---|---|
| Axillary nerve | C5,C6 (posterior cord) | Deltoid, teres minor | At risk in anterior GH dislocation and surgical neck fractures; passes through quadrangular space; loss → deltoid paralysis, loss of shoulder contour, sensory loss over regimental badge area (lateral upper arm) |
| Suprascapular nerve | C5,C6 (superior trunk) | Supraspinatus, infraspinatus | Passes through suprascapular foramen (under the ligament, unlike artery which passes above); at risk in overhead athletes; ganglion cysts at spinoglenoid notch affect only infraspinatus |
| Long thoracic nerve | C5,C6,C7 | Serratus anterior | Injury → winged scapula; can be damaged in radical mastectomy, rib resection, or direct blow |
| Dorsal scapular nerve | C5 (sometimes C4,C5) | Rhomboids, levator scapulae | Passes through middle scalene |
| Upper subscapular nerve | C5,C6 (posterior cord) | Subscapularis (upper) | - |
| Lower subscapular nerve | C5,C6 (posterior cord) | Subscapularis (lower), teres major | - |
| Thoracodorsal nerve | C6,C7,C8 (posterior cord) | Latissimus dorsi | Runs with thoracodorsal vessels; at risk in axillary dissection |
Quadrangular Space
- Formed by: teres minor (superior), teres major (inferior), long head of triceps (medial), surgical neck of humerus (lateral)
- Contains: Axillary nerve and posterior circumflex humeral artery
Triangular Space
- Formed by: long head of triceps (lateral), teres minor (superior), teres major (inferior)
- Contains: Circumflex scapular artery
Triangular Interval
- Formed by: long head of triceps (medial), humerus (lateral), teres major (superior)
- Contains: Radial nerve and profunda brachii artery
Blood Supply
- Axillary artery (continuation of subclavian at lateral border of 1st rib) gives:
- Superior thoracic artery
- Thoracoacromial artery (acromial, clavicular, deltoid, pectoral branches)
- Lateral thoracic artery
- Anterior circumflex humeral artery (smaller; supplies bicipital groove area, anterior GH capsule)
- Posterior circumflex humeral artery (larger; passes through quadrangular space; supplies deltoid, posterior GH joint, greater tubercle)
- Subscapular artery → thoracodorsal + circumflex scapular
6. Scapulohumeral Rhythm in Detail
During elevation of the arm:
- 0-30°: mostly GH motion ("setting phase" of scapula)
- 30-180°: 2:1 ratio - GH contributes 2° for every 1° of scapular rotation on the thorax
- Full elevation (180°): ~120° at GH + ~60° at ST
This rhythm requires coordinated action of:
- Trapezius (upper + lower) and serratus anterior - the "force couple" for scapular upward rotation
- Deltoid and supraspinatus - force couple for GH abduction
7. Gateways and Clinical Spaces
Suprascapular Foramen
- Suprascapular notch + superior transverse scapular ligament
- Suprascapular nerve passes through the foramen
- Suprascapular artery and vein pass above the ligament (mnemonic: "army goes under the bridge; navy sails over")
Subcoracoid/Coracoacromial Arch
- Formed by: coracoid process + coracoacromial ligament + acromion
- The supraspinatus and subacromial bursa pass beneath this arch
- Site of subacromial impingement syndrome
- Acromion morphology types (Bigliani):
- Type I: flat
- Type II: curved
- Type III: hooked (highest risk of impingement and rotator cuff tears)
8. Clinical Correlations
Anterior GH Dislocation
- Most common direction (>95%)
- Head typically dislocates anteroinferiorly (subcoracoid position)
- Bankart lesion: tear of anteroinferior glenoid labrum (with/without bony fragment)
- Hill-Sachs lesion: compression fracture of posterolateral humeral head
- Axillary nerve is at risk (test deltoid function and sensation after reduction)
Posterior GH Dislocation
- Rare (~2%); often missed
- Associations: seizures, electrocution, direct blow
- "Lightbulb sign" on AP X-ray (humerus internally rotated)
- Reverse Hill-Sachs (McLaughlin lesion) on anteromedial humeral head
Rotator Cuff Disorders
- Painful arc: 60-120° of abduction (supraspinatus impingement)
- Supraspinatus tears: full-thickness tears → inability to initiate abduction or maintain against resistance
- Infraspinatus/teres minor: external rotation weakness
- Subscapularis tears: internal rotation weakness; positive lift-off test, belly press test
Frozen Shoulder (Adhesive Capsulitis)
- Contraction of GH joint capsule, particularly the rotator interval and IGHL axillary pouch
- Progressive loss of all GH movements, especially external rotation and abduction
AC Joint Injury (Shoulder Separation)
- Rockwood Types I-III most common (I: sprain, II: AC torn + CC intact, III: both torn)
- Types IV-VI are rare and require surgery
Clavicle Fractures
- Most common fracture in upper limb
- Middle third (80%): proximal fragment pulled up by SCM; distal fragment pulled down by weight of arm
- Lateral third: if CC ligament torn, displacement can occur
9. Summary Table - The Four Joints at a Glance
| Feature | GH Joint | AC Joint | SC Joint | ST Joint |
|---|---|---|---|---|
| Type | Synovial ball-and-socket | Plane synovial | Saddle synovial | Physiological |
| Disc | No | Incomplete | Complete | N/A |
| Primary stabilizer | Rotator cuff + IGHL | Coracoclavicular lig. | Posterior SC lig. | Serratus anterior |
| Innervation | Axillary, suprascapular | Suprascapular, lateral pectoral | Supraclavicular nerve | Multiple |
| Common pathology | Dislocation, cuff tears | Separation | Dislocation | Winging (serratus palsy) |
Sources: Gray's Anatomy for Students (Elsevier); Rheumatology, 2-Volume Set (Elsevier 2022); Campbell's Operative Orthopaedics 15th Ed 2026; Rockwood and Green's Fractures in Adults 10th Ed 2025
This is a shared conversation. Sign in to Orris to start your own chat.