Successful thrombolysis in cva
Reading File
Finding Sources
Searching PubMed
"thrombolysis" AND "ischemic stroke" AND "outcomes"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Thrombolysis in Ischaemic Stroke (CVA) - Successful Use
Thrombolysis in ischaemic stroke (CVA) refers to the pharmacological dissolution of the occluding thrombus using intravenous recombinant tissue plasminogen activator (rt-PA). When administered correctly and within the appropriate time window, it is the most evidence-based intervention to reduce disability and death.
Mechanism of Action
rt-PA (alteplase, tenecteplase) activates plasminogen bound to fibrin within the clot, converting it to plasmin. Plasmin then degrades fibrin, dissolving the thrombus and restoring blood flow to the ischaemic penumbra (viable but non-functional brain tissue) before it progresses to infarction.
Agents and Dosing
| Agent | Dose | Route | Notes |
|---|---|---|---|
| Alteplase | 0.9 mg/kg IV (max 90 mg) - 10% as bolus over 1 min, remainder over 60 min | IV | FDA-approved; primary agent |
| Tenecteplase | 0.25 mg/kg (max 25 mg) single IV bolus | IV | Non-inferior to alteplase; easier to administer; preferred pre-thrombectomy |
Do not use abbreviations (rtPA, TNK) when ordering - use full generic names to avoid medication errors. Doses differ between stroke, STEMI, and PE indications.
Time Windows
Within 3 Hours
Strong evidence from NINDS trial and multiple RCTs. IV alteplase 0.9 mg/kg is recommended for all eligible patients ≥18 years, regardless of age (including >80 years), stroke severity (mild-disabling to severe), with no upper age limit.
3 to 4.5 Hours
Supported by ECASS III (OR 1.34, 95% CI 1.02-1.76 for favourable outcome). AHA/ASA recommends alteplase in this window only if all of the following apply:
- Age ≤80 years
- No history of both diabetes mellitus AND prior stroke
- NIHSS score ≤25
- Not on oral anticoagulants
- No imaging evidence of ischaemia >1/3 of the MCA territory
Beyond 4.5 Hours
Benefit is not established with standard criteria. However, the WAKE-UP trial demonstrated that MRI-guided thrombolysis (DWI-positive/FLAIR-negative mismatch) can benefit patients with unknown onset (e.g. wake-up strokes). At 90 days, 53.3% of alteplase patients achieved mRS 0-1 vs 41.8% in placebo (adjusted OR 1.61).
A 2025 meta-analysis (PMID 39882605) supports thrombolysis beyond 4.5 hours in selected patients with perfusion-diffusion mismatch.
DWI-FLAIR Mismatch (Wake-Up Stroke)
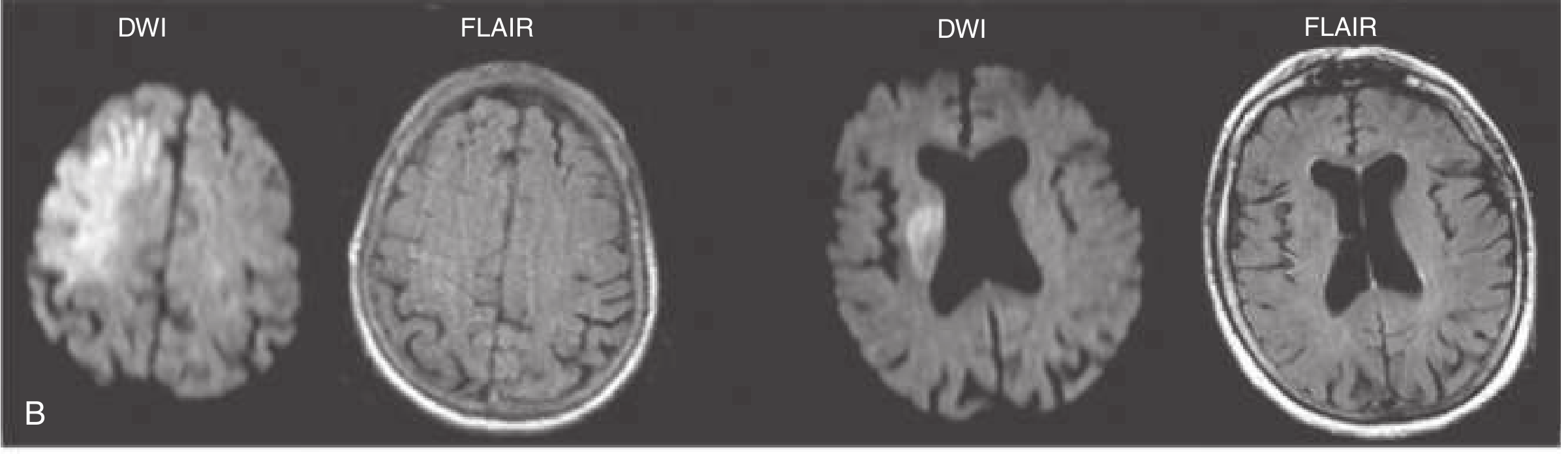
DWI shows acute ischaemia but FLAIR is negative = recent stroke (<4.5 h physiological age) - candidate for thrombolysis.
Inclusion Criteria (AHA/ASA 2019)
- Diagnosis of acute ischaemic stroke with measurable neurological deficit
- Symptom onset (or last known well time) within 3 h (or 3-4.5 h with stricter criteria)
- Age ≥18 years
- No contraindications
Exclusion Criteria (Key)
| Absolute | Relative |
|---|---|
| Intracranial haemorrhage on imaging | Recent surgery within 14 days |
| Subarachnoid haemorrhage | Minor/nondisabling stroke symptoms |
| Severe head trauma within 3 months | Blood glucose <50 or >400 mg/dL |
| Prior intracranial surgery within 3 months | Platelet count <100,000 |
| SBP >185 mmHg or DBP >110 mmHg (refractory) | INR >1.7 or aPTT elevated |
| GI/GU bleeding within 21 days | History of prior stroke + diabetes |
| Active internal bleeding | Pregnancy |
For the 3-4.5 h window, age >80, prior stroke + DM, NIHSS >25, and imaging showing >1/3 MCA territory ischaemia are added exclusions.
Monitoring After Alteplase
- Blood pressure: Check every 15 min during infusion, then every 30 min for 6 h, then hourly for 16 h
- BP targets: Maintain SBP ≤180 mmHg, DBP ≤105 mmHg throughout
- If SBP 180-230 or DBP 105-120 mmHg: Labetalol 10 mg IV, may repeat; or nicardipine infusion 5 mg/h titrated to effect
- Blood glucose: Keep 140-180 mg/dL; treat hypoglycaemia (<60 mg/dL) with IV dextrose
- No antithrombotic agents (heparin, aspirin, clopidogrel) for 24 hours post-alteplase
- Repeat CT head at 24 hours before starting anticoagulation/antiplatelets
Complications
| Complication | Incidence |
|---|---|
| Symptomatic intracranial haemorrhage | 2-7% |
| Asymptomatic intracranial haemorrhage / microbleeds | 30-45% |
| Angioedema (orolingual) | ~1-2% |
| Systemic haemorrhage | Rare |
Risk of ICH is lowest in patients with low NIHSS score, no hypertension, no diabetes, and age <70 years.
Indicators of Successful Thrombolysis
Clinical signs of reperfusion ("thrombolysis success") include:
- Neurological improvement - fall in NIHSS score by ≥4 points (or to 0-1) within 24 h
- Resolution of focal deficits - limb power, speech, visual field recovery
- Imaging evidence - follow-up CT/MRI showing no new infarction or reduced DWI lesion volume; CTA/MRA demonstrating vessel recanalisation
- Modified Rankin Scale (mRS) 0-2 at 90 days is the standard trial endpoint for good functional outcome
Tenecteplase vs Alteplase - Current Evidence
The EXTEND-IA TNK trial showed tenecteplase was associated with higher reperfusion rates and better functional outcomes compared to alteplase in patients proceeding to thrombectomy. A 2023 meta-analysis (PMID 38108256) also addresses thrombolysis in patients on anticoagulants. Tenecteplase is now preferred over alteplase in patients eligible for mechanical thrombectomy due to its simpler bolus dosing.
Key Points Summary
- Time is brain: for every 1 minute of treatment delay, ~1.9 million neurons are lost
- "Last known well" time determines eligibility, not time of discovery
- Mild nondisabling stroke (NIHSS 0-5, not affecting ADLs) - thrombolysis NOT recommended (PRISMS trial)
- Mild disabling stroke - thrombolysis IS recommended within 4.5 h
- Thrombolysis and mechanical thrombectomy are complementary; thrombectomy can proceed even after IV alteplase
- IV thrombolytics should be given even when endovascular therapy is being planned within 4.5 h
Sources: Rosen's Emergency Medicine (9th ed.), Tintinalli's Emergency Medicine (9th ed.), 2019 AHA/ASA Stroke Guidelines. Recent updates: PMID 38324409 (JAMA 2024 meta-analysis on thrombolysis timing before thrombectomy), PMID 39882605 (Stroke 2025 meta-analysis on extended window thrombolysis).
This is a shared conversation. Sign in to Orris to start your own chat.