What causes pedal edema in pregnancy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a detailed, textbook-supported answer on the causes of pedal edema in pregnancy:
Causes of Pedal Edema in Pregnancy
Pedal (ankle/foot) edema is present in up to 80% of normal pregnancies. It arises from several converging physiological mechanisms:
1. Massive Plasma Volume Expansion
Plasma volume begins rising at 6-8 weeks' gestation and reaches a peak of 4,700-5,200 mL by 32 weeks - an increase of 45% (1,200-1,600 mL) above non-pregnant values. Total body water increases by 6-8 liters, distributed between the plasma compartment and the interstitial space. The interstitial expansion is what manifests clinically as edema. There is also cumulative retention of approximately 950 mmol of sodium distributed between maternal extracellular compartments and the fetus.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 208 & 213
- Brenner and Rector's The Kidney, p. 2140
2. RAAS Activation and Sodium/Water Retention
The renin-angiotensin-aldosterone system (RAAS) is activated in pregnancy. Nitric oxide-mediated vasodilation triggers the RAAS, promoting renal sodium and water retention. Renal interstitial compliance increases, and interstitial pressure remains low despite increased renal interstitial volume - this attenuates the normal renal pressure-natriuresis response, further promoting fluid retention.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 208
- Brenner and Rector's The Kidney, p. 2140
3. Reduced Colloid Osmotic Pressure (Hypoalbuminemia)
Plasma volume increases disproportionately to protein mass, causing hemodilution and a fall in serum albumin (physiologic hypoalbuminemia). Albumin is the major contributor to colloid osmotic pressure (COP) - the force that holds fluid within the capillary. The drop in COP during pregnancy shifts the Starling forces toward net filtration of fluid into the interstitium, promoting dependent edema. This also raises the risk of pulmonary edema in complicated pregnancies (preeclampsia, sepsis, hemorrhage).
- Creasy & Resnik's Maternal-Fetal Medicine, p. 214
4. Mechanical Compression of the Inferior Vena Cava (IVC)
As the uterus enlarges, it compresses the inferior vena cava, particularly when the patient is supine or standing. This:
- Increases hydrostatic pressure in the lower limb veins
- Reduces venous return from the legs
- Promotes transudation of fluid into the interstitial space of the feet and ankles
This mechanical effect worsens progressively as pregnancy advances into the third trimester and explains why the edema is almost always bilateral and worse by end of day (gravitational/dependent).
- Robbins & Kumar Basic Pathology, p. 3343
- Campbell Walsh Wein Urology, p. 2583
5. Hormonal Effects (Progesterone and Estrogen)
- Progesterone promotes smooth muscle relaxation, reducing venous tone and increasing venous capacitance, which contributes to venous pooling in the lower limbs.
- Estrogen stimulates hepatic production of angiotensinogen and promotes aldosterone-mediated sodium retention, further expanding extracellular volume.
- Relaxin (a peptide hormone rising in pregnancy) also promotes systemic vasodilation and increases vascular permeability, contributing to the edematous tendency.
6. Increased Capillary Permeability
Rising levels of vascular endothelial growth factor (VEGF), produced in part by the placenta, increase capillary permeability throughout pregnancy. This allows more fluid to leak from capillaries into the interstitium, particularly in dependent areas.
Summary: Starling Forces in Pregnancy
| Factor | Change in Pregnancy | Effect on Edema |
|---|---|---|
| Capillary hydrostatic pressure | Increased (IVC compression) | Promotes edema |
| Plasma colloid osmotic pressure | Decreased (dilutional hypoalbuminemia) | Promotes edema |
| Interstitial hydrostatic pressure | Relatively low | Promotes edema |
| Sodium/water retention (RAAS) | Increased | Promotes edema |
| Venous capacitance (progesterone) | Increased | Promotes edema |
Clinical Note
Physiological pedal edema in pregnancy is pitting, bilateral, worsens in the evening, and is not associated with hypertension or proteinuria. Edema that is accompanied by hypertension (>140/90 mmHg) and proteinuria (>300 mg/24h) should raise suspicion for preeclampsia, where the mechanism shifts toward pathological endothelial dysfunction, decreased GFR, and more severe hypoalbuminemia. As noted in Bradley & Daroff's Neurology, edema alone is now considered too ubiquitous and nonspecific in pregnancy to be diagnostic of preeclampsia.
What is the mechanism of pain during wisdom tooth eruption
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
mechanism of pain wisdom tooth eruption pericoronitis inflammatory mediators
I now have sufficient information from textbook sources and web supplementation to give a comprehensive answer.
Mechanism of Pain During Wisdom Tooth Eruption
Pain from wisdom tooth (third molar) eruption is not a single event - it results from several overlapping anatomical, mechanical, and inflammatory mechanisms acting simultaneously.
1. Mechanical Pressure on the Periodontal Ligament and Bone
As the third molar moves through the alveolar bone toward the surface, it exerts pressure on the surrounding bony crypt and periodontal ligament (PDL). The PDL is densely supplied with mechanoreceptors and nociceptors (A-delta and C-fibers from the inferior alveolar branch of the trigeminal nerve - V3). Sustained pressure on these receptors directly triggers pain signals.
When the tooth is impacted (most commonly mesioangular impaction), it presses against the roots of the adjacent second molar or into the ascending ramus of the mandible. This creates a zone of ischemia and bone remodeling around the crown, generating a dull, deep, constant ache characteristic of bone pain.
2. Gingival Tissue Stretching and Rupture
As the crown pierces through the overlying mucosa and gingiva, the tissue is stretched and torn. This directly activates tissue nociceptors and releases local inflammatory mediators including:
- Bradykinin - a potent sensitizer of free nerve endings
- Prostaglandins (PGE2) - lower the pain threshold of nociceptors (peripheral sensitization)
- Histamine and serotonin - from mast cells and platelets in the traumatized tissue
- Substance P and CGRP - released from the nociceptor terminals themselves (neurogenic inflammation), causing local vasodilation and plasma extravasation (flare reaction)
This is the same peripheral sensitization mechanism underlying all inflammatory pain.
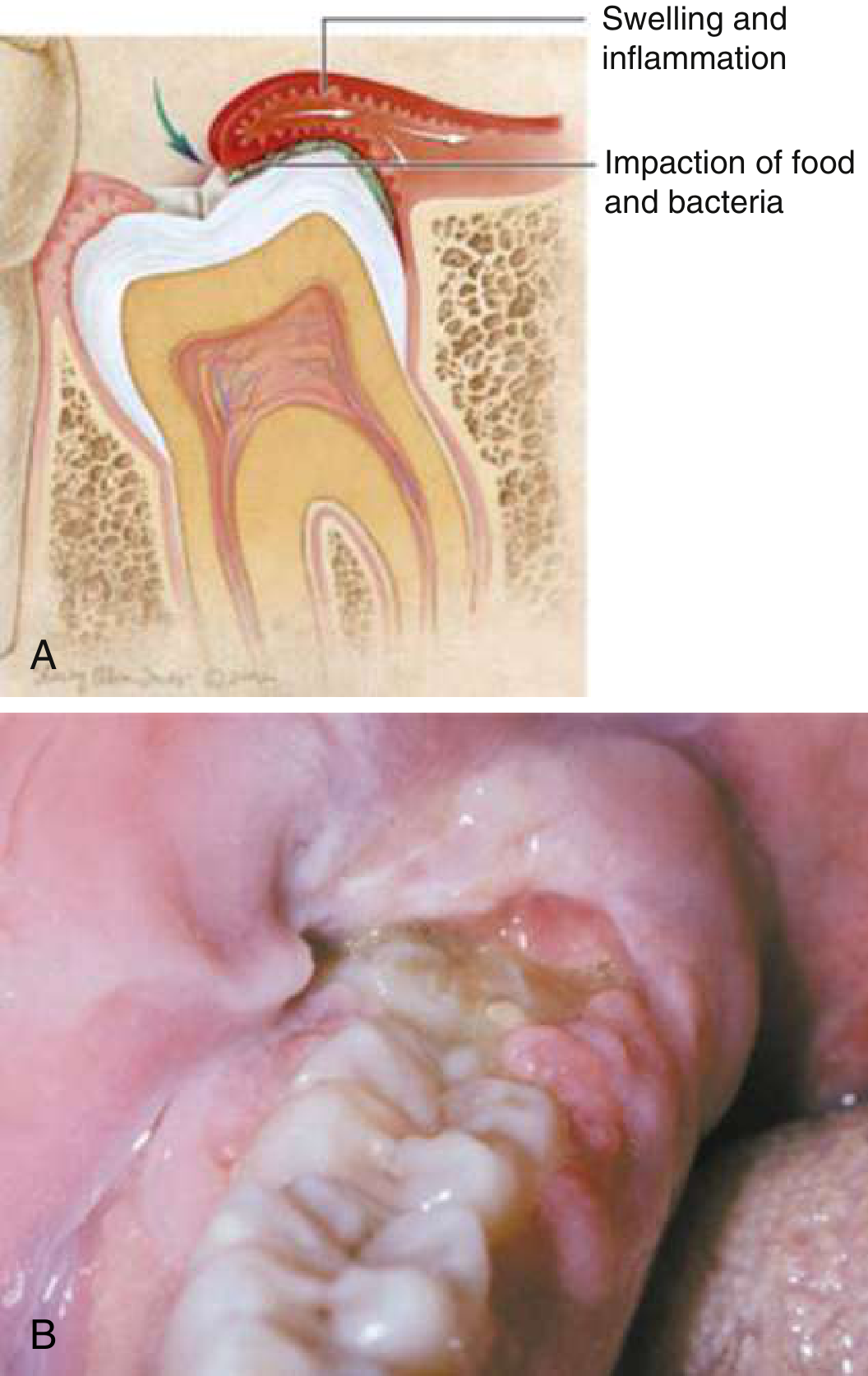
3. Pericoronitis - The Major Source of Acute Pain
This is the single most common and severe cause of third molar pain, occurring when the tooth only partially erupts.
Pathophysiology step by step:
- The crown partially erupts but remains covered by a flap of gingival tissue called the operculum
- The operculum creates a deep, stagnant pocket between the tooth surface and the overlying gum
- Food debris, saliva, and oral bacteria (predominantly gram-negative anaerobes - Fusobacterium, spirochetes, Prevotella) accumulate in this pocket and cannot be cleaned
- Bacteria trigger a polymicrobial inflammatory cascade - the immune system releases IL-1β, TNF-α, IL-6, and prostaglandins into the tissue
- The resulting tissue edema and purulent exudate increase hydrostatic pressure within the closed space of the operculum, compressing local nerve fibers - a major source of the throbbing, pressure-type pain
- Trauma from mastication worsens this: the upper molar occludes directly against the swollen operculum during biting, mechanically re-injuring the inflamed tissue with every chew
The pain of pericoronitis is typically described as throbbing, severe, worsened by chewing, and may radiate to the ear, jaw, or temple (referred pain via the auriculotemporal nerve - a branch of V3).
- Rosen's Emergency Medicine, p. 860
- Tintinalli's Emergency Medicine, p. 1622-1623
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 702
4. Trigeminal Nerve Sensitization and Referred Pain
The trigeminal nerve (V3 - inferior alveolar and lingual branches) provides sensory innervation to the third molar region. With sustained inflammatory input, central sensitization of the trigeminal nucleus occurs - lowering pain thresholds so that even light stimuli (touch, temperature change, jaw opening) become painful. This explains:
- Trismus (jaw spasm/limitation of mouth opening) - reflex muscle guarding mediated by the masseteric and pterygoid branches
- Earache - referred pain via the auriculotemporal nerve
- Sore throat / odynophagia - if infection spreads to the pterygomandibular or parapharyngeal spaces
5. Spreading Infection (Severe Cases)
If pericoronitis is untreated, the infection can spread into the adjacent deep fascial spaces (masseteric, pterygomandibular, parapharyngeal). This causes cellulitis and abscess formation, driving more intense, constant pain through:
- Tissue destruction and rising inflammatory cytokines
- Nerve compression from expanding soft tissue swelling
- In extreme cases, Ludwig's angina (floor-of-mouth cellulitis) - a life-threatening emergency
Summary Table
| Mechanism | Pain Type | Key Mediators |
|---|---|---|
| Pressure on PDL/bone during eruption | Deep, dull ache | Mechanoreceptor activation |
| Gingival tearing/stretching | Sharp, acute | Bradykinin, PGE2, histamine, substance P |
| Pericoronitis (operculum infection) | Throbbing, severe | IL-1β, TNF-α, PGE2, bacterial toxins |
| Masticatory trauma to operculum | Pain on biting | Mechanical nociceptor activation |
| Central sensitization (V3) | Referred, diffuse | Trigeminal nucleus sensitization |
| Deep space infection | Constant, severe | Pus/edema pressure, cytokines |
Why NSAIDs Work So Well
NSAIDs (ibuprofen 400-600 mg) are the first-line analgesic because they inhibit COX-1 and COX-2, blocking prostaglandin synthesis at the tissue level. This directly counters peripheral sensitization, reducing both pain and swelling. They are often more effective than opioids alone for this type of inflammatory pain.
- Rosen's Emergency Medicine, p. 861
- Tintinalli's Emergency Medicine, p. 1623
Can i take mefthal forte for the above?
Finding Sources
Searching the Web
Mefthal Forte mefenamic acid dicyclomine composition uses dental pain
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Meftal Forte composition mefenamic acid 500mg dicyclomine 10mg uses side effects
Reading Web Page
https://pharmeasy.in/online-medicine-order/meftal-forte-tabl…
Now I have a complete picture. Here is a thorough answer:
Can You Take Meftal Forte for Wisdom Tooth Pain?
Short answer: Yes, Meftal Forte is appropriate and will help - but with important caveats.
What Is Meftal Forte?
First, an important clarification - Meftal Forte and Meftal Spas are two different drugs that are commonly confused:
| Drug | Composition |
|---|---|
| Meftal Forte | Mefenamic Acid 500 mg + Paracetamol 325 mg |
| Meftal Spas | Mefenamic Acid 250 mg + Dicyclomine 10 mg |
Meftal Forte is a dual-analgesic combination. Meftal Spas is an antispasmodic combination primarily for abdominal/uterine cramps.
How Does Meftal Forte Work for Tooth Pain?
1. Mefenamic Acid 500 mg (NSAID - Fenamate class)
- Inhibits both COX-1 and COX-2 enzymes, blocking prostaglandin synthesis
- Prostaglandins (especially PGE2) are the major sensitizers of nociceptors in inflamed gingival tissue and the operculum in pericoronitis
- Directly counters the core mechanism of wisdom tooth pain
- Has both analgesic and anti-inflammatory effects - reduces both pain and swelling
- This is the same mechanism as ibuprofen (the textbook first-line NSAID for pericoronitis pain), just a different NSAID class
2. Paracetamol 325 mg (Acetaminophen)
- Provides central analgesic effect (inhibits prostaglandin synthesis in the CNS, possibly via COX-3)
- Works synergistically with the NSAID - together they provide better pain relief than either alone (the combination covers both peripheral and central pain pathways)
This dual mechanism makes Meftal Forte well-suited for wisdom tooth pain, which involves both peripheral tissue inflammation and central sensitization of the trigeminal nerve.
Important Caveats
1. Meftal Forte works - but Meftal Spas does NOT
If someone suggested Meftal Spas, decline it. Dicyclomine (the antispasmodic in Meftal Spas) relaxes smooth muscle and is used for gut/uterine cramps. It has no anti-inflammatory or analgesic action relevant to dental pain - as confirmed by dental practitioners. Meftal Forte is the right choice.
2. Take it with food
Mefenamic acid can cause GI irritation (nausea, diarrhea, heartburn). Always take Meftal Forte after a meal or with a full glass of water.
3. Dosage
Typical adult dose: 1 tablet (Mefenamic 500 mg + Paracetamol 325 mg) every 8 hours (three times a day), for no more than 5-7 days continuously. Do not exceed the recommended dose.
4. Contraindications - do NOT take if you have:
- Peptic ulcer or history of GI bleeding
- Asthma (NSAIDs can trigger bronchospasm in aspirin-sensitive asthmatics)
- Kidney or liver disease
- Currently pregnant (especially avoid in the third trimester - NSAIDs can cause premature closure of ductus arteriosus)
- Already taking blood thinners (warfarin, aspirin) or other NSAIDs
5. It treats the symptom, not the cause
Meftal Forte will reduce pain and inflammation, but it will NOT resolve the underlying pericoronitis. If the pain is from an infected or impacted wisdom tooth, you still need to see a dentist for:
- Irrigation and cleaning under the operculum
- Antibiotics if there is spreading infection (penicillin or metronidazole are standard)
- Possible extraction of the impacted tooth
Bottom Line
Yes, Meftal Forte is a reasonable OTC choice for short-term relief of wisdom tooth pain. The mefenamic acid directly blocks the inflammatory prostaglandin cascade driving the pain. Take it after food, limit use to a few days, and see a dentist - pain relief is not a substitute for treating the underlying cause.
- Rosen's Emergency Medicine (ibuprofen/NSAIDs as first-line for pericoronitis pain, p. 861)
- Tintinalli's Emergency Medicine (NSAIDs and opiates for pericoronitis analgesia, p. 1623)
What all will be the symptoms of wisdom tooth eruption pain
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is the complete, textbook-grounded answer on symptoms of wisdom tooth eruption pain:
Symptoms of Wisdom Tooth Eruption Pain
Symptoms range from mild local discomfort during simple eruption to severe systemic signs when pericoronitis or deep infection develops.
Local Symptoms (At the Tooth Site)
| Symptom | Description |
|---|---|
| Pain at the back of the mouth | Throbbing or dull ache at the lower/upper back jaw; typically the first and most prominent symptom |
| Swollen, red gum (operculum) | The gum flap overlying the erupting tooth becomes erythematous, edematous, and tender to touch |
| Pain worsened by biting/chewing | The upper tooth occludes directly against the inflamed operculum, re-injuring it with every bite |
| Bleeding gum | The inflamed operculum bleeds easily on contact or when probed |
| Pus or discharge | In pericoronitis, a purulent discharge may ooze from under the gum flap |
| Bad taste in the mouth | From purulent discharge and bacterial overgrowth in the stagnant pocket under the operculum |
- Rosen's Emergency Medicine, p. 860
Referred and Radiating Symptoms
| Symptom | Cause |
|---|---|
| Earache (otalgia) | Referred pain via the auriculotemporal nerve (branch of V3); the ear feels painful even though the problem is the tooth |
| Jaw or temple pain | Spread of pain along the inferior alveolar and masseteric branches of V3 |
| Sore throat / pain on swallowing | If infection tracks toward the pterygomandibular or parapharyngeal space |
Functional Symptoms
| Symptom | Cause |
|---|---|
| Trismus (difficulty opening the mouth) | Reflex muscle spasm of the masseter and medial pterygoid muscles; occurs when inflammation is near these muscles; a key sign of pericoronitis - Scott-Brown's Otorhinolaryngology, p. 702 |
| Difficulty chewing | Combination of trismus, pain on biting, and gum swelling |
| Difficulty swallowing (odynophagia) | If infection spreads to peritonsillar or parapharyngeal spaces |
Systemic Symptoms (in More Severe Cases)
| Symptom | Significance |
|---|---|
| Fever and malaise | Indicates spreading infection beyond the local gum tissue; warrants antibiotics |
| Facial swelling | Localized soft tissue edema over the jaw/cheek from the spreading inflammatory process |
| Regional lymphadenopathy | Swollen, tender lymph nodes under the jaw (submandibular) and neck - a clinical sign of infection, not simple eruption - Scott-Brown's, p. 702 |
| Headache | From systemic inflammation and central sensitization of the trigeminal nucleus |
Red Flag Symptoms (Seek Urgent Care)
These indicate the infection is spreading beyond the tooth and can become life-threatening:
- Progressive trismus - worsening inability to open the mouth
- High fever (>38.5°C) with chills
- Neck swelling or stiffness
- Difficulty swallowing or breathing
- Floor of mouth swelling - this suggests Ludwig's angina (bilateral cellulitis of the floor of the mouth), an airway emergency that can originate from third molar infections - Cummings Otolaryngology, p. 1953
If any of these are present, go to an emergency department immediately - not just a dentist.
How Symptoms Tend to Progress
Simple eruption Pericoronitis Spreading infection
───────────────── → ───────────────────── → ─────────────────────────
Mild ache Throbbing pain Severe pain + fever
Gum tenderness Swollen operculum Trismus + facial swelling
Bad taste + pus Lymphadenopathy
Pain on biting Dysphagia
Referred earache [Ludwig's angina risk]
The pain from wisdom teeth often comes and goes - the operculum repeatedly gets infected, partially resolves, then flares again. This relapsing-remitting pattern is characteristic, and each episode can escalate if the underlying tooth is not addressed.
- Tintinalli's Emergency Medicine, p. 1622-1623
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 702
- Rosen's Emergency Medicine, p. 860-861
This is a shared conversation. Sign in to Orris to start your own chat.