Coronary circulation for 8 marks make notes and flow chart
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the content needed to write comprehensive 8-mark notes with a flowchart. Let me compose the answer.
Coronary Circulation - 8 Mark Notes
(Sources: Guyton & Hall Medical Physiology, Costanzo Physiology, Ganong's Review of Medical Physiology)
1. DEFINITION
Coronary circulation is the system of blood vessels that supplies oxygenated blood to the myocardium and drains deoxygenated blood back to the right atrium. It is the most important regional circulation because cardiac muscle has virtually no O2 reserve and depends entirely on continuous blood delivery.
2. ANATOMICAL CONSIDERATIONS
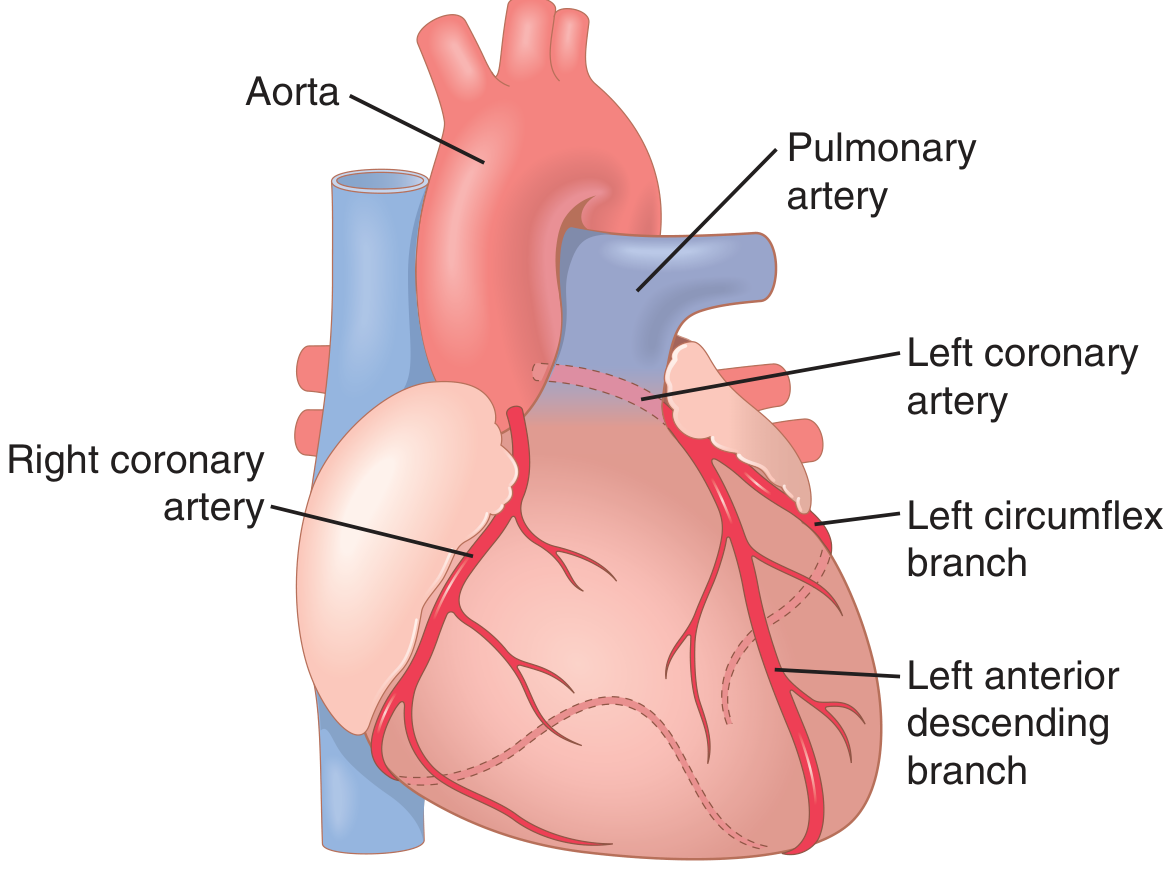
Arterial Supply
The two coronary arteries arise from sinuses (sinuses of Valsalva) behind the cusps of the aortic valve at the root of the aorta.
LEFT CORONARY ARTERY (LCA)
- Supplies: anterior + left lateral walls of the left ventricle (LV), most of the interventricular septum
- Divides into:
- Left Anterior Descending (LAD) - most important clinically; supplies anterior LV + septum
- Left Circumflex (LCx) - supplies posterior and lateral LV wall
RIGHT CORONARY ARTERY (RCA)
- Supplies: right ventricle (RV), posterior LV (in 80-90% of people), SA node (~60%), AV node (~85%)
- Main branches: marginal branch, posterior descending artery (PDA)
The myocardium is supplied through epicardial arteries on the surface → intramuscular arteries that penetrate inward → subendocardial arterial plexus (most vulnerable to ischemia).
Venous Drainage
| Route | What it drains | Drains into |
|---|---|---|
| Coronary sinus | ~75% of LV venous blood | Right atrium |
| Anterior cardiac veins | Most of RV | Right atrium (directly) |
| Thebesian veins | Small amount | All cardiac chambers directly |
| Arteriosinusoidal vessels | Connect arterioles → chambers | Cardiac chambers |
3. CORONARY BLOOD FLOW - NORMAL VALUES
| Parameter | Value |
|---|---|
| Resting flow | ~70 mL/min/100 g OR ~225 mL/min total |
| % of cardiac output | 4-5% |
| O2 extraction at rest | ~70% (very high - almost maximal) |
| During exercise | Increases 3-4 fold |
- Because O2 extraction is already near maximal at rest, increased demand must be met by increased blood flow (not increased extraction).
4. PHASIC FLOW - SYSTOLE vs DIASTOLE
This is the unique feature of coronary circulation:
Left Ventricle:
- During systole - intramyocardial pressure exceeds aortic pressure (LV pressure ~121 mmHg vs Aorta ~120 mmHg), compressing intramuscular vessels → blood flow falls to nearly zero
- During diastole - muscle relaxes, vessels open → blood flow is maximal
- Therefore, LV is perfused mainly during diastole
- ⚠ Tachycardia shortens diastole → reduces LV perfusion time → risk of ischemia
Right Ventricle:
- RV contraction force is much lower; pressure differential (Aorta 120 vs RV 25 mmHg) remains positive during systole
- Blood flow occurs throughout the cardiac cycle (not markedly reduced in systole)
Subendocardial region (innermost layer of LV wall) is most vulnerable because it faces the highest intramural compression during systole → most common site of myocardial infarction.
| Region | Perfusion Timing |
|---|---|
| LV epicardium | Both systole + diastole |
| LV subendocardium | Diastole ONLY |
| RV myocardium | Both systole + diastole |
5. REGULATION OF CORONARY BLOOD FLOW
A. Local Metabolic Control (PRIMARY - most important)
Blood flow is regulated mainly by local vasodilator metabolites matching O2 supply to demand:
| Metabolite | Trigger | Effect |
|---|---|---|
| Adenosine (most important) | ATP → AMP → Adenosine when O2 falls | Coronary arteriolar dilation |
| Hypoxia / ↓ PO2 | Increased cardiac work | Direct vasodilation |
| ↑ CO2 / ↑ H+ | Increased metabolism | Vasodilation |
| K+ ions | Action potentials, metabolic activity | Vasodilation |
| Nitric oxide (NO) | Shear stress, metabolites | Vasodilation |
| Prostaglandins | Metabolic demand | Vasodilation |
Mechanism of adenosine: O2 demand↑ → ATP degraded → AMP → adenosine released → diffuses to coronary arterioles → vasodilation → ↑ blood flow → ↑ O2 delivery (active hyperemia)
B. Autoregulation
Coronary blood flow is autoregulated over a perfusion pressure range of 60-120 mmHg. If pressure drops below this, blood flow falls proportionally and ischemia results.
C. Reactive Hyperemia
During systolic compression (brief occlusion), an O2 debt accumulates. When occlusion ends at diastole, flow surges above baseline to repay the O2 debt. This is reactive hyperemia.
D. Nervous Control (secondary - indirect > direct)
| Stimulus | Direct Effect | Indirect Effect (via heart rate/contractility) | Net Result |
|---|---|---|---|
| Sympathetic (norepinephrine) | α1: vasoconstriction | ↑ HR + contractility → ↑ O2 demand → metabolic vasodilation | Net: vasodilation (metabolic overrides) |
| Sympathetic (epinephrine) | β2: vasodilation | ↑ HR + contractility → ↑ O2 demand | Net: vasodilation |
| Parasympathetic (ACh/vagal) | Direct: mild vasodilation | ↓ HR + contractility → ↓ O2 demand → vasoconstriction | Net: reduced flow |
6. CLINICAL SIGNIFICANCE
- Myocardial Infarction: most common in subendocardial region of LV (LAD territory most often)
- Tachycardia: reduces diastolic filling time → reduces LV coronary flow → angina risk
- Aortic stenosis: LV must generate far higher pressure than aorta → subendocardial ischemia
- Coronary artery disease (CAD): ~1/3 of all deaths in industrialized nations (Guyton)
- Angina pectoris: chest pain when O2 demand exceeds supply
7. FLOWCHART: REGULATION OF CORONARY BLOOD FLOW
INCREASED CARDIAC WORKLOAD
(e.g., exercise, tachycardia, increased contractility)
│
▼
↑ O2 Consumption by Myocardium
│
▼
Local Hypoxia / ↓ PO2
ATP → AMP → ADENOSINE (+ CO2, H+, K+, NO)
│
▼
Coronary Arteriolar VASODILATION
(Active Hyperemia)
│
▼
↑ Coronary Blood Flow (up to 3-4x at peak exercise)
│
▼
↑ O2 Delivery to Myocardium
│
▼
O2 demand is met → Adenosine recycled back to ATP
(Negative feedback loop restored)
PHASIC CORONARY FLOW (Cardiac Cycle)
SYSTOLE DIASTOLE
│ │
LV intramural pressure HIGH LV muscle relaxes
(~121 mmHg) compresses vessels Vessels open fully
│ │
▼ ▼
LV flow ↓ (near zero) LV flow ↑ (maximal)
RV flow not much reduced (subendocardial repaid)
│ │
└──────────────────┬─────────────┘
▼
If systole prolonged / diastole shortened
(e.g., tachycardia, aortic stenosis)
│
▼
Subendocardial ISCHEMIA → MI risk
8. SUMMARY TABLE (Quick Revision)
| Feature | Detail |
|---|---|
| Origin of coronary arteries | Aortic sinuses (sinuses of Valsalva) |
| LCA supplies | Anterior LV, septum (via LAD + LCx) |
| RCA supplies | RV, posterior LV (in 80-90%), SA + AV nodes |
| Resting coronary flow | 225 mL/min (~5% of cardiac output) |
| O2 extraction | ~70% at rest (near maximal) |
| LV perfusion timing | Mainly diastole |
| RV perfusion timing | Both systole and diastole |
| Primary regulator | Local metabolites (adenosine, hypoxia) |
| Key vasodilator substance | Adenosine |
| Most ischemia-prone region | Subendocardium of LV |
| Venous drainage | Coronary sinus (75%) + anterior cardiac veins + Thebesian veins |
Sources:
- Guyton & Hall Medical Physiology - Chapter 21 (Coronary Circulation)
- Costanzo Physiology 7th Edition - Special Circulations
- Ganong's Review of Medical Physiology 26th Edition - Chapter 33
This is a shared conversation. Sign in to Orris to start your own chat.