Explain me 10 common heart disease with ECG changes , & ECG image
Reading File
Finding Sources
Searching Images
ECG changes myocardial infarction STEMI
Finding Sources
Searching Images
ECG atrial fibrillation heart block ventricular tachycardia
Searching Images
ECG left ventricular hypertrophy heart failure pericarditis
Searching Images
ECG Wolff-Parkinson-White syndrome delta wave pre-excitation
Searching Images
ECG pulmonary embolism right heart strain S1Q3T3
Searching Images
ECG ventricular tachycardia hypertrophic cardiomyopathy long QT syndrome
I now have excellent ECG images for all 10 conditions. Let me compile the comprehensive answer.
10 Common Heart Diseases — ECG Changes & Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery (most commonly LAD, RCA, or LCx) causing transmural myocardial injury.
ECG Changes:
- Hyperacute T-waves (earliest sign — tall, peaked, asymmetric)
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in precordial leads
- Convex ("tombstone") ST morphology in severe cases
- Reciprocal ST depression in opposing leads
- Pathological Q-waves developing within hours (irreversible necrosis)
- T-wave inversion in the evolutionary phase
Localisation:
| Territory | Leads with ST Elevation | Culprit Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA / LCx |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V3 + tall R | RCA / LCx |
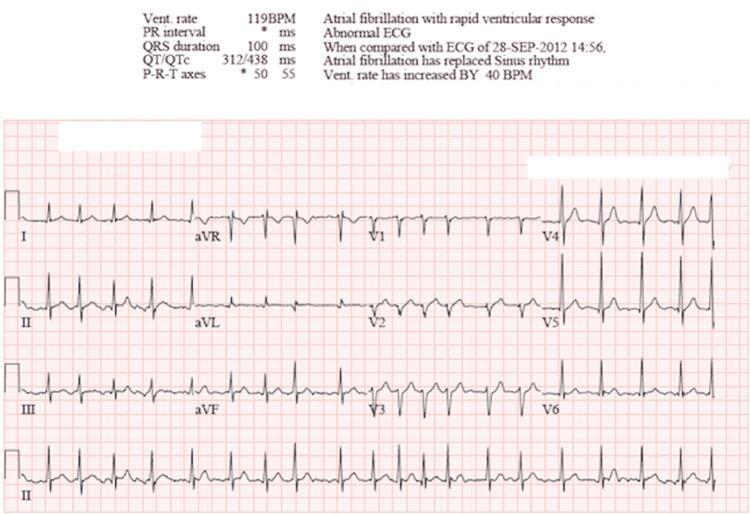
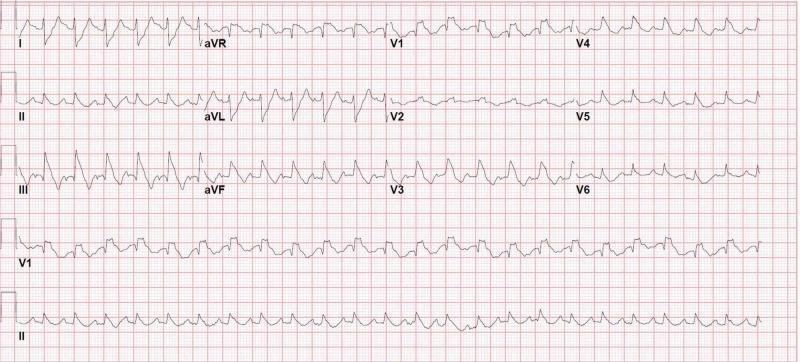
2. Atrial Fibrillation (AF)
Pathophysiology: Disorganized chaotic atrial electrical activity from multiple reentrant wavelets, causing irregular ventricular response.
ECG Changes:
- Absent P-waves — replaced by irregular fibrillatory baseline (best seen in V1)
- Irregularly irregular RR intervals (hallmark sign)
- Narrow QRS complexes (unless aberrant conduction or bundle branch block)
- Ventricular rate variable — controlled (<100 bpm) or uncontrolled (>100 bpm = rapid ventricular response, RVR)
- No discrete PR interval
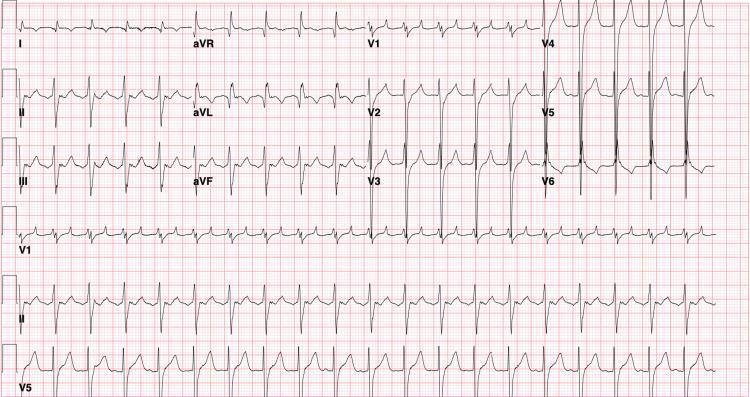
3. Atrial Flutter
Pathophysiology: Single reentrant circuit in the right atrium (cavotricuspid isthmus), producing regular rapid atrial depolarization.
ECG Changes:
- Sawtooth flutter waves (F-waves) at ~300 bpm — best seen in II, III, aVF and V1
- Regular atrial rate ~300 bpm with AV block in fixed ratios
- 2:1 block → ventricular rate ~150 bpm (most common)
- 4:1 block → ventricular rate ~75 bpm
- Narrow QRS complexes (unless aberrant conduction)
- No isoelectric baseline between flutter waves
4. Complete (Third-Degree) AV Block
Pathophysiology: Complete dissociation between atrial and ventricular conduction — no impulses pass through the AV node. Escape rhythm from junctional or ventricular pacemaker takes over.
ECG Changes:
- Complete P-wave and QRS dissociation — P-waves and QRS complexes are totally independent
- Regular P-waves at normal atrial rate (60–100 bpm)
- Slow escape rhythm — junctional escape (40–60 bpm, narrow QRS) or ventricular escape (<40 bpm, wide QRS)
- No relationship between PR intervals (vary randomly)
- Bradycardia with haemodynamic compromise
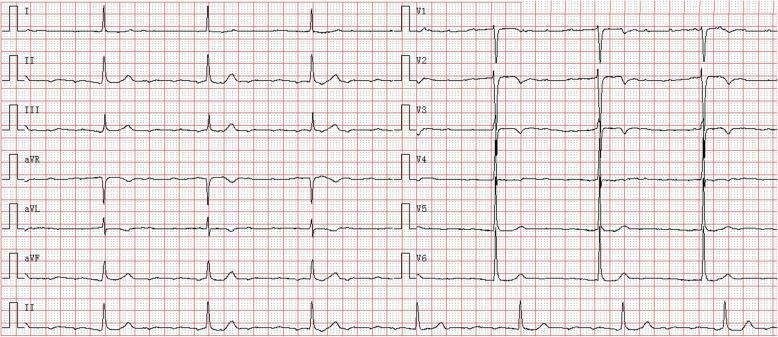
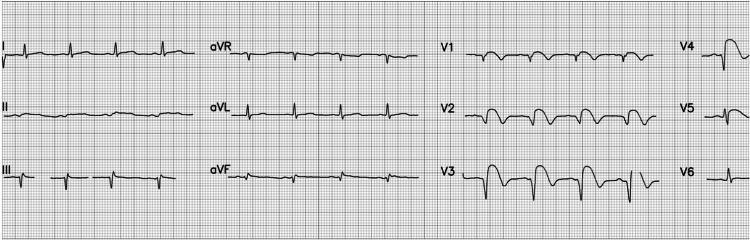
5. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased myocardial mass from chronic pressure overload (hypertension, aortic stenosis) or volume overload, increasing the electrical forces of the left ventricle.
ECG Changes:
- High-voltage QRS — Sokolow-Lyon: S in V1 + R in V5/V6 ≥35 mm
- Cornell criterion: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- Left axis deviation
- ST depression and T-wave inversion in lateral leads (V5–V6, I, aVL) = "strain pattern"
- Left atrial enlargement — broad, notched P-wave in II ("P mitrale"), biphasic P in V1
- Increased QRS duration (may approach 100 ms)
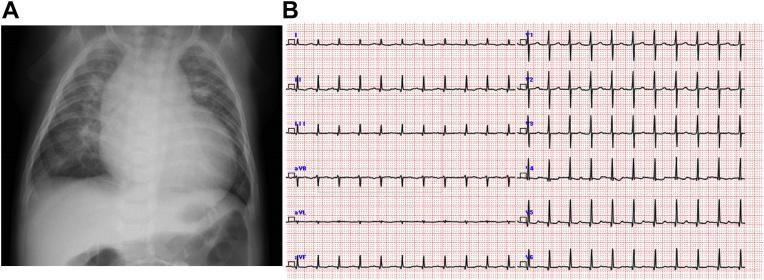
6. Pulmonary Embolism (PE) — Right Heart Strain
Pathophysiology: Acute obstruction of pulmonary vasculature increases right ventricular afterload → acute RV dilation and strain → electrical axis shifts rightward.
ECG Changes:
- Sinus tachycardia (most common and sensitive finding)
- S1Q3T3 pattern — deep S wave in lead I, Q wave in lead III, T-wave inversion in lead III
- Incomplete or complete RBBB (acute right ventricular stress)
- T-wave inversions in V1–V4 (right precordial leads)
- Rightward axis shift
- P pulmonale — tall peaked P in II (right atrial strain)
- ST changes may mimic inferior MI


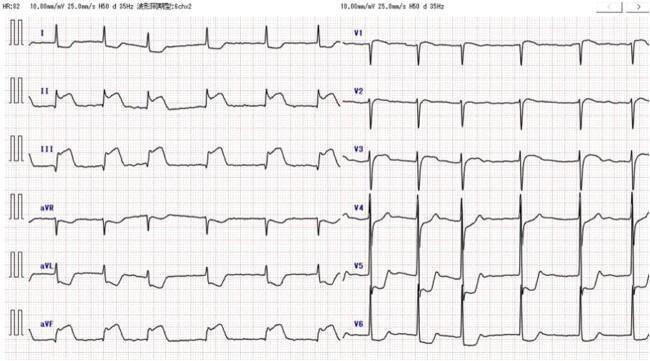
7. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: Accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Risk of rapid conduction via the accessory pathway during AF → ventricular fibrillation.
ECG Changes (classic triad):
- Shortened PR interval (<120 ms) — bypasses AV nodal delay
- Delta wave — slurred upstroke at the beginning of the QRS (initial pre-excitation)
- Widened QRS complex (>120 ms) — fusion of pre-excited and normally conducted beats
- Secondary ST-T changes — opposite to main QRS deflection
- Pseudo-infarct Q-waves in inferior leads (posteroseptal pathway)
- Delta wave polarity localises the pathway

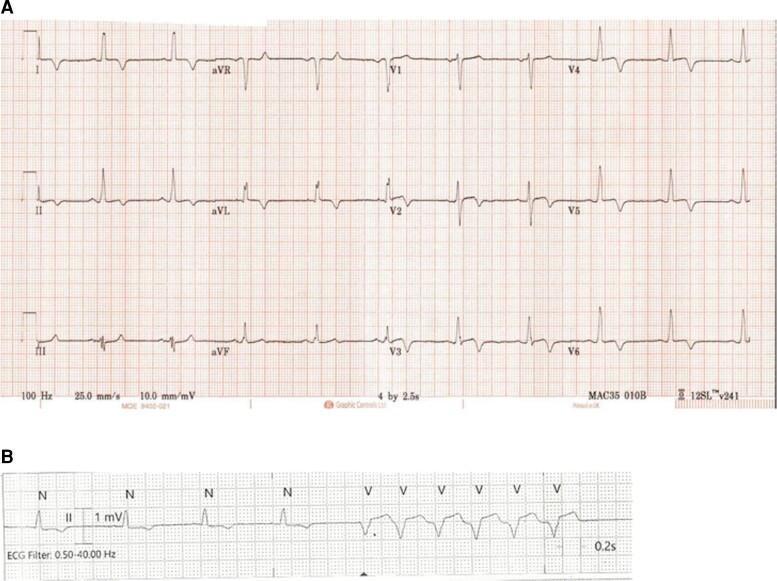
8. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Asymmetric septal hypertrophy (sarcomeric gene mutation) causes dynamic LVOT obstruction, diastolic dysfunction, and risk of sudden cardiac death from ventricular arrhythmias.
ECG Changes:
- LVH voltage criteria (Sokolow-Lyon met in ~75%)
- Deep, narrow Q-waves (septal depolarisation abnormality) in lateral/inferior leads — key feature
- "Giant" T-wave inversions in precordial leads V4–V6 — pathognomonic of apical HCM (Yamaguchi syndrome)
- Left axis deviation
- ST depression in lateral leads
- Short PR interval (in some)
- Non-sustained VT on Holter monitoring
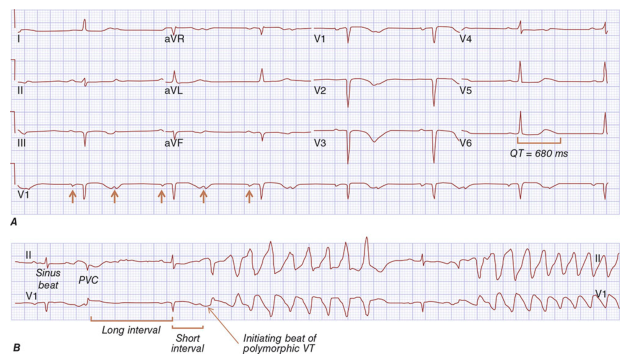
9. Long QT Syndrome (LQTS)
Pathophysiology: Delayed ventricular repolarisation from ion channel mutations (congenital) or drugs/electrolytes (acquired). Predisposes to Torsades de Pointes (TdP) → ventricular fibrillation → sudden death.
ECG Changes:
- Prolonged QTc interval — Bazett's formula: QT/√RR
- QTc ≥450 ms (men) or ≥460 ms (women) = abnormal
- QTc ≥500 ms = high risk for TdP
- Abnormal T-wave morphology — notched T-waves (LQT2), broad-based T-waves (LQT1), late-onset T-waves (LQT3)
- U-waves — prominent in LQT2 (lead V1)
- T-wave alternans — beat-to-beat variation in T-wave amplitude/polarity (severe form)
- Torsades de Pointes — polymorphic VT with characteristic "twisting" QRS morphology around isoelectric line, initiated by short-long-short RR sequence
10. Right Bundle Branch Block (RBBB)
Pathophysiology: Delayed conduction through the right bundle branch causes sequential ventricular activation — left ventricle activates first (normally), followed by delayed right ventricular activation.
ECG Changes:
- QRS duration ≥120 ms (complete RBBB)
- RSR' (or "M-shaped") pattern in V1–V2 — initial R (septal), S (LV activation), and terminal R' (delayed RV activation)
- Wide, slurred S-waves in I, aVL, V5–V6 (terminal conduction delay leftward to right)
- Secondary ST depression and T-wave inversion in V1–V2
- No change in Q-wave pathology or axis (unless associated with hemiblock)
- Clinical associations: acute PE, ASD, Brugada syndrome unmasking, ischaemia
Quick Reference Summary
| # | Condition | Key ECG Sign |
|---|---|---|
| 1 | STEMI | ST elevation in contiguous leads + reciprocal changes |
| 2 | Atrial Fibrillation | Irregularly irregular, no P-waves |
| 3 | Atrial Flutter | Sawtooth F-waves ~300 bpm, 2:1 block |
| 4 | Complete AV Block | P-QRS dissociation, escape rhythm |
| 5 | LVH | High voltage + lateral strain pattern |
| 6 | Pulmonary Embolism | S1Q3T3 + sinus tachycardia + RBBB |
| 7 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 8 | HCM | LVH + deep Q-waves + giant T inversions (apical) |
| 9 | Long QT Syndrome | QTc ≥500 ms + T-wave alternans → TdP |
| 10 | RBBB | RSR' in V1, wide S in I/aVL/V5–V6 |
Clinical note: ECG changes must always be interpreted in clinical context. A single ECG pattern can be caused by multiple conditions, and some serious conditions (e.g., posterior MI, early PE) may have subtle or atypical findings. Serial ECGs and correlation with symptoms, biomarkers, and imaging remain essential.
This is a shared conversation. Sign in to Orris to start your own chat.