You are posted as the District Program Officer under the National Health Mission. During your field visits and record review, you notice that the district's MMR has remained unchanged over the last three years, despite adequate infrastructure and skilled staff . Using the health planning cycle outline the step by step approach you would adopt to:
Reading File
Finding Sources
Finding Sources
Searching the Web
health planning cycle steps MMR maternal mortality reduction district NHM India
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything I need. Note that the user's question appears to have been cut off (ends with "to:"), but the core intent is clear: apply the health planning cycle to investigate stagnant MMR and develop an action plan. I'll address the full scenario comprehensively.
Note: Your question appears to have been cut off after "to:" - the specific sub-tasks you wanted addressed weren't captured. I've interpreted the full intent as: (a) investigate why MMR is stagnant despite adequate infrastructure and staff, and (b) develop a corrective action plan - both using the health planning cycle. If you had specific sub-questions in mind, please share them and I'll tailor the response.
Applying the Health Planning Cycle to Stagnant MMR: A District DPO Approach
The core framework comes from Park's textbook definition: health planning is "the orderly process of defining community health problems, identifying unmet needs and surveying the resources to meet them, establishing priority goals that are realistic and feasible and projecting administrative action to accomplish the purpose of the proposed programme."
The planning cycle below is the structured tool for doing exactly this.
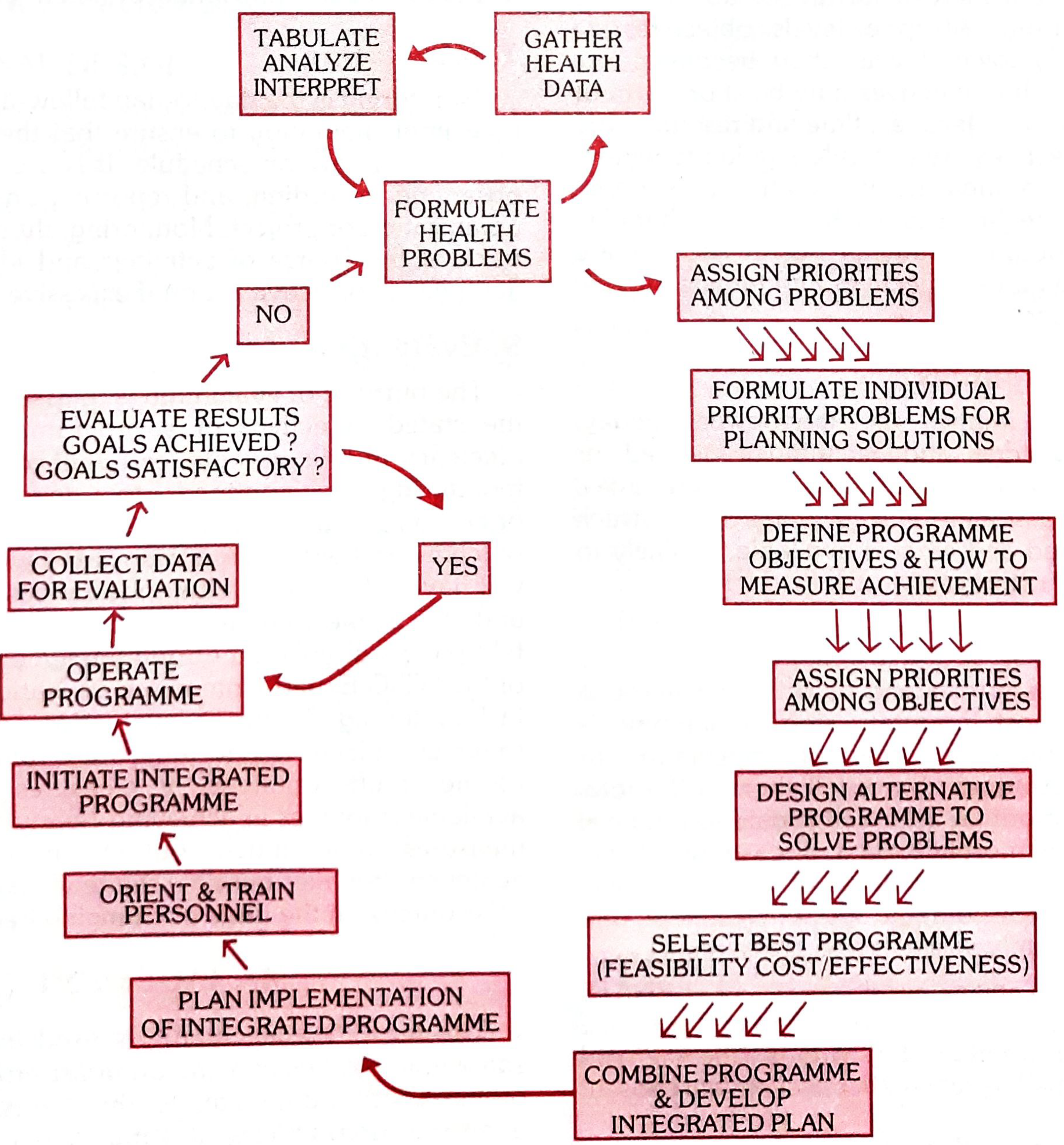
STEP 1: Analysis of the Health Situation
What to do: Gather, tabulate, analyze, and interpret all available health data for the district - this is the foundation.
In this scenario - specific data to collect:
| Data Source | What to Extract |
|---|---|
| HMIS/DHIS-2 | Cause-of-death breakdown in maternal deaths (PPH, sepsis, eclampsia, unsafe abortion, obstructed labour) |
| Maternal Death Review (MDR) registers | Avoidable factors - patient delays, provider delays, system delays (3-delays model) |
| Facility delivery records | Proportion of home vs institutional deliveries; night-time deliveries; referral patterns |
| ANC registers | 4 ANC coverage, high-risk identification and follow-up rates |
| Labour room registers | Active management of 3rd stage (AMTSL) compliance, blood transfusion availability |
| Staff attendance and duty rosters | Whether skilled birth attendance is actually present 24x7 |
| Drug/supply chain records | Oxytocin, MgSO4, antihypertensives, blood - availability vs stockouts |
Key investigative lens: "Adequate infrastructure and skilled staff" does not mean functioning infrastructure and deployed skilled staff. Disaggregate the data by facility, by time (night vs day), by cause of death, and by sub-block/geography. MMR stagnating despite inputs almost always means a process or quality gap, not a capacity gap.
STEP 2: Formulation of the Health Problem
What to do: Based on Step 1 data, precisely define the problem using epidemiological evidence.
Formulate it as:
- "Despite 3 years of maintained health infrastructure and staffing norms, the district MMR remains at [X/100,000 live births], with [Y%] of deaths occurring in institutions, predominantly due to [top 1-2 causes], with [Z%] classified as avoidable by MDR committees."
Likely findings that explain stagnant MMR:
- Delays in receiving care at facility (Delay Type 3) - staff present but not responsive; signal functions not being performed (e.g., no blood transfusion, no C-section at FRU)
- Weak high-risk pregnancy identification and referral during ANC
- Poor quality of maternal death reviews - deaths recorded but root causes not actioned
- Social/geographic barriers - tribal, remote, or migrant populations not accessing care (Delay Type 1 and 2)
- Data quality issues - deaths missed or miscoded, giving a false picture of "no improvement"
STEP 3: Assign Priorities Among Problems
What to do: Not all identified gaps can be tackled simultaneously. Use criteria to prioritize:
- Magnitude (how many deaths does this cause account for?)
- Severity (case fatality of the cause)
- Feasibility of intervention (can it be fixed with existing resources?)
- Community and political concern
In practice: If PPH accounts for 40% of maternal deaths and oxytocin is sporadically available or AMTSL is not being practiced, that is Priority 1. If eclampsia deaths are occurring without MgSO4 being given, that is Priority 2. Prioritize by the leading preventable cause identified in the MDR data.
STEP 4: Formulate Objectives and How to Measure Achievement
What to do: Convert priorities into SMART objectives with clear indicators.
Example objectives:
- "Reduce MMR from [current] to [target] per 100,000 live births by [date]."
- "Achieve 100% AMTSL practice at all institutional deliveries within 6 months."
- "Ensure MgSO4 availability at all 24x7 PHCs within 3 months."
- "Conduct MDR for 100% of maternal deaths within 6 weeks of occurrence."
- "Increase proportion of high-risk pregnancies receiving 3rd trimester facility-based follow-up from [X]% to 90% within 1 year."
Indicators must be measurable from existing HMIS, with a clear numerator, denominator, and data source.
STEP 5: Design Alternative Programmes and Select the Best
What to do: Examine multiple intervention strategies for each priority; select on the basis of feasibility, cost-effectiveness, and contextual fit.
For the scenario of stagnant MMR despite adequate resources:
| Approach | Feasibility | Likely Impact |
|---|---|---|
| Strengthen Maternal Death Surveillance and Response (MDSR) - action-oriented MDR | High - existing system, needs activation | High - directly links deaths to corrective action |
| Monthly facility-level quality checks using LaQshya/MNH toolkit | High - NHM framework exists | High for process improvement |
| On-site mentoring and clinical skills refresher for SBAs (not just training) | Medium - requires master trainers | High for skill-practice gaps |
| Community-level ASHA sensitization for danger signs and early referral | High - ASHA network available | Moderate (addresses Delay 1 and 2) |
| PPP for blood banking or telemedicine obstetric consultation | Medium - requires state approval | Useful for remote FRUs |
| Social mapping of unreached women (migrant, tribal, marginalized) | Medium effort, high equity impact | Addresses hidden burden |
Select the best programme by combining approaches - MDSR strengthening + quality improvement cycles + community mobilization typically gives the highest yield for resource-constrained settings.
STEP 6: Write Up the Formulated Plan (District Action Plan)
What to do: Produce a written District Health Action Plan (DHAP) with the following components, aligned to NHM norms:
- Situation analysis summary
- Problem statement with evidence
- Objectives and targets (time-bound)
- Activity schedule (who does what, by when)
- Resources required (human, financial, logistics)
- Roles and responsibilities at each level (CHC/PHC/DH/ASHA)
- Built-in monitoring indicators
This plan is presented to the District Health Society for approval and budget allocation under the NHM Programme Implementation Plan (PIP).
STEP 7: Programming and Implementation
What to do: Translate the approved plan into action - assign roles, delegate authority, and set deadlines.
Key implementation actions specific to this problem:
- Reactivate the District MDR Committee - schedule quarterly review meetings with case-by-case analysis, with a mandatory "action taken" column
- Conduct 24x7 PHC and FRU signal function audits - verify that all 9 basic EmOC and 7 comprehensive EmOC signal functions are actually being performed, not just declared available
- Supply chain lock-in - oxytocin, MgSO4, antihypertensives, IV fluids, blood (or rapid referral protocol to blood bank) made non-negotiable at each facility level
- Rota verification - confirm skilled birth attendant night duty compliance; address contractual/motivational issues for staff deployed in remote PHCs
- ASHA incentive alignment - ensure JSY/JSSK payments are not delayed, which demotivates ASHA accompaniment
- Convergence with ICDS and Panchayati Raj - for social mobilization, identifying unreached women
STEP 8: Monitoring
What to do: Establish continuous, real-time tracking of key process indicators - not just MMR (which is an outcome and lags by months).
Process indicators to monitor monthly:
- % institutional deliveries
- % high-risk pregnancies identified and followed up
- % deliveries with documented AMTSL
- % maternal deaths reviewed within 6 weeks with action plan
- Stockout days for oxytocin, MgSO4 at each facility
- % FRU C-section rate (should be 3-10% of deliveries)
- 48-hour post-natal care coverage
Tools: HMIS dashboards, monthly facility performance review meetings at DPMU, District Health Society (DHS) quarterly reviews.
STEP 9: Evaluation (Closing the Loop)
What to do: Periodically assess whether objectives are being achieved and whether the MMR is actually moving. Feed results back into the next planning cycle.
How to evaluate in this district:
- Annual review of MMR trend using SRS/HMIS data
- Process evaluation: are the targeted activities happening at planned scale and quality?
- Impact evaluation: are the intermediate outcomes (high-risk coverage, institutional delivery quality, signal function performance) improving?
- If MMR still does not improve after process indicators have improved, suspect a data quality problem - active community-based maternal death searching should be initiated (verbal autopsies, ASHA reporting, cremation/burial ground surveillance)
The key feedback question: "Are the goals achieved? Are goals satisfactory?" If NO - the cycle restarts from Step 1 with revised hypotheses.
Summary: The DPO's Diagnostic Lens
The central insight in your scenario is that stagnant MMR despite adequate inputs points to a process and quality failure, not a resource failure. The planning cycle operationalizes this by forcing a rigorous situation analysis (Step 1) before jumping to solutions. In this context, the most productive steps are:
- Step 1: Deep-dive MDR data analysis and facility audit
- Step 4: Sharp, measurable objectives (not vague "improve MMR")
- Step 7: Implementation focused on accountability - MDR-to-action linkage, signal function audit, duty compliance
- Step 8: Monitoring process indicators, not just the outcome (MMR)
This approach directly addresses what research on India's MMR drivers confirms: "More than individual-level factors, health system factors account for a greater reduction in MMR" - meaning system processes and quality are the primary levers once infrastructure is in place.
Source: Park's Textbook of Preventive and Social Medicine - Health Planning (Planning Cycle, pp. 972-976); Maternal Mortality Ratio (p. 320)
This is a shared conversation. Sign in to Orris to start your own chat.