Mri findings in hsv encephalitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"herpes simplex encephalitis"[MeSH Terms] AND "MRI" AND neuroimaging
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks and two actual MRI images. Here is the complete answer:
MRI Findings in HSV Encephalitis
MRI is the most sensitive imaging modality for detecting HSV encephalitis (HSE), identifying lesions far earlier than CT.
Characteristic Regions Involved
HSV-1 has a striking predilection for limbic structures due to its route of entry via the olfactory pathway and reactivation from the trigeminal ganglion:
| Region | Structures |
|---|---|
| Mesiotemporal lobe | Amygdala, hippocampus, uncus, parahippocampal gyrus |
| Inferofrontal lobe | Cingulate gyrus, orbital frontal cortex |
| Insular cortex | Claustrum region, lateral temporal border |
- Distribution is typically unilateral or asymmetrically bilateral
- Mesiotemporal > lateral temporal involvement - this is a key differentiator from other encephalitides
- Gray matter predominance over white matter - another distinguishing feature from autoimmune/paraneoplastic limbic encephalitis
MRI Signal Characteristics by Sequence
T2-weighted / FLAIR (most important)
- Increased (hyperintense) signal in the affected regions
- FLAIR is superior to standard T2 for detecting subtle early involvement
- Cortical swelling and gyral expansion often present
T1-weighted
- Mildly hypointense signal in affected areas
- Can show cortical/gyral pattern of involvement
Diffusion-weighted imaging (DWI)
- Restricted diffusion (bright on DWI, dark on ADC) in the medial temporal lobe and hippocampus
- Represents cytotoxic edema and early neuronal death
- DWI may be positive even before FLAIR becomes abnormal in very early cases
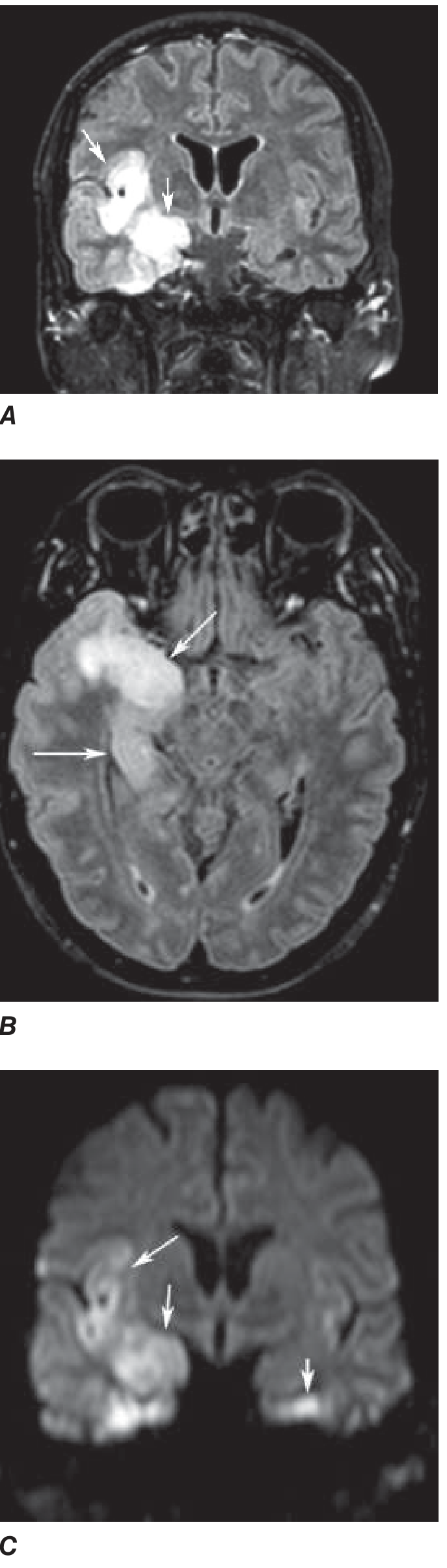
- As seen in Harrison's image (Panel C): restricted diffusion in the right medial temporal lobe/hippocampus with subtle involvement on the left side
Gadolinium contrast (T1+C)
- Early gadolinium enhancement may occur but is not universal
- Enhancement reflects blood-brain barrier breakdown
- Leptomeningeal or cortical pattern of enhancement
CT comparison
- CT is less sensitive than MRI for early/mild disease
- However, because HSE can be hemorrhagic, CT may detect hemorrhage more reliably than MRI in some cases
Actual MRI Images
Figure 1 - FLAIR MRI (Goldman-Cecil): Right mesiotemporal hyperintensity (Panel A) and bilateral interfrontal/cingulate/right insular cortex signal change (Panel B):
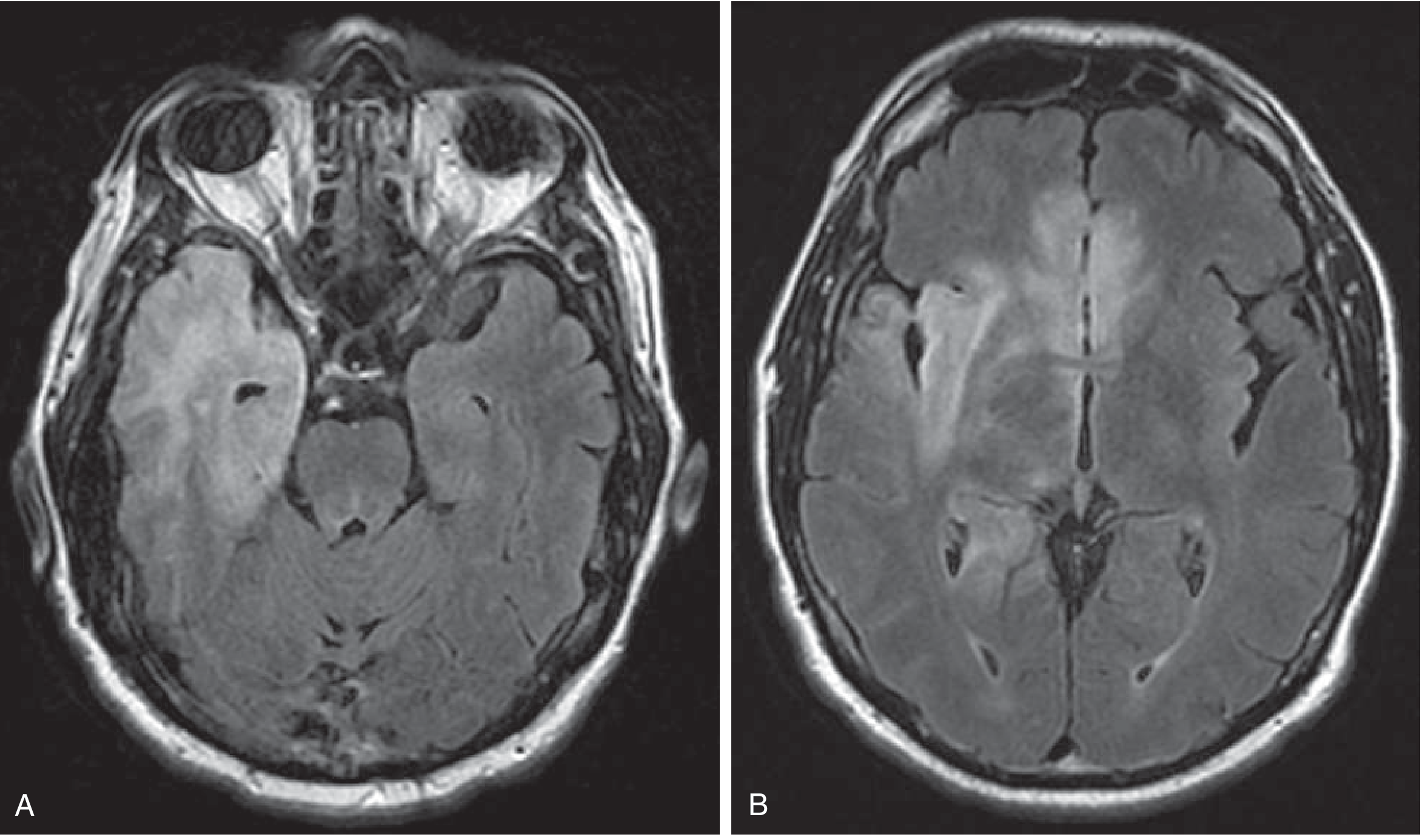
Figure 2 - Harrison's (FLAIR + DWI): Coronal FLAIR (A), axial FLAIR (B), and coronal DWI (C) showing right medial temporal/insular high signal with restricted diffusion, and subtle left temporal involvement on DWI:
Additional Features
- EEG correlation: Periodic high-voltage 1-Hz sharp waves from one or both temporal lobes are highly characteristic and correlate with the temporal lobe MRI changes
- Functional imaging: Hyperperfusion in the temporal lobe on SPECT/PET
- Normal MRI does not exclude HSE - frank encephalitis can occur with normal imaging findings, especially very early in disease
- Hemorrhagic transformation: Small areas of cortical hemorrhage can be seen, as the pathology is a necrotizing hemorrhagic encephalitis
Key Differentiating Points (from other limbic encephalitides)
| Feature | HSV Encephalitis | Autoimmune Limbic Encephalitis |
|---|---|---|
| Onset | Acute (hours-days) | Subacute (weeks) |
| Location | Mesiotemporal, insular, cingulate | Similar but often bilateral |
| Laterality | Unilateral or asymmetric | Often bilateral, more symmetric |
| Gray/white matter | Gray matter predominant | Can be similar |
| Hemorrhage | May be present | Rare |
| ADC restriction | Common | Less common |
Post-HSE Complication
Late autoimmune encephalitis (anti-NMDA receptor antibody mediated) can occur 1-7 weeks after HSE, showing worsening or new MRI changes with a clinical relapse - Goldman-Cecil Medicine.
Sources: Goldman-Cecil Medicine (International Ed.) | Harrison's Principles of Internal Medicine, 22E | Plum & Posner's Diagnosis and Treatment of Stupor and Coma | Bradley & Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.