Latarjet procedure
Reading File
Finding Sources
Finding Sources
Searching PubMed
Latarjet procedure shoulder instability
Reading File
Finding Sources
Searching Images
Latarjet procedure shoulder coracoid transfer glenoid
Reading File
Reading File
Reading File
Now I have comprehensive information. Let me compile the full answer.
Latarjet Procedure
Overview
The Latarjet procedure is an open bony reconstruction of the anterior glenoid using a transferred coracoid process graft to treat recurrent anterior glenohumeral instability. It was originally described by Michel Latarjet in 1954 and remains one of the most reproducible and durable operations for shoulder instability, especially where glenoid bone loss is a factor.
Mechanism of Stability — The "Triple Effect"
The Latarjet achieves stability through three simultaneous mechanisms:
- Bony augmentation — the transferred coracoid graft extends the glenoid arc, increasing articular surface contact area anteroinferiorly
- Dynamic sling effect — the conjoined tendon (short head of biceps + coracobrachialis), which remains attached to the graft tip, acts as a dynamic anterior restraint to anterior humeral translation, especially in the arm-at-risk position (abduction + external rotation)
- Capsulolabral reinforcement — the coracoacromial (CA) ligament stump, preserved during harvest, is used to repair the anterior capsule, adding a static restraint
Indications
| Indication | Detail |
|---|---|
| Glenoid bone loss >13.5–17.3% | Critical threshold above which Bankart repair has unacceptably high failure rates; open Latarjet is preferred |
| >17.3% bone loss (Shin et al.) | Failure rate after ABR = 42.9% vs. 3.7% with <17.3% — clear indication for bony reconstruction |
| Contact/high-demand athletes | Even with 13.5% bone loss, Latarjet is preferred over arthroscopic repair |
| Engaging Hill-Sachs lesion | Combined glenoid + humeral head bone loss ("off-track" lesion) |
| Failed prior Bankart repair | Revision in the setting of bone deficiency |
| Hyperlaxity / generalized ligamentous laxity | Relative indication |
A CT scan with 3D reconstruction is mandatory preoperatively to quantify anterior glenoid bone loss.
Surgical Technique (Open Latarjet)
Positioning: Beach chair; arm holder for variable positioning.
Approach: Deltopectoral incision via a midaxillary crease centered over the coracoid; cephalic vein retracted laterally.
Key steps:
- Incise clavipectoral fascia; expose coracoid and conjoint tendon
- Release pectoralis minor from medial coracoid; free conjoint tendon from fascia
- Resect the CA ligament from the acromion, preserving its full length for later capsule repair
- Harvest the coracoid with a 90° oscillating saw, cutting at the base medial-to-lateral — minimum 1.5–2 cm must be harvested
- Flatten the inferior (articular) surface of the coracoid with the same saw
- Drill two evenly-spaced holes in the coracoid (2.7-mm drill bit)
- Horizontal split of subscapularis at mid-belly; vertical capsulotomy
- Place humeral head retractor; expose anterior glenoid neck and bone loss
- Protect axillary nerve with curved cobra retractor inferiorly
- Flatten the anteroinferior glenoid neck; drill pilot hole ~5–6 mm medial to articular surface
- Transfer coracoid through the subscapularis split; fix flush with the glenoid rim with two partially or fully threaded screws (5-mm osteopenia screws)
- Repair anterior capsule to the preserved CA ligament stump
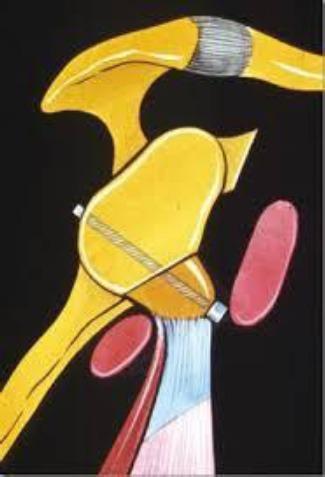
Coracoid process osteotomized and transferred to the anteroinferior glenoid, secured with a compression screw. The conjoined tendon remains attached, providing the dynamic sling effect.
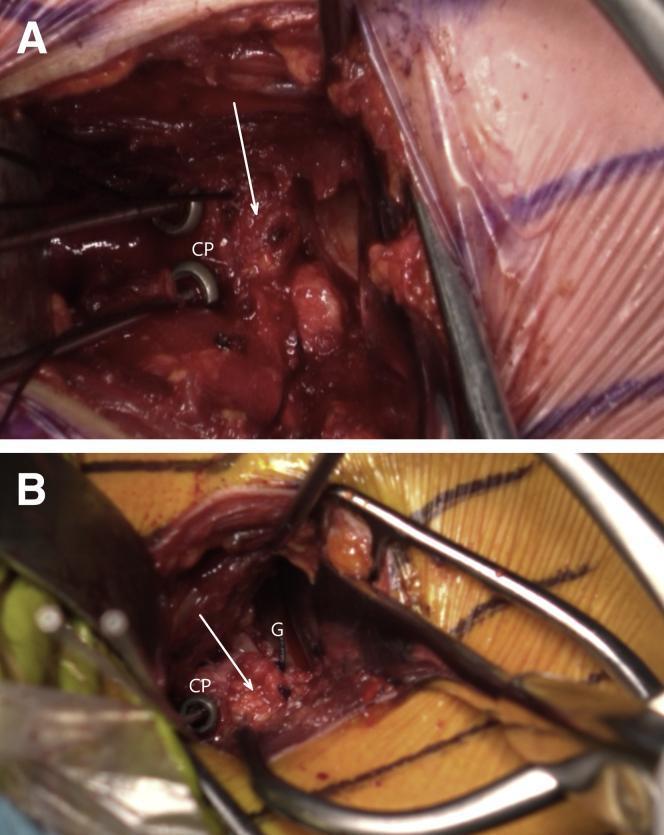
Intraoperative views: (A) coracoid process (CP) in position with labral detachment, (B) labral reattachment completed, glenoid (G) visible.
Graft Positioning — Critical Concept
- The coracoid must be positioned flush with the articular surface of the glenoid (not medial, not proud)
- Lateral overhang causes early glenohumeral arthrosis
- Medial positioning fails to restore glenoid width and leads to recurrence
- Confirmation: Bernageau view on plain X-ray or axial CT postoperatively
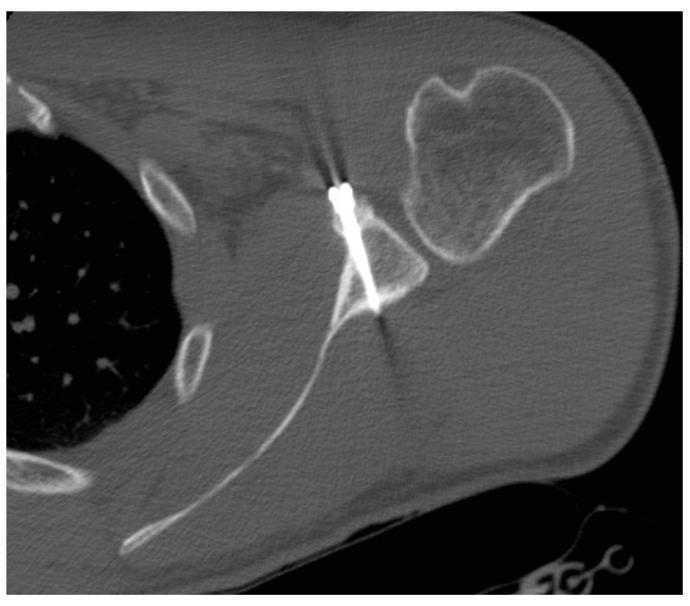
Postoperative axial CT: coracoid graft united at anterior glenoid neck, screw flush with articular surface, no intra-articular protrusion.
Outcomes vs. Bankart Repair
| Measure | Arthroscopic Bankart | Open Bankart | Latarjet |
|---|---|---|---|
| Redislocation rate | 15.1% | 7.7% | 2.7% |
| Instability (sublux + disloc) | 20.2% | 20.8% | 14.8% |
| Rowe score | 85.5 | 87.1 | 87.9 |
| Complication rate | ~0.2–0.3% | ~4.3% | 10.6–15% |
From Rollick NC et al., Sports Med 2017; cited in Rockwood & Green's 10th ed., 2025
Key finding from Zimmerman et al. (360 patients): Latarjet had a 1% redislocation vs. 13% for ABR at 6-year follow-up, with no late failures in the Latarjet group — suggesting superior long-term durability.
Complications
| Complication | Notes |
|---|---|
| Recurrent instability | ~2.9% frank dislocation; ~5.8% subluxation post-Latarjet |
| Bone graft failure | Graft fracture, lysis, non-union |
| Neurologic injury | Musculocutaneous nerve (at risk through conjoint tendon) and axillary nerve (inferior to glenoid) — most common serious complication |
| Glenohumeral arthrosis | Usually from graft malposition (lateral overhang) |
| Infection | Low but higher than arthroscopic |
| Stiffness / ER loss | Expected; typically 10–20° loss of external rotation |
| Hardware-related | Screw loosening, prominence, or intra-articular migration |
Revision After Failed Latarjet
- Revision is challenging; malpositioned graft is the most common cause of recurrence
- Options: Eden-Hybinette procedure (iliac crest autograft or allograft bone block), osteochondral allograft reconstruction
- Schmid et al. (49 patients, failed prior repairs + glenoid deficiency): after revision Latarjet, no further dislocations, 88% rated good/excellent
Arthroscopic Latarjet
An arthroscopic version has been developed for surgeons with advanced shoulder arthroscopy skills. It offers the same anatomical reconstruction with potential benefits of smaller incisions and better capsular visualization, though with a steeper learning curve and similar recurrence rates to the open technique when properly performed.
Rockwood and Green's Fractures in Adults, 10th ed. 2025 (ISBN 9781975211608)
Recent evidence note: A 2024 systematic review (Sarna et al., PMID 39245259) examined surgical options after failed Latarjet — the most current evidence on revision strategies, consistent with the textbook guidance above.
This is a shared conversation. Sign in to Orris to start your own chat.