Give me 10 common heart disease with ecg changes and ecg images of that diseases
Reading File
Finding Sources
Searching the Web
ECG changes 10 common heart diseases images examples STEMI atrial fibrillation heart block
Finding Sources
Loading Image
Reading Web Page
https://mesimedical.com/insights/frequently-diagnosed-condit…
Loading Image
Searching the Web
atrial fibrillation ECG image heart block complete ECG image site:litfl.com OR site:ecgwaves.com
Finding Sources
Loading Image
Searching the Web
STEMI inferior ECG image pericarditis ECG image ventricular tachycardia ECG image litfl
Loading Image
Loading Image
Searching the Web
atrial fibrillation ECG litfl WPW syndrome ECG ventricular tachycardia ECG left ventricular hypertrophy ECG images
Loading Image
Loading Image
Searching the Web
pulmonary embolism ECG S1Q3T3 right bundle branch block ECG left bundle branch block ECG ventricular tachycardia ECG image litfl
Loading Image
Loading Image
I now have excellent ECG images and comprehensive information. Let me compile the full answer:
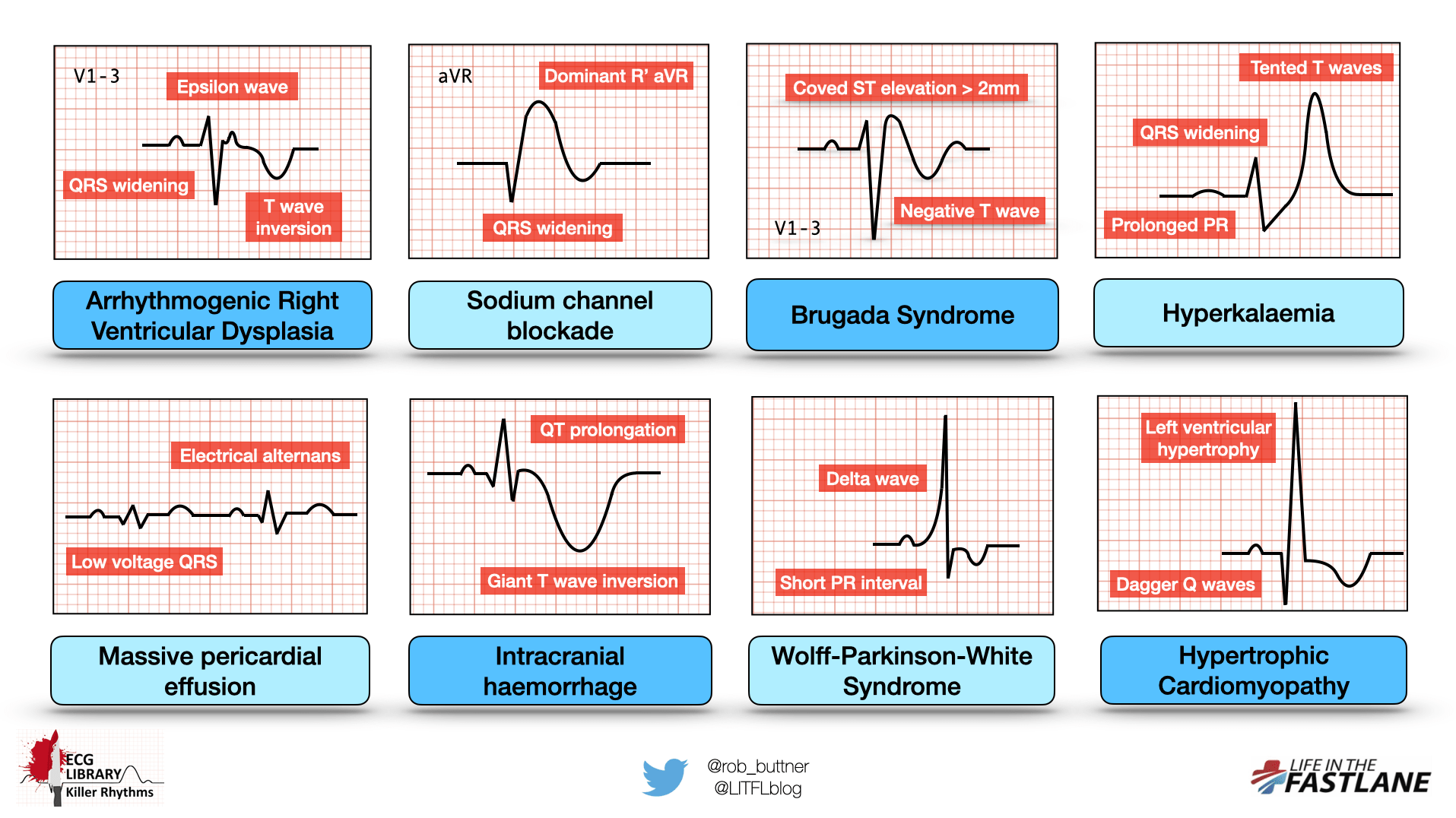
10 Common Heart Diseases with ECG Changes and Images
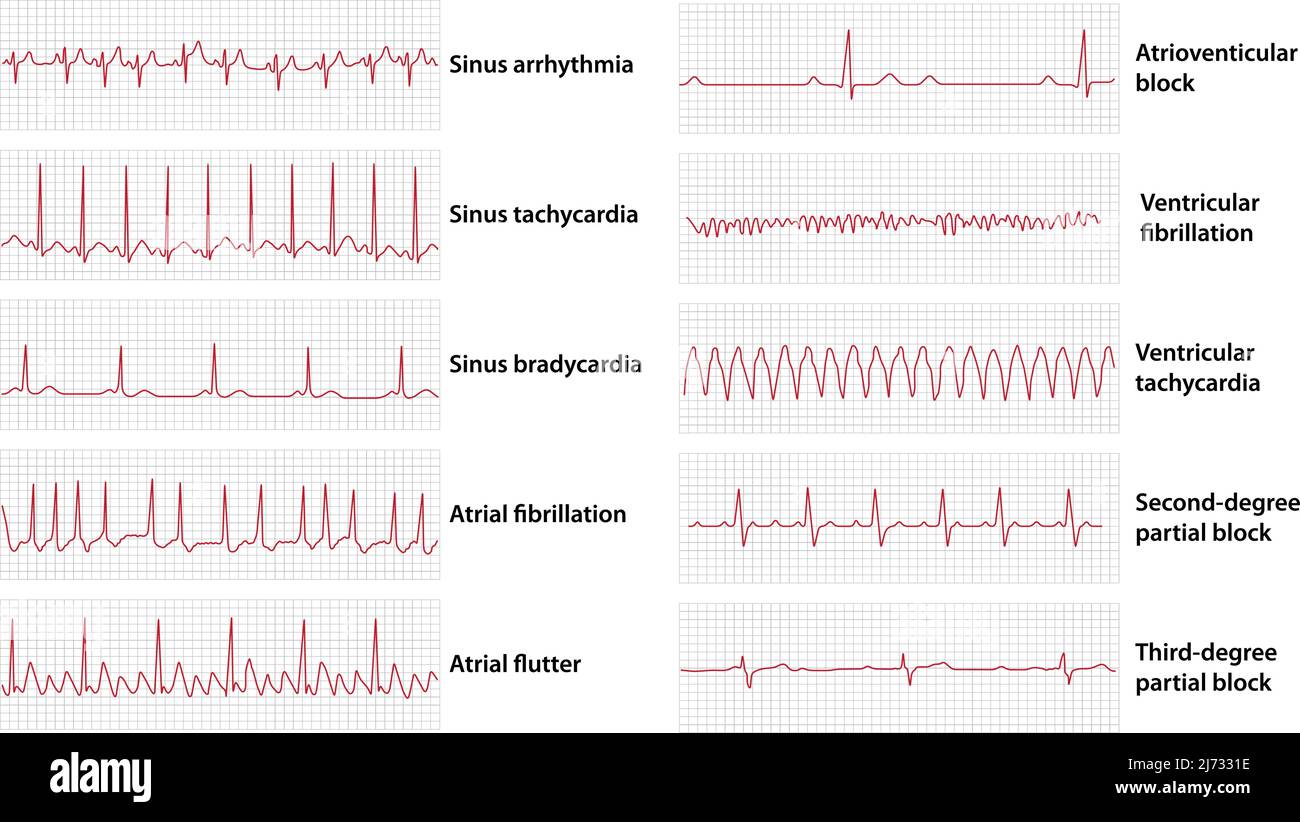
Here is a quick-reference infographic showing ECG patterns across several killer cardiac conditions:
1. ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of a coronary artery causes transmural myocardial ischemia and infarction.
ECG Changes:
- ST elevation ≥1 mm in 2 or more contiguous leads (≥2 mm in V1-V3)
- Hyperacute (peaked, broad) T waves - the very earliest sign
- Development of pathological Q waves (>25% of R wave height, >40ms wide)
- Reciprocal ST depression in opposite leads
- T wave inversion in the evolutionary phase
- Lead localization: Inferior STEMI (II, III, aVF), Anterior STEMI (V1-V4), Lateral STEMI (I, aVL, V5-V6)
ECG Image - Inferior STEMI (massive "tombstone" ST elevations in II, III, aVF):

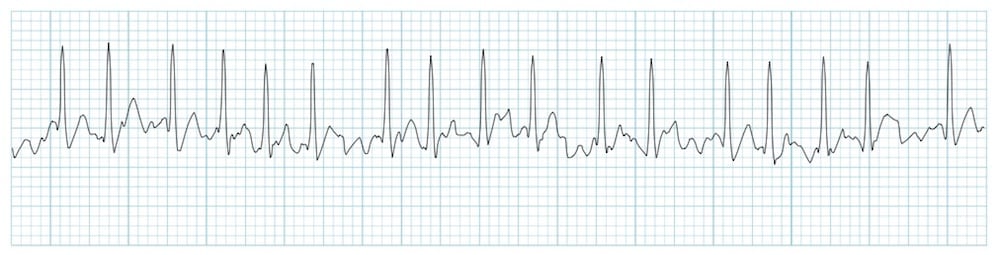
2. Atrial Fibrillation (AF)
Mechanism: Chaotic, disorganized electrical activity in the atria at 350-600 impulses/min. The AV node blocks most impulses, creating an irregular ventricular response.
ECG Changes:
- Absent P waves - replaced by irregular fibrillatory baseline (f-waves)
- Irregularly irregular R-R intervals (the hallmark feature)
- Narrow QRS complexes (unless aberrant conduction or pre-excitation)
- Ventricular rate typically 100-180 bpm in uncontrolled AF
ECG Image - AF with irregular rhythm and absent P waves:
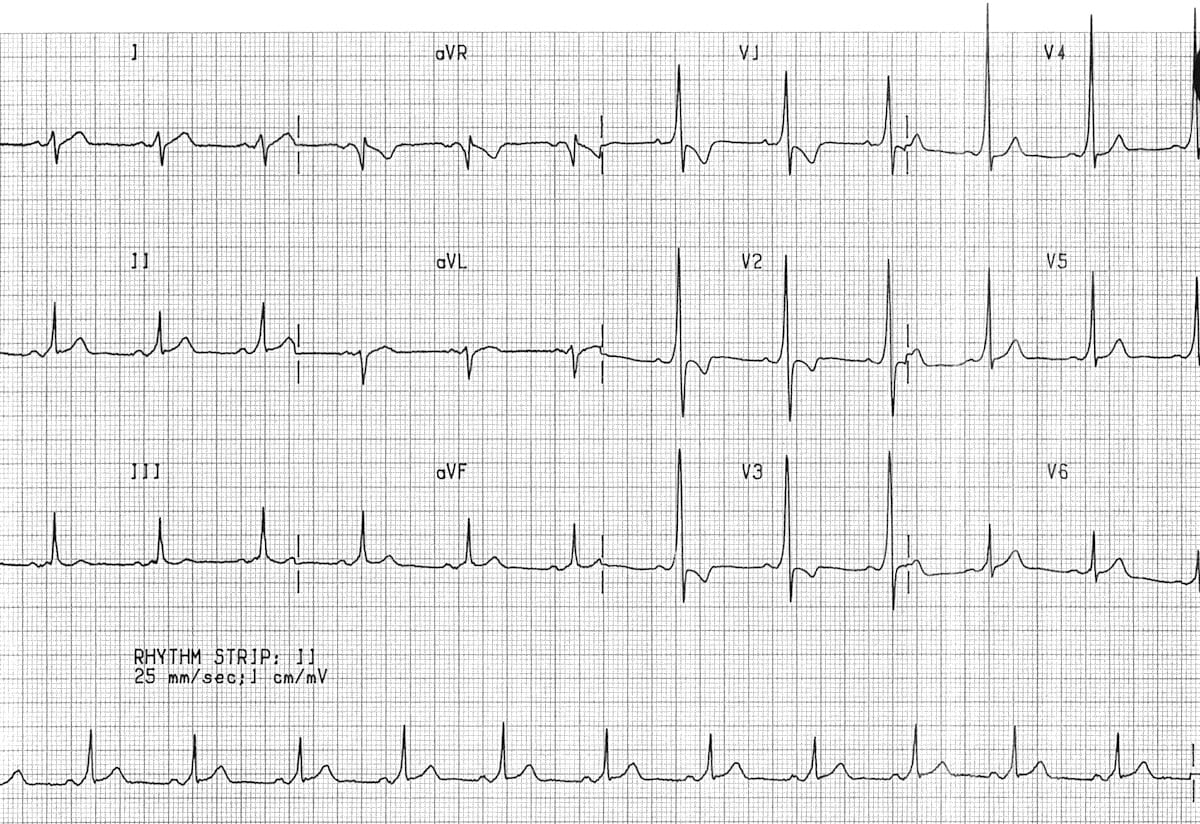
3. Complete Heart Block (3rd Degree AV Block)
Mechanism: Complete failure of AV conduction - no atrial impulses reach the ventricles. The ventricles are driven by a junctional or ventricular escape pacemaker at 20-40 bpm.
ECG Changes:
- P waves present at normal rate (60-100 bpm) but completely dissociated from QRS complexes
- Slow, regular ventricular escape rhythm (30-50 bpm)
- Wide QRS complexes if escape rhythm is ventricular (below Bundle of His)
- Narrow QRS if junctional escape (above Bundle of His)
- AV dissociation is the diagnostic hallmark
ECG Image - Complete Heart Block with AV dissociation:
4. Acute Pericarditis
Mechanism: Inflammation of the pericardium from viral, bacterial, autoimmune, or idiopathic causes. The inflammatory process affects myocardial repolarization globally.
ECG Changes (classically evolves in 4 stages):
- Stage 1 (acute): Widespread concave ("saddle-shaped") ST elevation in most leads (I, II, III, aVF, aVL, V2-V6), with PR segment depression - the most characteristic feature
- Stage 2: Normalization of ST and PR segments
- Stage 3: T wave inversion (diffuse)
- Stage 4: Normalization of T waves
- Notably absent: reciprocal ST depression (unlike STEMI), no Q waves
ECG Image - Pericarditis with saddle-shaped ST elevation and PR depression:

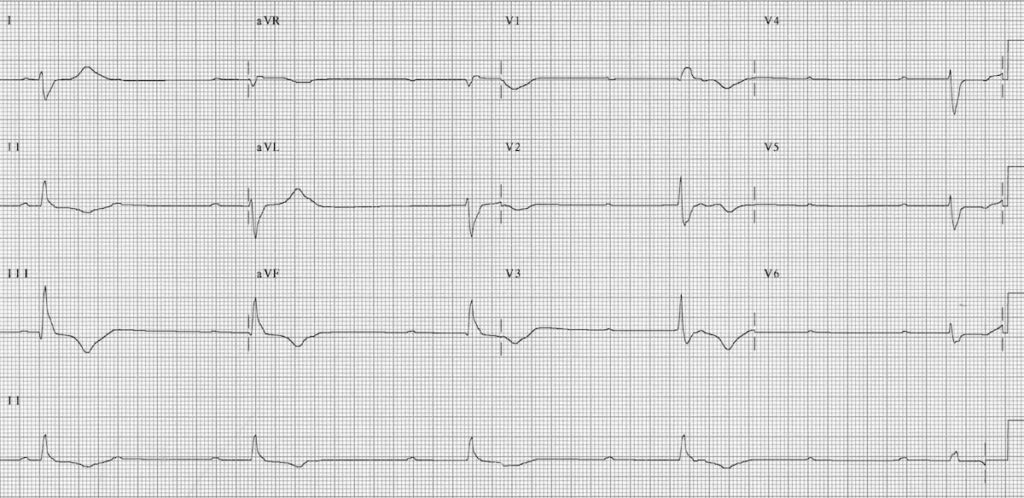
5. Pulmonary Embolism (PE)
Mechanism: Acute right ventricular strain from obstruction of pulmonary vasculature increases RV afterload, causing RV dilatation and altered electrical vectors.
ECG Changes:
- Sinus tachycardia (most common finding - seen in >50%)
- S1Q3T3 pattern (McGinn-White sign): S wave in lead I, Q wave and T wave inversion in lead III
- New right bundle branch block (RBBB) - complete or incomplete
- Right axis deviation
- T wave inversions in V1-V4 (right heart strain pattern)
- Atrial fibrillation or flutter can occur
ECG Image - Massive bilateral PE with sinus tachycardia, S1Q3T3, and right heart strain pattern (T inversions V1-V4):

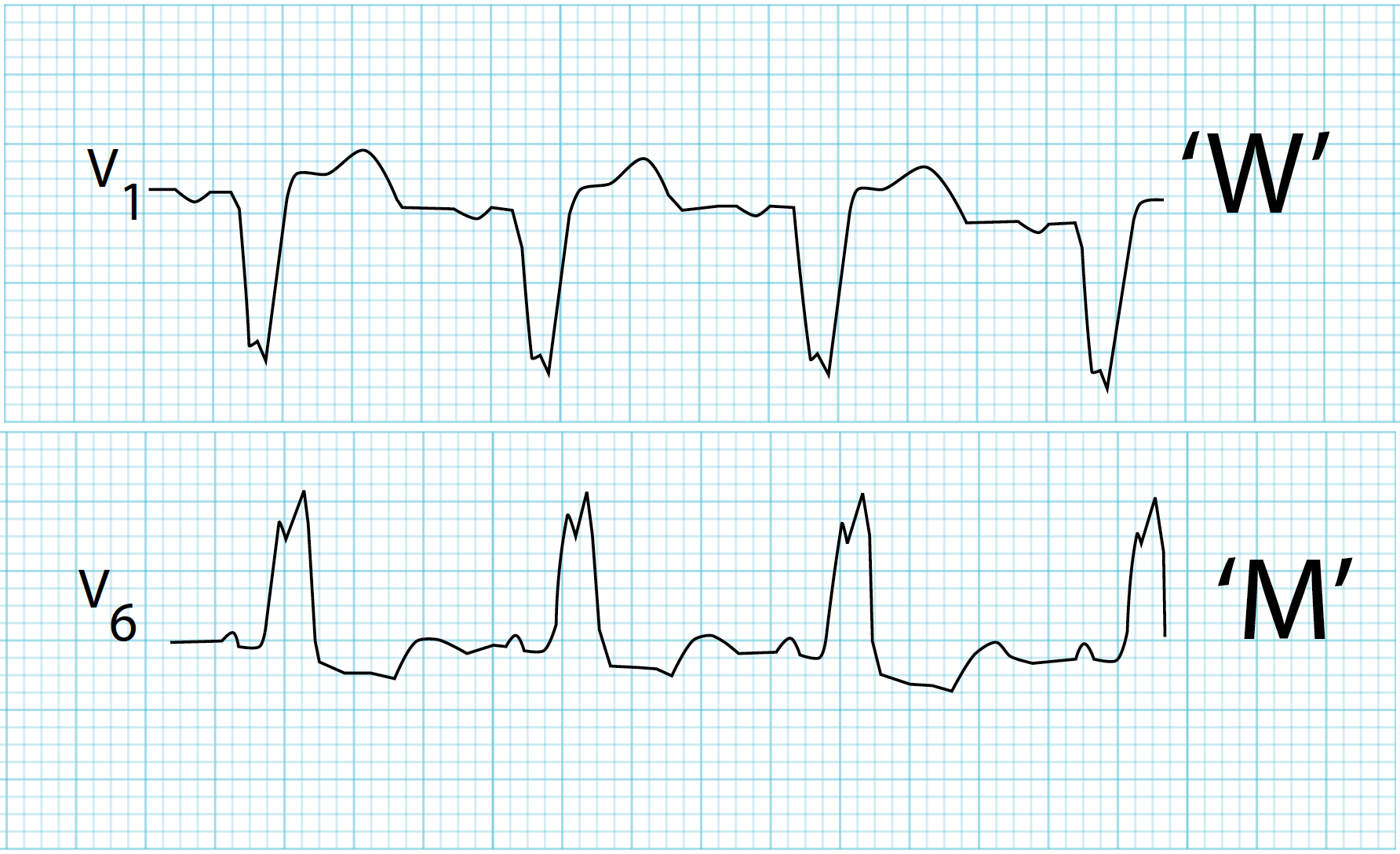
6. Left Bundle Branch Block (LBBB)
Mechanism: Conduction block in the left bundle branch causes abnormal, sequential (right then left) ventricular depolarization producing a broad, notched QRS complex. LBBB is associated with ischemic heart disease, cardiomyopathy, and hypertension. New LBBB should prompt assessment for acute MI (Sgarbossa criteria).
ECG Changes:
- QRS duration ≥120 ms (broad QRS)
- Dominant S wave in V1 (rS or QS pattern) - "W" shape
- Broad, notched ("M-shaped") R wave in V6/I - "M" shape
- Absence of septal Q waves in I and V6
- Discordant ST changes (ST/T in opposite direction to QRS)
- Left axis deviation common
ECG Image - LBBB with classic "W" pattern in V1 and "M" pattern in V6:
7. Wolff-Parkinson-White Syndrome (WPW)
Mechanism: An accessory pathway (Bundle of Kent) bypasses the AV node, causing early ("pre-excitation") ventricular depolarization. This creates the characteristic delta wave.
ECG Changes (in sinus rhythm):
- Short PR interval (<120 ms) - AV bypass
- Delta wave - slurred upstroke of the QRS
- Wide QRS complex (>120 ms total, due to delta wave + normal conduction)
- ST-T wave changes discordant to QRS
- Type A: positive delta and dominant R in V1-V3 (left-sided pathway)
- Type B: negative delta and QS in V1 (right-sided pathway)
- During AF: rapid, broad irregular complexes - life-threatening
ECG Image - WPW (Type A) with short PR, delta wave, and wide QRS in sinus rhythm:
8. Left Ventricular Hypertrophy (LVH)
Mechanism: Pressure overload (hypertension, aortic stenosis) or volume overload causes myocardial hypertrophy, increasing the amplitude of electrical vectors from the left ventricle.
ECG Changes:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men), >20 mm (women)
- Tall R waves in I, aVL, V5-V6
- Deep S waves in V1-V3
- Left axis deviation
- LV "strain" pattern: ST depression and T wave inversion in I, aVL, V5-V6 (secondary repolarization abnormality)
- Prolonged QRS duration (not as wide as LBBB)
ECG Image showing LVH pattern (tall R waves in lateral leads, deep S waves in right precordial leads, with ST-T strain):
9. Ventricular Tachycardia (VT)
Mechanism: Three or more consecutive ventricular ectopic beats at a rate >100 bpm, originating below the Bundle of His. Most commonly occurs in the setting of structural heart disease (post-MI scar, cardiomyopathy).
ECG Changes:
- Broad QRS complexes (≥120 ms) at rate >100 bpm (usually 110-250 bpm)
- AV dissociation - P waves march through the QRS at a different rate (diagnostic when present)
- Fusion beats and capture beats (pathognomonic)
- Concordance: all QRS in precordial leads positive or all negative
- Brugada criteria and Vereckei algorithm used for VT vs SVT with aberrancy
- Morphology criteria: northwest axis, QRS >160 ms favors VT
10. Hypertrophic Cardiomyopathy (HCM)
Mechanism: Genetic disorder (most commonly sarcomere protein mutations) causing asymmetric myocardial hypertrophy. The hypertrophied muscle creates abnormal depolarization and repolarization patterns.
ECG Changes (>90% of patients have an abnormal ECG):
- Left ventricular hypertrophy voltages (giant R waves)
- Pathological Q waves in inferior (II, III, aVF) and lateral (I, aVL, V5-V6) leads - caused by abnormal septal depolarization ("dagger Q waves")
- ST depression and T wave inversion in lateral leads
- Left axis deviation
- P wave changes (left atrial enlargement)
- In apical HCM (Yamaguchi variant): giant, symmetric T wave inversions in V3-V5 (up to -20 to -30 mm)
- Atrial fibrillation can occur as a complication
Quick Summary Table
| # | Condition | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation + Q waves in affected leads |
| 2 | Atrial Fibrillation | Irregularly irregular rhythm, no P waves |
| 3 | Complete Heart Block | Complete AV dissociation, slow escape rhythm |
| 4 | Acute Pericarditis | Widespread saddle-shaped ST elevation + PR depression |
| 5 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, RBBB, RV strain T inversions |
| 6 | LBBB | Wide QRS, "W" in V1, "M" in V6, discordant ST-T |
| 7 | WPW | Short PR, delta wave, wide QRS |
| 8 | LVH | Tall R waves (Sokolow ≥35mm), lateral strain pattern |
| 9 | Ventricular Tachycardia | Broad QRS tachycardia, AV dissociation, fusion beats |
| 10 | HCM | LVH + dagger Q waves in inferior/lateral leads, giant T inversions (apical type) |
Sources: LITFL ECG Library, MESI Medical ECG Guide
Clinical note: ECG interpretation should always be correlated with the patient's clinical presentation, history, and other investigations. No single ECG finding is pathognomonic in isolation.
This is a shared conversation. Sign in to Orris to start your own chat.