Ocular manifestation of diabetes and hypertension from basic to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
diabetic retinopathy hypertensive retinopathy management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I have all the images and comprehensive content from the textbooks. Now let me compile the complete, well-structured answer.
Ocular Manifestations of Diabetes and Hypertension: Basic to Clinical
PART 1: DIABETIC EYE DISEASE
Basic Science: Pathogenesis
The retinal capillary bed normally consists of endothelial cells (with elongated nuclei) supported by pericytes (with rounded nuclei). In the trypsin digest preparation below, this normal architecture is clearly visible:
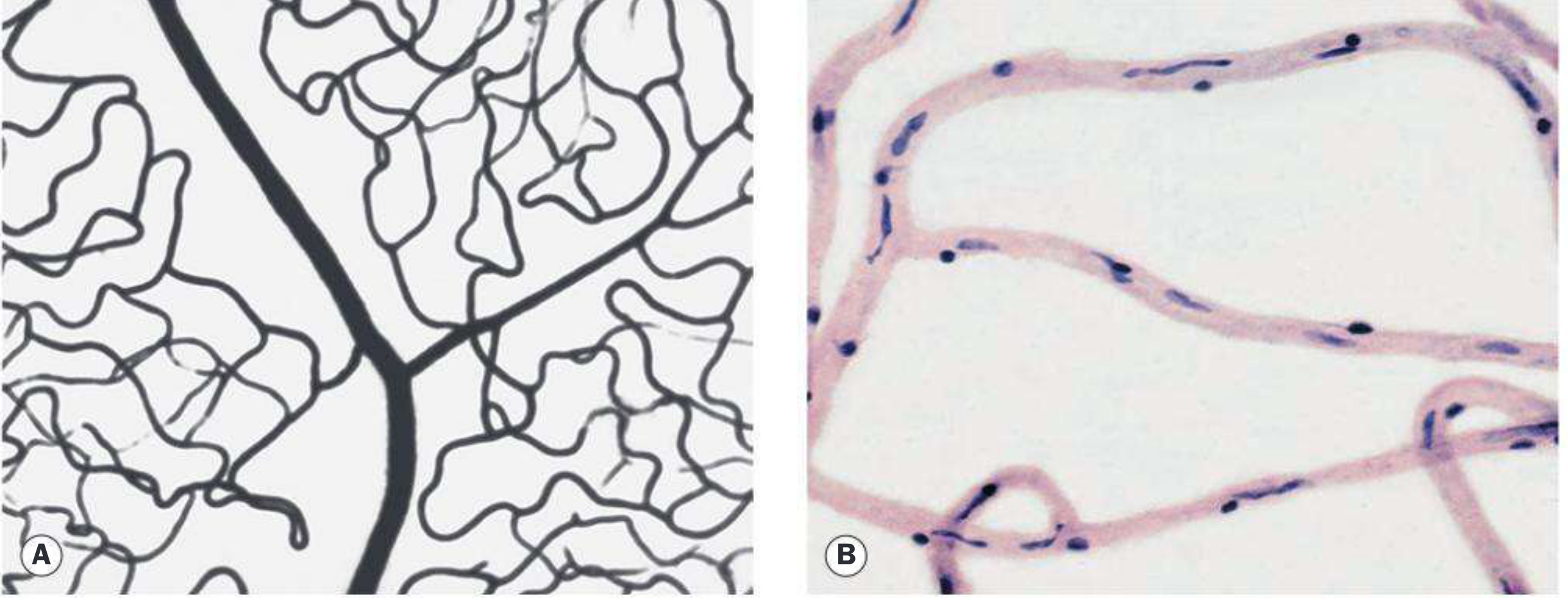
Normal retinal capillary bed: (A) periarteriolar capillary-free zone on flat Indian-ink injection; (B) endothelial cells with elongated nuclei and pericytes with rounded nuclei on trypsin digest. (Kanski's Clinical Ophthalmology)
The key steps in diabetic retinopathy (DR) pathogenesis:
- Pericyte loss - the earliest and most specific histological change. Pericytes regulate capillary autoregulation; their loss destabilizes vessel walls.
- Basement membrane thickening - increased permeability of the blood-retinal barrier (BRB).
- Endothelial cell dysfunction - loss of tight junctions, fluid leakage, and platelet aggregation.
- Capillary occlusion and non-perfusion - leads to retinal ischemia.
- VEGF upregulation - ischemic retina secretes VEGF, driving neovascularization, edema, and ultimately blindness.
Risk Factors for DR Progression
(Kanski's Clinical Ophthalmology, 10th ed.)
| Factor | Effect |
|---|---|
| Duration of diabetes | Most important predictor; DR rare within 5 years of onset |
| Poor glycemic control | Higher HbA1c = higher risk; DCCT confirmed tight control prevents/delays DR |
| Hypertension | Target BP <140/80 mmHg; especially important in type 2 with maculopathy |
| Nephropathy | Worsening nephropathy worsens DR |
| Pregnancy | Can accelerate progression; ~5% with mild DR and ~33% with moderate DR progress to PDR during pregnancy |
| Pioglitazone | Associated with worsening diabetic macular edema |
| Hyperlipidaemia, anaemia | Additional risk factors |
- Prevalence: ~40% of all diabetics; 67% of type 2 diabetics have DR at 10 years
- DR is the most common cause of new blindness in industrialized countries in working-age adults
Complete Spectrum of Ophthalmic Complications of Diabetes
(Kanski's Clinical Ophthalmology 10th)
Common:
- Maculopathy (diabetic macular edema and macular ischemia)
- Retinopathy - neovascularization of disc/retina, vitreous hemorrhage
- Unstable refraction (lens changes with fluctuating glucose)
Uncommon:
- Recurrent styes (hordeola)
- Accelerated age-related cataract
- Tractional retinal detachment
- Neovascularization of iris and angle
- Neovascular glaucoma (NVG)
- Ocular motor nerve palsies (CN III, IV, VI)
- Reduced corneal sensitivity
Rare:
- Papillopathy
- Pupillary light-near dissociation
- Wolfram syndrome
- Acute-onset cataract
- Rhino-orbital mucormycosis
Classification: Diabetic Retinopathy Disease Severity Scale
(Wills Eye Manual; ETDRS-based International Classification)
| Stage | Definition |
|---|---|
| No apparent DR | Normal fundus |
| Mild NPDR | Microaneurysms only |
| Moderate NPDR | More than mild but less than severe; may have cotton-wool spots (CWSs), venous beading |
| Severe NPDR | Any of: >20 intraretinal hemorrhages in all 4 quadrants; venous beading in 2+ quadrants; prominent IRMA in 1+ quadrant (the "4-2-1 rule") |
| PDR | Neovascularization of iris (NVI), angle (NVA), disc (NVD), elsewhere (NVE); or vitreous/preretinal hemorrhage |
| DME | Can occur at any stage; clinically significant when involving or threatening fovea |
Key Clinical Signs in Detail
NPDR signs:
- Microaneurysms - dot-like outpouchings, earliest funduscopic sign, seen on fluorescein angiography before ophthalmoscopy
- Dot-blot hemorrhages - intraretinal, round (from capillary rupture in the deep nuclear layers)
- Hard exudates - lipoprotein deposits from leaking capillaries; form rings around leaking microaneurysms
- Cotton-wool spots (CWSs) - nerve fiber layer infarcts (soft exudates), indicate ischemia
- Venous beading - irregular venous caliber, indicates severe ischemia
- IRMA (intraretinal microvascular abnormalities) - dilated shunts within ischemic retina
PDR signs:
- Neovascularization (NVD, NVE) - fragile new vessels on disc or elsewhere
- Preretinal/vitreous hemorrhage from neovascular rupture
- Fibrovascular proliferation leading to tractional retinal detachment
Diabetic Macular Edema (DME):
- Can occur at any stage of DR
- Center-involving DME threatening fovea = indication for treatment
- Identified by OCT (thickening) and FA (leakage patterns)
Differential Diagnosis of NPDR
| Condition | Distinguishing Features |
|---|---|
| CRVO | Optic disc swelling, more dilated/tortuous veins, flame-shaped hemorrhages in NFL; unilateral sudden onset |
| BRVO | Hemorrhages along a vein, do not cross horizontal raphe |
| Hypertensive retinopathy | Flame-shaped hemorrhages, few microaneurysms, arteriolar narrowing + AV nicking |
| Radiation retinopathy | History of irradiation; microaneurysms rare |
| Ocular Ischemic Syndrome | Midperipheral hemorrhages, episcleral injection, pain; usually unilateral |
Treatment of Diabetic Eye Disease
Systemic:
- Tight glycemic control (HbA1c target): DCCT and UKPDS demonstrate prevention/delay of DR
- Tight BP control (<140/80 mmHg)
- Lipid control
Diabetic Macular Edema (Center-involving):
- Anti-VEGF injections (first-line) - FDA-approved: ranibizumab, aflibercept; off-label: bevacizumab
- Intravitreal corticosteroids - dexamethasone implant or fluocinolone acetonide for anti-VEGF non-responders; risks include cataract and raised IOP
- Focal macular laser - for extrafoveal microaneurysms; also considered when anti-VEGF/steroids contraindicated
Proliferative DR (PDR) - High-Risk Characteristics requiring PRP:
- NVD > 1/4 to 1/3 disc area
- Any NVD with preretinal/vitreous hemorrhage
- NVE > 1/2 disc area with preretinal/vitreous hemorrhage
- Any NVI or NVA
Treatment options for PDR:
- Panretinal photocoagulation (PRP) - standard treatment
- Anti-VEGF - preferred initial therapy when DME coexists or vitreous hemorrhage limits view to peripheral retina; use cautiously if follow-up unreliable
Indications for Vitrectomy:
- Dense non-clearing/recurrent vitreous hemorrhage
- Tractional RD involving the macula
- Macular ERM or vitreomacular traction
- Dense premacular hemorrhage
- Chronic DME refractory to other treatments
- Severe fibrovascular proliferation unresponsive to laser/anti-VEGF
With effective screening and implementation of ETDRS and anti-VEGF trial evidence, risk of severe visual loss can be reduced to less than 5%. (Kanski's)
PART 2: HYPERTENSIVE EYE DISEASE
Basic Science: Pathogenesis
Hypertension damages the retinal vasculature through two main mechanisms:
- Vasospasm/autoregulation - early response to elevated pressure; manifests as arteriolar narrowing
- Arteriosclerosis - chronic structural change from intimal thickening and hyalinization; manifests as copper/silver wiring and AV nicking
The choroidal circulation, having no autoregulation, is disproportionately affected in acute/malignant hypertension, leading to ischemic infarcts of the choroid (Elschnig spots) and exudative retinal detachment.
Classification: Keith-Wagener-Barker (KWB) Grading
(Textbook of Family Medicine 9e; Scheie classification)
Hypertensive Retinopathy:
| Grade | Signs |
|---|---|
| Grade 1 | Generalized attenuation of retinal arterioles |
| Grade 2 | More pronounced and focal arteriolar attenuation |
| Grade 3 | Grade 2 + retinal exudates, cotton-wool spots, hemorrhages |
| Grade 4 | Grade 3 + papilledema |
Arteriosclerotic Changes (Scheie grading):
| Grade | Signs |
|---|---|
| Grade 1 | Broadening of arteriolar reflex; minimal AV crossing defects |
| Grade 2 | Increased arteriolar light reflex; AV crossing changes |
| Grade 3 | Copper-wire arterioles; marked AV crossing changes |
| Grade 4 | Silver-wire arterioles; severe AV crossing changes |
Clinical Signs
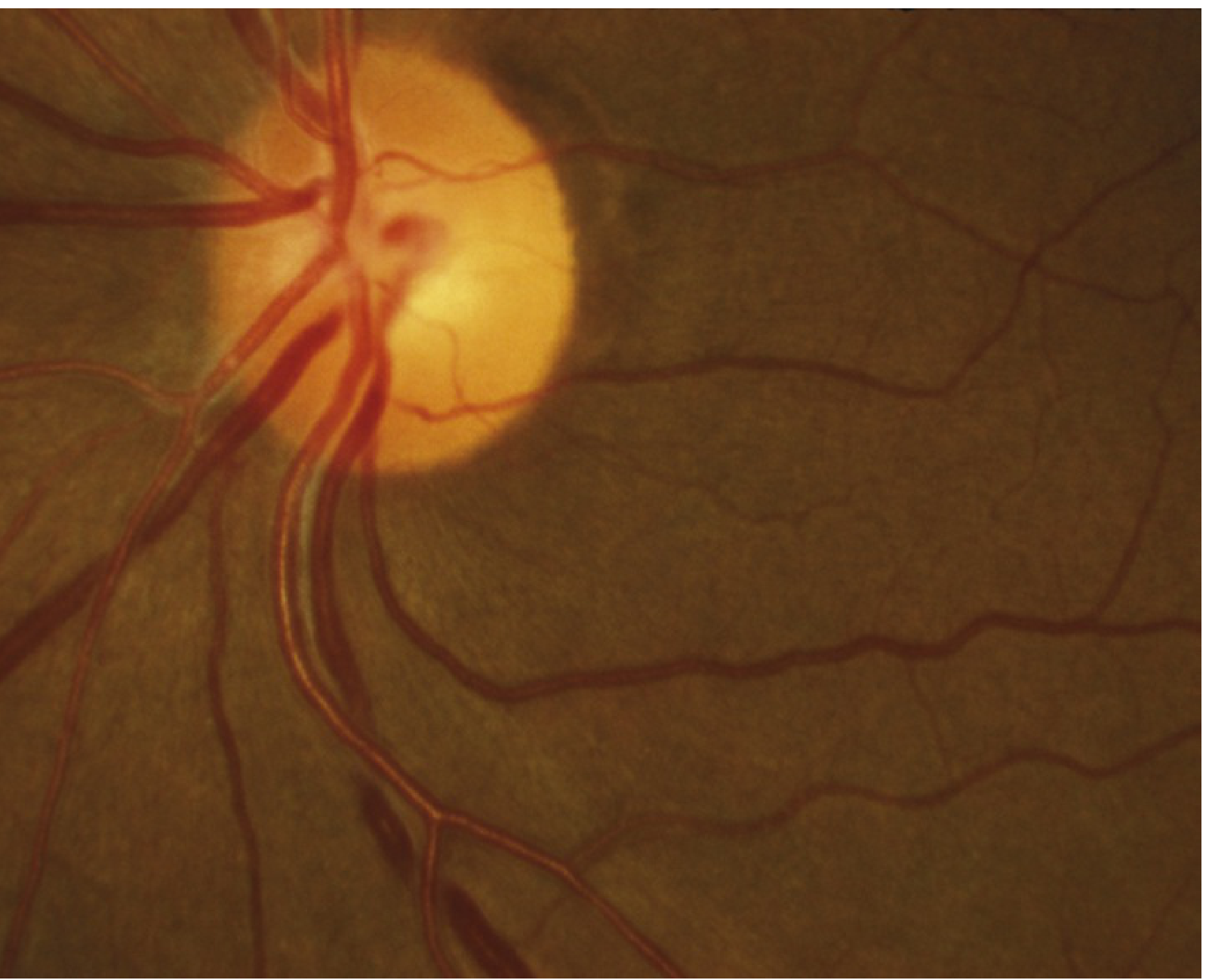
Chronic hypertensive retinopathy: arteriolar narrowing and AV nicking. (Wills Eye Manual)
Chronic Hypertension:
- Generalized or localized retinal arteriolar narrowing - almost always bilateral (critical sign)
- AV nicking (AV crossing changes) - arteriole compresses the vein at crossings
- Copper wiring - increased light reflex, arteriole wall thickened/sclerotic
- Silver wiring - arteriole wall so opaque the blood column is invisible
- Flame-shaped hemorrhages (nerve fiber layer)
- CWSs (ischemic infarcts)
- Arterial macroaneurysms
- Central or branch retinal artery/vein occlusion
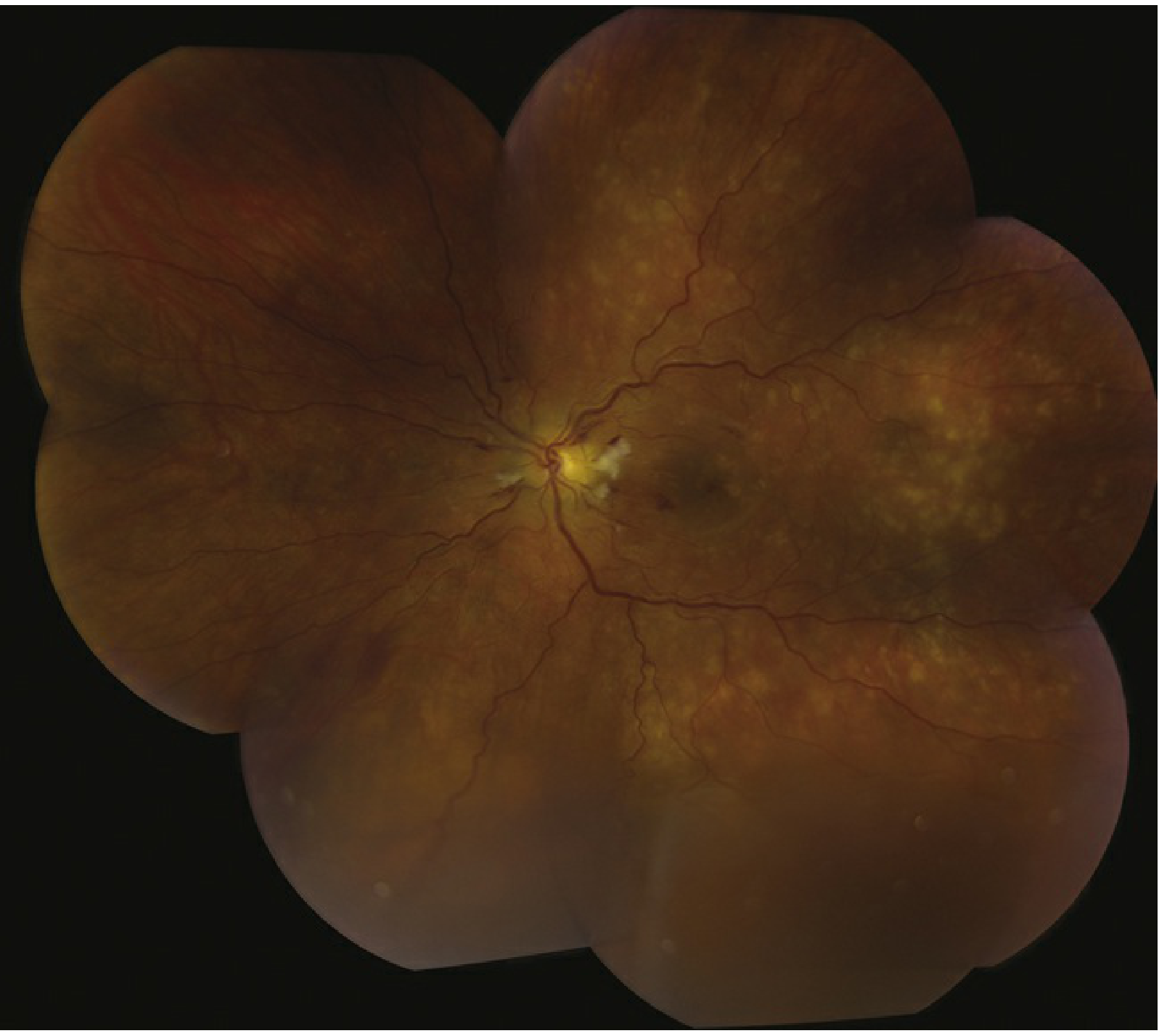
Acute (malignant) hypertensive retinopathy: widespread yellow exudates, hemorrhages, and disc edema. (Wills Eye Manual)
Acute / Malignant Hypertension:
- Hard exudates in macular star configuration (leakage in Henle's fiber layer)
- Retinal edema
- CWSs
- Flame-shaped hemorrhages
- Optic nerve head edema (papilledema) - Grade 4 / malignant hypertension
- Rarely: serous retinal detachment or vitreous hemorrhage
- Elschnig spots - focal areas of chorioretinal atrophy from previous choroidal infarcts; sign of past episodes of acute hypertension
Hypertensive Choroidopathy (predominantly in malignant hypertension)
- Choroidal ischemia/infarcts
- Elschnig spots (pigmented halos around choroidal infarcts)
- Siegrist streaks (linear arrays of pigmentation along choroidal arteries)
- Can cause serous exudative retinal detachment
Key Clinical Pearl
If hypertensive retinopathy appears UNILATERAL, suspect ipsilateral carotid artery obstruction on the side of the normal-appearing eye - the carotid stenosis protects the ipsilateral retina from the effects of systemic hypertension. (Wills Eye Manual)
Workup for Hypertensive Retinopathy
- History: Known hypertension, diabetes, prior adnexal radiation?
- Measure blood pressure immediately
- Complete dilated fundus examination
- Refer urgently if: systolic BP ≥180 mmHg, diastolic BP ≥110 mmHg, or if symptomatic (chest pain, headache, altered mental status, blurred vision with disc swelling)
- Workup for secondary causes of hypertension (renal artery stenosis, pheochromocytoma, hyperaldosteronism, etc.)
Treatment: Control hypertension (per internist). Ophthalmic changes are largely reversible with adequate BP control in early-stage disease.
Follow-up: Every 2-3 months initially, then every 6-12 months.
Differential Diagnosis: DR vs. Hypertensive Retinopathy
| Feature | Diabetic Retinopathy | Hypertensive Retinopathy |
|---|---|---|
| Hemorrhage type | Dot-blot (deep retinal) | Flame-shaped (NFL) |
| Microaneurysms | Common, characteristic | Rare |
| Hard exudates | Common, ring-shaped around leaking vessels | Less prominent |
| Arteriolar changes | Vessel attenuation less prominent | AV nicking, copper/silver wiring prominent |
| Neovascularization | Common in PDR | Rare |
| Papilledema | Not typical (diabetic papillopathy is distinct) | Present in Grade 4 (malignant) |
| Macular star | Not typical | Classic in malignant HTN |
| Laterality | Bilateral, symmetric | Bilateral (unilateral = consider carotid stenosis) |
Overlap: When Diabetes and Hypertension Coexist
- Hypertension is very common in type 2 diabetes and accelerates DR progression
- Target BP <140/80 mmHg in all diabetics with retinopathy
- Tight BP control is particularly beneficial in type 2 diabetics with maculopathy
- Both conditions cause CWSs and retinal hemorrhages - careful fundoscopic analysis is needed to distinguish the predominant pathology
- CRVO and BRVO (vein occlusions) are more common when both conditions are present
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.
- Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease
- Textbook of Family Medicine, 9th ed.
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.