Medial joint height of knee is reduced on xray
Reading File
Finding Sources
Finding Sources
Searching the Web
medial joint space narrowing knee X-ray causes diagnosis clinical significance
Reading File
Reading File
Loading Image
Finding Sources
Here is a structured answer on reduced medial joint height (medial joint space narrowing) on knee X-ray:
Medial Joint Space Narrowing on Knee X-ray
What It Means
Reduction in the medial joint height on X-ray reflects loss of articular cartilage in the medial (tibiofemoral) compartment. It is the primary radiographic indicator of medial compartment osteoarthritis (OA) of the knee. The joint space on X-ray represents the combined thickness of the articular cartilage on both the femoral condyle and tibial plateau - cartilage itself is radiolucent, so when it thins or disappears, the bones appear to come closer together.
Why the Medial Side First?
The medial compartment is the most commonly affected in knee OA. The normal limb alignment places ~60-70% of loading forces through the medial side. Varus malalignment (bow-legs) accelerates this further. As noted in Campbell's Operative Orthopaedics 15th Ed 2026:
"The most common deformity in patients with osteoarthritis of the knee is varus malalignment, which causes stresses to be concentrated medially, accelerating degenerative changes in the medial part of the joint."
Kellgren-Lawrence (KL) Grading System
This is the standard grading system based on the AP knee radiograph. The two primary features rated are osteophytes and joint space narrowing:
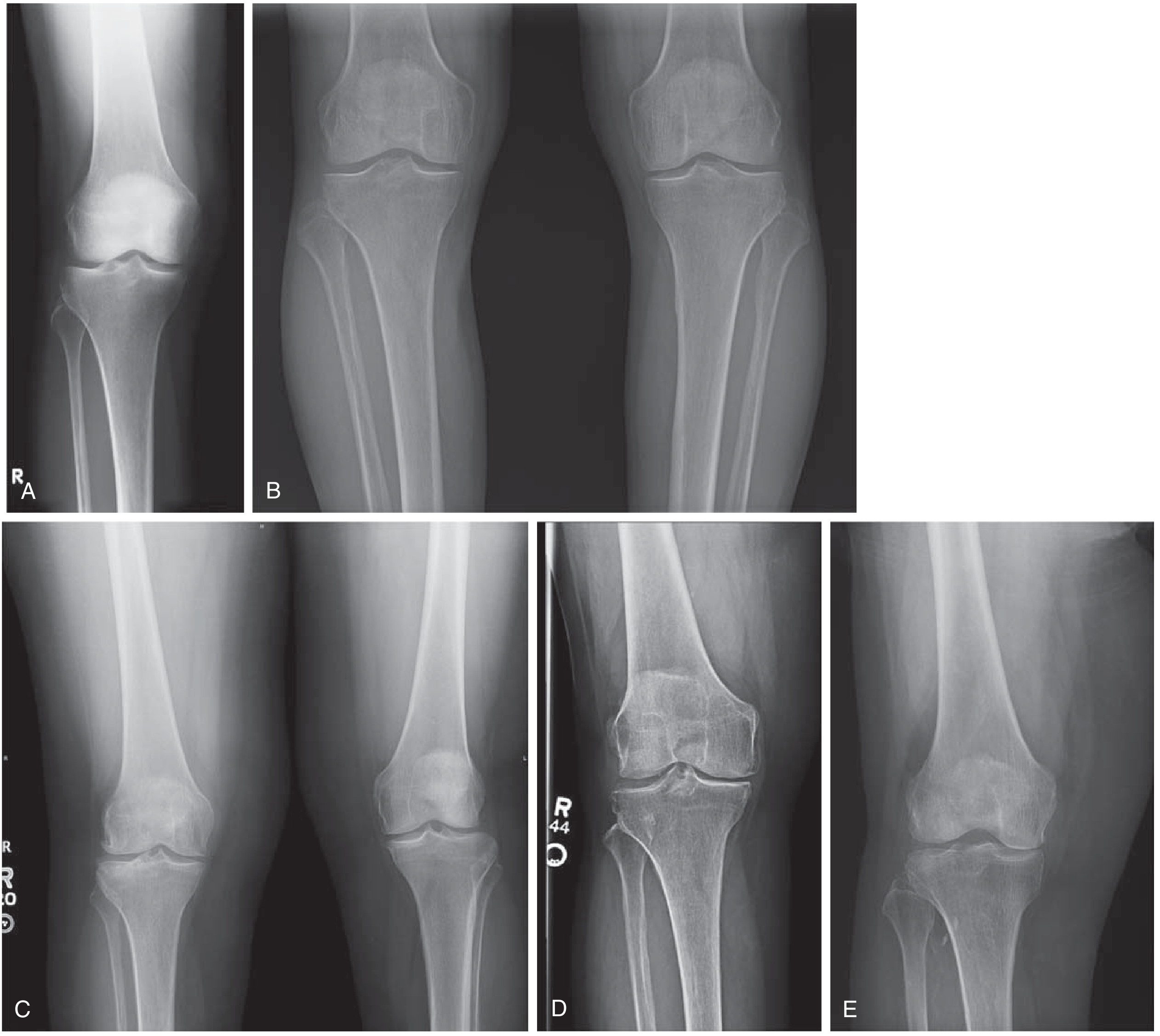
(Miller's Review of Orthopaedics, Fig. 5.73 - KL Grades 0 through 4)
| KL Grade | Findings | Interpretation |
|---|---|---|
| 0 | Normal, symmetrical joint spaces | No OA |
| 1 | Small tibial spine osteophyte; suspected medial JSN | OA possibly present |
| 2 | Marginal osteophytes; JSN <50%; normal bone contours | OA present, minimal |
| 3 | Significant osteophytes; joint space loss >50%; subchondral sclerosis; early bone deformity | OA moderate |
| 4 | Prominent osteophytes; joint space absent; subchondral sclerosis with cysts; bone deformity with femoral condyle flattening; medial tibial bone loss | OA severe |
- Miller's Review of Orthopaedics 9th Ed
Key Radiographic Features of Medial Compartment OA
- Joint space narrowing - medial > lateral (asymmetric)
- Subchondral sclerosis - white (dense) bone beneath the cartilage
- Subchondral cysts - small lucencies in subchondral bone
- Osteophytes - bony spurs at joint margins and tibial spines
- Varus deformity - the classic "bow-leg" alignment from medial collapse
- Bone deformity - flattening of medial femoral condyle in late disease
Important Radiology Tip: Weight-Bearing Views Are Essential
Non-weight-bearing (supine) films frequently underestimate the severity of cartilage loss. A weight-bearing view (especially semi-flexed, posterior-anterior) is the most sensitive projection.
As described in Firestein & Kelley's Textbook of Rheumatology:
"The supine view demonstrates mild osteophytosis and possible subtle joint space narrowing in the medial compartment, whereas in the weight-bearing view, severe medial joint space narrowing is present, indicating severe cartilage damage."
The standard knee OA X-ray series should include:
- Weight-bearing AP view (most important)
- 45-degree semi-flexed weight-bearing PA view (most sensitive for JSN)
- Lateral view
- Sunrise/Merchant view (patellofemoral compartment)
- Full-length standing AP (hip to ankle) - to assess overall limb alignment
Differential Diagnosis of Medial Joint Space Narrowing
| Cause | Distinguishing Features |
|---|---|
| Osteoarthritis (most common) | Asymmetric JSN, osteophytes, sclerosis, no erosions, middle-aged/elderly |
| Medial meniscus tear/loss | JSN without osteophytes; MRI confirms |
| Rheumatoid arthritis | Symmetric JSN, periarticular osteoporosis, erosions, bilateral |
| Post-traumatic arthritis | History of fracture/injury, may be younger patient |
| Spontaneous osteonecrosis of knee (SONK) | Subchondral collapse of medial femoral condyle; preserved or reduced JSN; sudden onset pain |
| Septic arthritis (old) | Rapid JSN, joint destruction, history |
Clinical Correlation
- Medial JSN correlates with medial knee pain, especially on weight-bearing and stair climbing
- A degenerative medial meniscus tear is very commonly coexistent with medial OA
- The resulting varus deformity increases medial compartment loading, creating a vicious cycle
- High tibial osteotomy (HTO) is a surgical option in younger patients with isolated medial OA and varus deformity - it offloads the medial compartment by correcting alignment to slight valgus
- Total/unicompartmental knee replacement is the definitive treatment in severe cases
Sources: Miller's Review of Orthopaedics 9th Ed | Firestein & Kelley's Textbook of Rheumatology | Campbell's Operative Orthopaedics 15th Ed 2026 | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.