








Explain each question and explain further respectively
KMTC Radiology / Orthopaedics MCQ Paper - Full Explanations
SECTION A: MULTIPLE CHOICE QUESTIONS
Q1. The main source of unnecessary irradiation to patients - Which one is NOT?
Q2. The main radiological method of liver examination in children
- Uses no ionizing radiation (safe for pediatric patients)
- Is non-invasive and painless
- The liver is a superficial, large organ easily accessed by ultrasound
- Readily available and inexpensive
Q3. Rheumatoid arthritis primarily involves
Q4. The following when seen in a radiograph means R or L
Q5. The following does NOT use ionizing radiation
- CT scan - uses X-rays (ionizing radiation)
- Ultrasound - uses HIGH-FREQUENCY SOUND WAVES (no ionizing radiation)
- OPG (Orthopantomogram/dental panoramic x-ray) - uses X-rays
- X-ray - uses ionizing radiation
Q6. Spiral fracture is due to
Q7. Fracture may appear in the radiograph EXCEPT
- a) Loss of continuity of the cortex - YES, cortex breaks
- b) Dark line traversing the bone - YES, lucent fracture line
- c) Dense/sclerotic line if fracture ends overlap (impacted fracture) - YES
Q8. The meaning of the 10-day rule in radiation protection
Q9. Which is NOT a way to minimize radiation dose received by patients and staff
- a) Reducing gonad dose to the general population - YES, use gonad shielding
- b) Protecting radiosensitive tissues - YES
- d) Ensuring staff receive low levels via distance, shielding, monitoring - YES
Q10. What tumour has a similar radiological picture as osteomyelitis?
- Periosteal reaction ("onion-skin" periosteal layering in Ewing's)
- Bone destruction
- Soft tissue mass
- Fever, raised ESR, raised WBC (in osteomyelitis AND Ewing's)
- Permeative bone destruction pattern
Q11. The radiological picture of bone destruction in osteomyelitis occurs
- Bone destruction only becomes visible when >30-50% of bone mineral content is lost
- This takes approximately 10-14 days (second week) from onset
- Early disease (first hours, first day, first few days) shows NO x-ray changes
Q12. Cartilages as seen on ultrasound
Q13. The most specific radiological feature of CHRONIC osteomyelitis
- Osteophytes = osteoarthritis
- Generalized sclerosis = seen in many conditions
- Linear periostitis = seen in both acute and chronic infection
Q14. Which is NOT TRUE regarding radiological densities
- Air/Gas - darkest (black)
- Fat - dark grey
- Soft tissue/Water - grey
- Bone/Calcium - white
- Metal - BRIGHTEST WHITE (most dense)
Q15. Which is NOT TRUE on radiological densities
- a) Calcification in tendons/vessels increases soft tissue density - TRUE
- b) Sclerotic lesions show increased density - TRUE
- d) Calcified cartilage/menisci cause dense lines in joint space - TRUE
Q16. Radiological examination of shoulder trauma - EXCEPT which view?
- AP external rotation view - standard
- AP internal rotation view - standard
- Axillary view - essential to detect posterior dislocations
- Grashey view (true AP of glenohumeral joint) - standard
Q17. Which is NOT a characteristic of a good X-ray
- a) At least two views required - TRUE (one view is never sufficient)
- b) Entire anatomical area should be included - TRUE
- d) Nature of soft tissue may speak for occult fractures - TRUE (soft tissue swelling can indicate hidden fractures)
Q18. Which is NOT a cause of generalized increased bone density on X-ray?
- Fluorosis - causes dense bones (skeletal fluorosis)
- Myelosclerosis - bone marrow replaced by fibrous tissue, leading to dense bone
- Metastatic bone tumours - prostate, breast mets can be sclerotic
Q19. Which is NOT true regarding X-rays as used in traumatology?
- A fracture may only be visible in one plane
- Displacement/angulation cannot be assessed in one view
- The standard is TWO views (e.g., AP + Lateral)
- Both joints above and below the fracture must be included - TRUE
- X-ray of both limbs may be needed (especially in children, for comparison) - TRUE
- X-rays taken on two different occasions to ascertain fracture (stress fractures may not be initially visible) - TRUE
Q20. TRUE regarding callus formation in fracture healing
- b) Small haematoma = small callus (FALSE - large haematoma = more callus)
- c) Marked displacement = more callus (TRUE, but the statement is already answered by a)
- d) Rigid fixation in close apposition = LESS callus (primary/direct bone healing without visible callus)
Q21. NOT TRUE regarding fracture lines as seen in X-rays
- b) Fracture pattern indicates causative force - TRUE (spiral = torsion, transverse = direct blow)
- c) Greenstick = incomplete break in resilient children's bones - TRUE
- d) Impacted = fragments driven into each other with no movement - TRUE
Q22. NOT TRUE on rate of bone union as seen in X-rays
- a) Callus visible on X-ray within 2 weeks in young children - TRUE
- b) Union is slower in older children than younger ones - TRUE
- d) Hard cortical bone takes longer to heal than cancellous bone - TRUE (cortical/diaphyseal fractures take longer than metaphyseal/cancellous fractures)
Q23. NOT a cause of pathological fractures
- Pyogenic osteomyelitis - weakens bone
- Bone tumours - primary or metastatic destroy bone
- Osteoporosis - reduced mineral density
Q24. To ascertain sound union - which feature is NOT present in well-united bone?
- b) No pain over the fracture site - sign of union
- c) Callus visible on x-ray - sign of healing
- d) Continuity of bone trabeculae across the fracture on x-ray - definitive sign of union
Q25. Late complications of fractures - which is NOT?
- Avascular necrosis (AVN) - blood supply interruption leading to bone death
- Shortening - malunion with limb length discrepancy
- Volkmann's ischaemic contracture - compartment syndrome sequela with muscle fibrosis
Q26. Features associated with non-union - which is NOT?
- a) Interposition of soft tissues - prevents bone contact
- b) Excessive movement at fracture line - disrupts healing tissue
- d) Severed blood supply - avascular necrosis
Q27. NOT true about fracture lines of the forearm
- Nightstick fracture = isolated mid-shaft ulna fracture (from direct blow, like defending against a nightstick) - TRUE
- Colles' fracture = distal radius fracture with DORSAL displacement ("dinner fork deformity") - TRUE
- Smith's fracture = distal radius fracture with VOLAR/palmar displacement (reverse Colles') - TRUE (visible on next question)
Q28. Radiological features of Rickets - which is NOT?
- a) Broadening/widening of the metaphysis - TRUE (unmineralized osteoid accumulates)
- b) Rarefaction (reduced bone density) - TRUE
- c) Cupping of the metaphysis - TRUE (classic "cupped and frayed" metaphysis)
Q29. Radiological features of dislocated DRUJ - which is NOT?
- a) Shortening of radius - can occur with associated fractures
- b) Fractured base of ulna styloid process - common associated injury
- c) Widened DRUJ space on AP view - TRUE (joint disruption widens the space)
Q30. Suggestive of a pathological fracture - which is NOT?
- a) Bone pain and limb swelling PREDATING the fracture (pain before trauma = diseased bone)
- b) Marked post-fracture swelling disproportionate to minor trauma
- c) Cystic abnormality on x-ray (bone cyst, tumour visible before fracture)
Q31. Fracture lines on shaft humerus as indications of ORIF - which is NOT?
- a) Segmental fractures - need rigid fixation
- b) Displaced intra-articular extension - joint surface must be anatomically reduced
- c) Floating elbow (ipsilateral fractures of humerus and forearm) - needs fixation
Q32. External fixation is particularly useful - which is NOT?
- a) Fractures with severe soft-tissue damage - YES (keeps bone aligned without implants in contaminated field)
- b) Open fractures where the wound must be left open - YES
- c) Severely comminuted, unstable fractures - YES (temporizing measure)
Q33. Radiological features of Brodie's abscess - which is NOT?
- a) Central radiolucency with surrounding thick rim of reactive bone sclerosis - TRUE (classic)
- b) Pathognomonic tortuous parallel lucent channels extending toward the growth plate - TRUE
- c) Variable degree of periosteal new-bone formation - TRUE
Q34. Radiological features of osteoarthritis - which is NOT?
- a) Joint space NARROWING - cartilage is eroded (TRUE)
- c) Osteophytes - bone spurs at joint margins (TRUE)
- d) Sclerotic changes on margins (subchondral sclerosis) - (TRUE)
Q35. Radiological features of Rheumatoid Arthritis - which is NOT?
- a) Soft tissue swelling (periarticular, uniform) - TRUE
- b) Juxta-articular osteoporosis (periarticular bone loss around inflamed joints) - TRUE
- d) Widening of joint space early (due to effusion) - TRUE
Q36. True statement regarding growth plate injuries (Salter-Harris)
- Type I: Fracture through the physis (growth plate) only - LOWEST risk of growth arrest
- Type II: Fracture through physis AND metaphysis (most common) - low growth arrest risk
- Type III: Fracture through physis AND epiphysis - INVOLVES THE JOINT SURFACE (TRUE - answer c)
- Type IV: Fracture through all three: metaphysis, physis, epiphysis
- Type V: Crush injury of the physis - HIGHEST risk of growth arrest (not "always evident" on plain films - option d is FALSE)
- a) Type I has HIGH incidence of growth arrest - FALSE (Type I has low risk)
- b) Type II = physis and metaphysis - TRUE (but this is already true!)
- d) Type V always evident on plain films - FALSE (Type V is often invisible initially)
- c) Type III involves joint surface - TRUE
Q37. Fracture remodelling depends on - which is NOT?
- a) Age - younger children remodel better/faster
- c) Proximity to the joint - fractures near joints (close to the physis) remodel best
- d) Orientation to the joint axis - deformity in the plane of joint movement remodels; rotational and angulation perpendicular to the plane of movement does NOT remodel
Questions 38-40 (Radiograph-based)
- The rounded end = Epiphysis
- Growth plate (dark line) = Physeal plate
- Flared region between growth plate and shaft = Metaphysis
- Long shaft = Diaphysis
Q38. What does letter A indicate?
Q39. What does letter C indicate?
Q40. What does letter D indicate?
SECTION B: SHORT ANSWER QUESTIONS
1. ABC's approach to interpreting an X-ray image (5 marks)
- A - Adequacy/Alignment: Is the film well-exposed, correctly positioned? Check patient alignment.
- B - Bone: Examine each bone for fractures, dislocations, density changes, periosteal reaction, lesions.
- C - Cartilage/Joints: Check joint spaces (narrowing, widening), articular surfaces, growth plates in children.
- S - Soft tissues: Swelling, gas, foreign bodies, calcifications in soft tissues. Soft tissue swelling can indicate an occult fracture.
2. Five radiation protection measures (5 marks)
- Justification: Only perform radiation procedures when clinically justified - no unnecessary x-rays.
- Distance: Increase distance from the radiation source (inverse square law - doubling distance reduces dose by 75%).
- Lead shielding: Use lead aprons, thyroid shields, gonad shields for both patients and staff.
- Collimation: Restrict the x-ray beam to the area of clinical interest only.
- Time: Minimize time of exposure (especially for fluoroscopy and staff in radiation areas).
- ALARA principle: As Low As Reasonably Achievable - always optimize technique to minimize dose.
- 10-day rule: Schedule elective pelvic/abdominal x-rays in women of childbearing age within the first 10 days post-menstruation.
3. What a good radiograph should entail (5 marks)
- Correct identification: Patient name, date, side markers (R/L) clearly visible.
- Two views at 90°: At minimum, AP and lateral views of the area.
- Adequate penetration: Neither overexposed (too dark) nor underexposed (too pale) - all structures visible.
- Entire area included: The region of interest plus the joints above and below (in limb trauma).
- No motion blur: Patient kept still - sharp, clear bone and soft tissue outlines.
- Proper positioning: Anatomically correct position so structures are not distorted.
4. Five uses of ultrasound (5 marks)
- Obstetrics: Fetal assessment, gestational age, anomaly screening, placenta location.
- Abdominal/Pelvic organs: Liver, gallbladder (gallstones), kidneys, uterus, ovaries, prostate.
- Musculoskeletal: Tendons, ligaments, muscles, joint effusions, soft tissue masses.
- Vascular: Doppler ultrasound for blood flow assessment (DVT, carotid stenosis, renal artery stenosis).
- Guided procedures: Real-time guidance for biopsies, aspiration of fluid collections, nerve blocks.
- Cardiac (Echocardiography): Heart valves, function, pericardial effusion.
5. Five indications for surgical management of humeral fractures (5 marks)
- Polytrauma/Multiple fractures: Patient has other injuries requiring early mobilization.
- Floating elbow: Ipsilateral fractures of the humerus and forearm bones.
- Pathological fracture: Fracture through tumour or diseased bone.
- Radial nerve palsy that does NOT recover: Explore and fix.
- Segmental fractures: Cannot be controlled with conservative management.
- Intra-articular extension with displacement: Joint surface must be anatomically reduced.
- Open fractures: Require debridement and stabilization.
- Vascular injury requiring repair: Need bone stabilization first.
6. Gustilo-Anderson classification of open fractures (5 marks)
- Type I: Open fracture with wound <1 cm, clean, minimal soft tissue damage. Simple fracture pattern.
- Type II: Open wound 1-10 cm, moderate soft tissue damage. No flaps, devascularization, or periosteal stripping. Adequate soft tissue coverage.
- Type III: High-energy injury. Extensive soft tissue damage. Subdivided:
- IIIA: Adequate soft tissue coverage despite extensive laceration/flaps. High-energy trauma.
- IIIB: Extensive periosteal stripping with massive contamination. Requires local/free flap for coverage.
- IIIC: Any open fracture with arterial injury requiring repair.
7. Salter-Harris classification of growth plate fractures (5 marks)
- Type I (S): Slip through physis only. X-ray often normal or shows widened growth plate. Good prognosis.
- Type II (A): Fracture through physis + metaphysis. Most common type (75%). Triangular metaphyseal fragment (Thurston-Holland sign). Good prognosis.
- Type III (L): Fracture through physis + epiphysis. Involves joint surface. Moderate risk of growth arrest.
- Type IV (T): Fracture through all three: metaphysis + physis + epiphysis. High risk of growth arrest. Requires ORIF.
- Type V (R): Crush injury of physis. Often invisible on initial x-ray. Highest risk of growth arrest.
8. Definitions (1 mark each)
SECTION C: LONG ANSWER
Complications of Fractures
i. Early Complications (10 marks)
- Haemorrhage: Blood loss into fracture haematoma. Femur fracture can lose 1-1.5L; pelvic fractures can be life-threatening with several litres.
- Shock: Hypovolaemic shock from blood loss (especially pelvic, femoral, multiple fractures).
- Fat embolism: Fat globules from bone marrow enter the bloodstream → lungs (ARDS), brain (confusion), skin (petechiae). Occurs 24-72 hours post-injury.
- Damage to adjacent vessels: Sharp bone fragments lacerate or occlude arteries (e.g., popliteal artery in supracondylar fracture, brachial artery in distal humerus fracture).
- Nerve injury: Radial nerve in humeral shaft fractures, axillary nerve in shoulder fractures/dislocations, common peroneal nerve in fibular neck fractures.
- Visceral injury: Pneumothorax from rib fractures; bladder/urethral injury from pelvic fractures; spinal cord injury from vertebral fractures.
- Compartment syndrome: Raised intracompartmental pressure from haematoma/swelling in closed fascial compartments → ischaemia of muscles and nerves. Presents with the 6 Ps: Pain (out of proportion), Pallor, Pulselessness, Paresthesia, Paralysis, Poikilothermia. Emergency fasciotomy required.
- Infection: Especially in open fractures - contamination leads to osteomyelitis. Requires thorough debridement, antibiotics, and fracture stabilization.
ii. Late Complications (10 marks)
- Delayed union: Fracture takes longer than expected to heal but is still progressing. Defined as no radiological evidence of union by the expected time (3-6 months for most long bone diaphyseal fractures).
- Non-union: Complete failure of fracture healing. Types: hypertrophic (abundant callus but no bridging - needs stability) and atrophic (no callus - needs bone graft + fixation). Features on x-ray: sclerotic fracture ends, no callus bridging.
- Malunion: Fracture heals in abnormal position (angulation, rotation, shortening) → deformity and dysfunction.
- Avascular necrosis (AVN): Blood supply disrupted → bone death. Common in femoral head (neck of femur fracture), scaphoid (waist fractures), talus. Shows as increased density (sclerosis) on x-ray.
- Joint stiffness: Prolonged immobilization and fibrous adhesions within and around joints.
- Osteoarthritis: Post-traumatic OA in joints affected by intra-articular fractures with residual step-off deformity.
- Myositis ossificans: Heterotopic bone formation in muscle/soft tissue around the fracture (especially elbow). Visible as calcification on x-ray.
- Volkmann's ischaemic contracture: Late sequela of untreated compartment syndrome → muscle fibrosis and contracture (typically flexion deformity of wrist and fingers after forearm compartment syndrome).
- Reflex sympathetic dystrophy (Complex Regional Pain Syndrome - CRPS): Persistent burning pain, vasomotor changes, bone demineralization (Sudeck's atrophy visible on x-ray).
- Shortening and growth disturbance: In children, physeal damage causes limb length discrepancy or angular deformity.
Search for clinical images of common fracture patterns in radiology
common fracture patterns radiology clinical X-ray images types
Colles fracture Monteggia Galeazzi spiral greenstick comminuted X-ray radiology images site:radiopaedia.org OR site:radiologymasterclass.co.uk
greenstick fracture torus buckle fracture comminuted impacted fracture X-ray clinical image radiology
transverse fracture oblique fracture spiral fracture impacted fracture X-ray images radiology
Common Fracture Patterns in Radiology - Clinical Image Guide
1. Fracture Healing Stages (Overview)

2. Monteggia Fracture-Dislocation

- Ulna fractures at the proximal third
- The radial head always dislocates - if you miss this, treatment fails
- Rule: always check the elbow when you see an ulna fracture
3. Galeazzi Fracture

- Fracture is at the distal radius (opposite end to Monteggia)
- The DRUJ at the wrist is disrupted - check the ulnar styloid and DRUJ space
- Mnemonic: "GAL" = GALeazzi = distal rAdius + wrist joint
4. Colles' Fracture (Smith's fracture for comparison)

- Colles' fracture: distal radius fracture with dorsal (posterior) displacement - "dinner fork deformity" on lateral view
- Smith's fracture: distal radius fracture with volar (anterior/palmar) displacement - "garden spade deformity"
- Both caused by FOOSH (fall on outstretched hand) but at different wrist positions
5. Torus (Buckle) Fracture - Paediatric
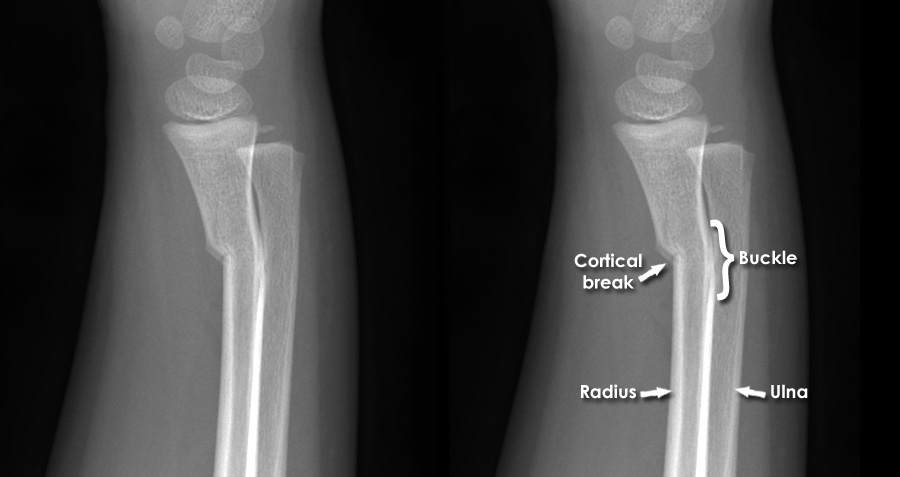
- Only ONE side of the cortex buckles (compressive side)
- The other cortex and periosteum remain intact
- Stable fracture - treated with splint/cast only
- Easily missed! Look carefully at the metaphysis of the distal radius
6. Greenstick Fracture - Paediatric

| Feature | Torus/Buckle | Greenstick |
|---|---|---|
| Cortex | Bulges/buckles, no break | Breaks on tension side |
| Side affected | Compression side | Tension (convex) side |
| Stability | Very stable | Less stable, may angulate |
| Age | Any paediatric | Usually younger children |
7. Spiral Fracture of the Femur

- The fracture line spirals along the bone shaft
- Caused by torsion - a twisting force (e.g., planted foot + body rotation)
- In children under 3 years: raise concern for non-accidental injury
- Contrasted with transverse fracture (direct blow) and oblique fracture
8. Comminuted Fracture of the Tibia (AO Foundation)

- Three or more bone fragments = comminuted
- Results from high-energy trauma
- More complex to fix - often requires intramedullary nail or external fixator
- Associated with greater soft tissue injury
Summary Table: Fracture Pattern Recognition
| Fracture Pattern | X-ray Appearance | Causative Force | Common Location |
|---|---|---|---|
| Transverse | Line perpendicular to bone axis | Direct blow | Tibia, ulna (nightstick) |
| Oblique | Line at an angle (~45°) | Angulation force | Any long bone |
| Spiral | Helical line wrapping the shaft | Torsion/rotation | Tibia, humerus, femur |
| Comminuted | 3+ fragments | High energy | Tibia, femur, radius |
| Impacted | Dense/sclerotic line, bone driven together | Axial compression | Femoral neck, vertebrae |
| Greenstick | Partial cortical break, one side intact | Bending | Paediatric forearm |
| Torus/Buckle | Cortical bulge, no break | Axial load + compression | Paediatric distal radius |
| Segmental | Two fracture lines, floating segment | High energy | Femur, tibia |
| Avulsion | Small fragment pulled from bone | Muscle/ligament pull | Ankle, pelvis, finger |
| Stress | Subtle cortical break or periosteal reaction | Repetitive loading | Metatarsal, tibia |
Search for radiological features of specific bone tumours (osteomyelitis vs Ewing's sarcoma)
osteomyelitis vs Ewing sarcoma radiological features X-ray MRI comparison clinical images
Ewing sarcoma onion skin periosteal reaction X-ray radiograph clinical image radiopaedia
acute osteomyelitis X-ray periosteal reaction bone destruction sequestrum involucrum clinical radiograph
Radiological Features: Osteomyelitis vs. Ewing's Sarcoma
PART 1 - OSTEOMYELITIS
Pathological Basis
X-Ray: Chronic Osteomyelitis - Sequestrum, Involucrum, and Cloaca

- Sequestrum (yellow arrow, right image): dense, sclerotic fragment of dead (avascular) bone separated from living bone. The most specific sign of chronic osteomyelitis.
- Involucrum (white arrow, left image): thick shell of periosteal new bone that forms around the sequestrum as the body attempts to contain the infection.
- Cloaca (red arrow, left image): opening/aperture in the involucrum through which pus drains - may form a sinus tract to the skin.
Radiological Features of Osteomyelitis - Stage by Stage
| Stage | Timing | X-ray Findings | Best Modality |
|---|---|---|---|
| Acute early | Days 1-7 | NORMAL plain x-ray (30-50% bone mineral loss needed before visible) | MRI (changes in 24-48h) |
| Acute late | Week 2 | Soft tissue swelling, subtle bone lysis, periosteal reaction beginning | X-ray + MRI |
| Subacute | Weeks-months | Well-defined lytic lesion ± sclerotic rim (Brodie's abscess) | X-ray + CT |
| Chronic | Months-years | Sequestrum + involucrum + cloaca, cortical thickening, sclerosis | X-ray + CT |
- Soft tissue swelling (earliest sign, days 3-5)
- Periosteal elevation and periosteal new bone formation
- Patchy/moth-eaten bone destruction in the metaphysis
- Lucent areas within bone (pus cavities)
Brodie's Abscess (Subacute/Chronic Osteomyelitis)
- Well-defined central lucency (the abscess cavity)
- Surrounding thick rim of reactive sclerosis
- A characteristic tortuous lucent channel extending toward the growth plate (pathognomonic)
- Variable periosteal new bone formation
PART 2 - EWING'S SARCOMA
Pathological Basis
X-Ray: Classic "Onion-Skin" Periosteal Reaction
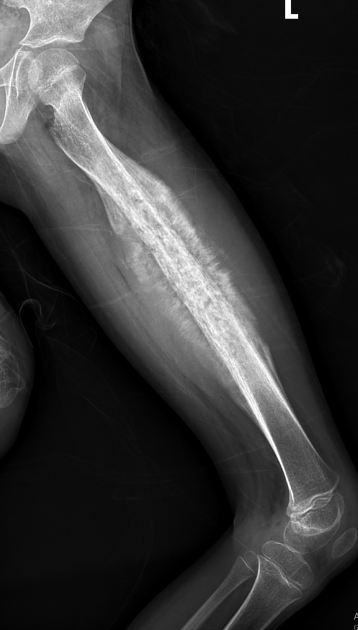
X-Ray: Ewing's Sarcoma - Full Femur View (Permeative Pattern)
X-Ray: Ewing's Sarcoma - Distal Femur

Ewing's Sarcoma with MRI Correlation

PART 3 - DIRECT COMPARISON: The Great Mimic

MASTER COMPARISON TABLE
| Feature | Osteomyelitis | Ewing's Sarcoma |
|---|---|---|
| Age | Any (peak: <5 years, haematogenous) | 5-25 years (peak: 10-15 yrs) |
| Race | Any | Predominantly Caucasian (rare in Black patients) |
| Bone location | Metaphysis (children), diaphysis (adults) | Diaphysis (classic), also metaphysis |
| Bone affected | Tibia, femur most common | Femur, tibia, pelvis, flat bones |
| Pattern of destruction | Focal lytic → moth-eaten | Permeative, moth-eaten, wide zone of transition |
| Periosteal reaction | Solid/layered; less aggressive | Lamellated "onion-skin"; aggressive; Codman triangle |
| Soft tissue mass | Present but typically smaller | LARGE soft tissue mass (>50% of cases) - key differentiator |
| Sequestrum/Involucrum | YES (chronic) - pathognomonic | NOT present |
| Brodie's abscess | YES (subacute form) | NO |
| Zone of transition | Narrow (more organized) | Wide (more aggressive) |
| MRI soft tissue mass | Poorly defined, inflammatory | Well-defined, large, distinct from surrounding tissue |
| Marrow signal on MRI | Diffuse T2 high signal (oedema pattern) | More focal, sharper margins |
| Fever / raised ESR / WBC | YES (infection) | YES (tumour, mimics infection) |
| Treatment | Antibiotics ± surgical drainage | Chemotherapy + radiotherapy ± surgery |
| Key distinguishing sign | Sequestrum (chronic), Brodie's abscess | Large soft tissue mass + sharp transition zone on MRI |