ACS protocol
Reading File
Finding Sources
Searching PubMed
"acute coronary syndrome" AND management
Reading File
Finding Sources
Reading Article
PMID: 40014670
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have enough comprehensive content from multiple authoritative textbooks. Let me compile the full ACS protocol response.
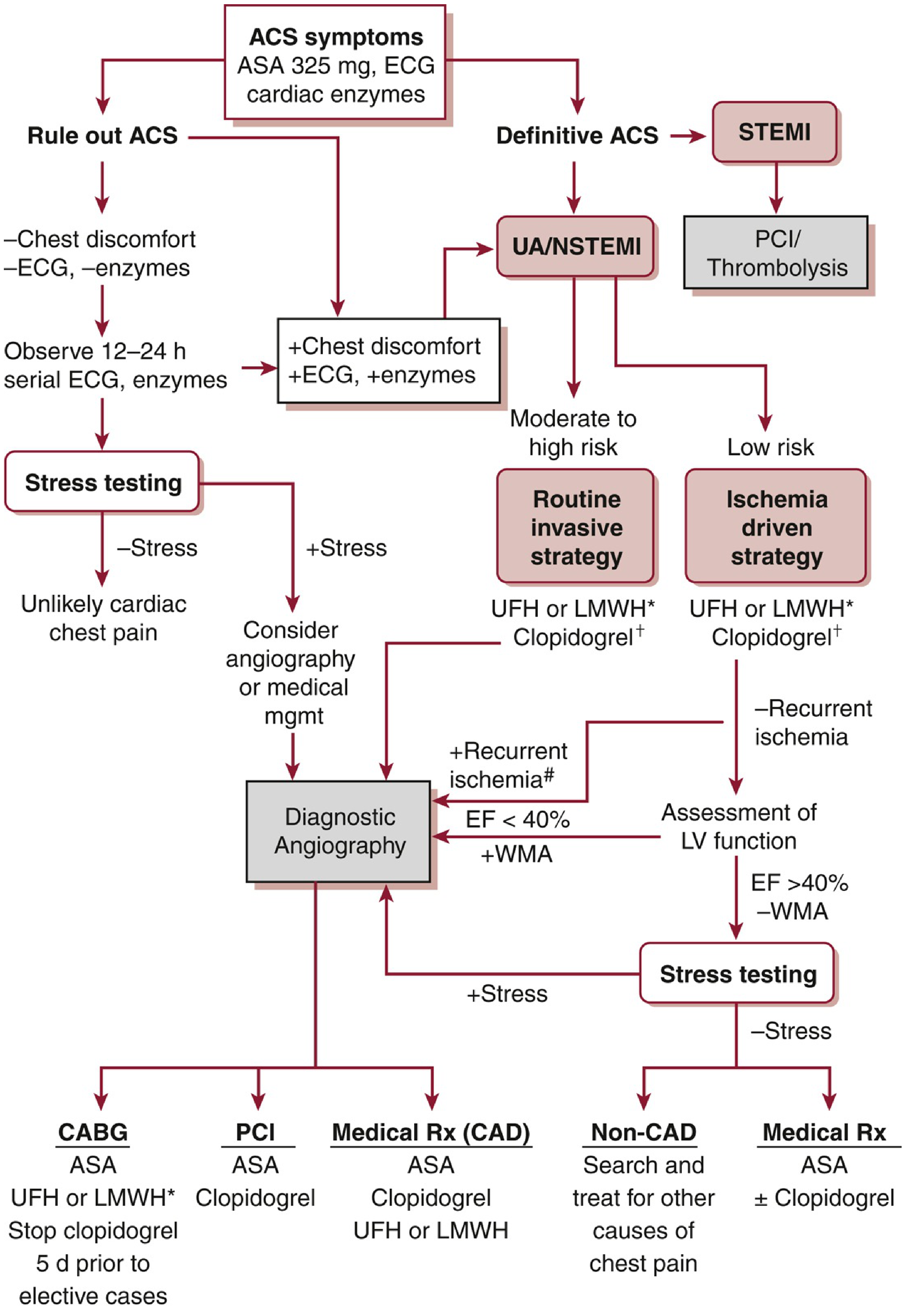
Acute Coronary Syndrome (ACS) Protocol
Overview
ACS is a spectrum of myocardial ischemia/infarction defined by three entities:
| Entity | Troponin | ST Changes | Definition |
|---|---|---|---|
| Unstable Angina (UA) | Negative | No ST elevation | Chest pain at rest/new-onset/crescendo, no necrosis |
| NSTEMI | Positive | ST depression or T-wave changes | Myonecrosis without transmural occlusion |
| STEMI | Positive | Persistent ST elevation >20 min | Complete transmural occlusion; medical emergency |
The key mechanism in type 1 MI: atherosclerotic plaque rupture/erosion → platelet aggregation → thrombus → partial (UA/NSTEMI) or complete (STEMI) coronary occlusion.
Step 1 - Initial Assessment (within 10 minutes of arrival)
History: Classic = chest pain/pressure radiating to arm/jaw, diaphoresis, nausea. Atypical presentations are more common in elderly, women, diabetics, and postoperative patients (dyspnea, confusion, abdominal pain, syncope, unexplained hypotension).
Immediate workup:
- 12-lead ECG within 10 minutes of presentation (first priority)
- Cardiac biomarkers: high-sensitivity troponin (serial at 0, 1, 3 hours)
- CBC, BMP, coagulation studies (aPTT, PT/INR), lipid panel, magnesium
- Portable CXR (assess for pulmonary edema, exclude aortic dissection)
- Continuous cardiac monitoring / telemetry
STEMI ECG criteria (2 or more contiguous leads):
- Men >40 yr: ≥2 mm in V2-V3; ≥1 mm all other leads
- Men <40 yr: ≥2.5 mm in V2-V3
- Women: ≥1.5 mm in V2-V3; ≥1 mm all other leads
- Right-sided leads (V4R): ≥0.5 mm (for RV infarction in inferior STEMI)
- Posterior leads (V7-V9): ≥0.5 mm
ECG-Territory-Artery correlation:
| ST Elevation | Territory | Culprit Artery |
|---|---|---|
| V1-V6 / LBBB | Anterior/septal | Proximal LAD or left main |
| V2-V4 | Anterior wall | LAD |
| V5-V6 | Lateral wall | LCX |
| II, III, aVF | Inferior | RCA or LCX |
| I, aVL | High lateral | Diagonal or proximal LCX |
STEMI mimics to exclude: Pericarditis, LV aneurysm, Brugada syndrome, aortic dissection, LV hypertrophy, early repolarization, Prinzmetal angina, hyperkalemia, PE, myocarditis.
Step 2 - Initial Medical Therapy (All ACS)
ASA: 162-325 mg orally (chewed) or rectally immediately. 325 mg preferred if ASA-naive. Maintenance 81 mg/d after PCI.
Supplemental O2: Only if SpO2 <90%.
Nitroglycerin: 0.4 mg SL q5 min × 3 doses for ongoing chest pain (avoid if hypotension, right ventricular infarction, or PDE5 inhibitor use within 24-48 h).
Beta-blockers (e.g., metoprolol 25 mg PO qid): Reduce O2 demand and arrhythmia risk. Contraindicated in heart failure, hemodynamic instability, advanced AV block, significant bradycardia, or active bronchospasm.
Morphine: Used cautiously for refractory chest pain (note: the 2025 ACC/AHA guideline emphasizes avoiding routine morphine in NSTEMI due to potential slowing of P2Y12 inhibitor absorption).
Step 3 - Antiplatelet and Anticoagulant Therapy
DAPT (Dual Antiplatelet Therapy)
ASA + one P2Y12 inhibitor:
| Agent | Loading Dose | Maintenance | Notes |
|---|---|---|---|
| Clopidogrel | 600 mg (PCI) / 300 mg (lysis) | 75 mg/d | Prodrug; variable response |
| Ticagrelor | 180 mg | 90 mg BID | Mortality benefit vs clopidogrel; reversible; preferred if PCI |
| Prasugrel | 60 mg | 10 mg/d | Avoid if prior stroke/TIA, age ≥75, or weight <60 kg |
| Cangrelor | 30 µg/kg IV bolus | 4 µg/kg/min infusion | IV only; FDA-approved for PCI only |
DAPT duration: 12 months standard for DES; may be shortened if high bleeding risk.
Anticoagulation
| Agent | Dose | Notes |
|---|---|---|
| UFH | 60 units/kg IV bolus (max 4000 units), then 12 units/kg/h | All PCI patients; thrombolysis (except streptokinase) |
| Enoxaparin (LMWH) | 30 mg IV bolus, then 1 mg/kg SC q12h | Age >75: no bolus, 0.75 mg/kg SC q12h |
| Bivalirudin | 0.75 mg/kg bolus, then 1.75 mg/kg/h | Direct thrombin inhibitor; alternative at time of PCI |
| Fondaparinux | 2.5 mg IV, then 2.5 mg SC daily | Superior to UFH with thrombolytics; NOT for PCI alone (catheter thrombosis risk) |
Step 4 - Reperfusion Strategy
This is the cornerstone of STEMI management. Mortality is directly proportional to total ischemia time.
STEMI: Reperfusion
Primary PCI is the preferred strategy:
- Door-to-balloon (D2B) time goal: ≤90 minutes (if first medical contact at PCI-capable center)
- FMC-to-device time: ≤120 minutes (if transfer required)
- If transfer expected to delay >120 min from FMC: thrombolytics within 30 minutes (door-to-needle ≤30 min), then transfer for angiography (pharmacoinvasive strategy)
Thrombolytics (if PCI not available within time window):
- Alteplase (tPA), reteplase, tenecteplase (fibrin-specific agents preferred)
- Absolute contraindications: Prior intracranial hemorrhage, ischemic stroke <3 months, active internal bleeding, aortic dissection, known intracranial neoplasm
STEMI Alert should be activated prehospital or in ED - catheterization lab team mobilized analogously to trauma alert.
UA/NSTEMI: Invasive vs. Conservative Strategy
Risk stratify using TIMI risk score (0-7 points):
- Age ≥65 years
- ≥3 CAD risk factors
- Known CAD (stenosis ≥50%)
- ST-segment deviation on admission ECG
- ≥2 anginal events in prior 24 hours
- ASA use in prior 7 days
- Elevated cardiac markers
Higher TIMI score = higher 14-day risk of death/MI/urgent revascularization → prefer routine invasive strategy.
| Strategy | Timing | Indications |
|---|---|---|
| Immediate invasive (<2h) | <2 hours | Refractory ischemia, hemodynamic instability, sustained VT/VF, heart failure |
| Early invasive (<24h) | <24 hours | GRACE score >140, troponin rise/fall, new ST depression |
| Delayed invasive (24-72h) | 24-72 hours | Stabilized moderate-to-high risk |
| Ischemia-driven (conservative) | Selective | Low TIMI score, EF >40%, no recurrent ischemia |
Step 5 - Secondary Prevention (Discharge Medications)
| Drug Class | Agent | Goal |
|---|---|---|
| Antiplatelet | ASA 81 mg/d indefinitely + P2Y12 for 12 months | Reduce stent thrombosis / recurrent MI |
| Statin | High-intensity (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) | LDL <55 mg/dL ideally |
| Beta-blocker | Metoprolol succinate or carvedilol | Reduce mortality, especially if EF reduced |
| ACE inhibitor / ARB | Ramipril, lisinopril, or equivalent | If EF ≤40%, diabetes, hypertension, CKD |
| Aldosterone antagonist | Eplerenone / spironolactone | If EF ≤40% + HF symptoms or diabetes |
Special Populations
Elderly (>75 years): Higher atypical presentations; AHA guidelines support revascularization with no absolute age cutoff; higher bleeding risk - adjust LMWH dosing (no IV loading dose in enoxaparin).
RV Infarction (complicating inferior STEMI): Hypotension + clear lungs + JVD triad; avoid nitrates, diuretics; treat with IV fluids and maintain RV preload.
Cardiogenic Shock: Early revascularization; consider mechanical circulatory support (IABP, Impella, ECMO). Inotropes (dobutamine) if needed.
Key Time Targets (2025 ACC/AHA Guideline)
| Metric | Target |
|---|---|
| First ECG after ED arrival | ≤10 minutes |
| Door-to-balloon (PCI center) | ≤90 minutes |
| FMC-to-device (transfer) | ≤120 minutes |
| Door-to-needle (thrombolytics) | ≤30 minutes |
Sources
- The Washington Manual of Medical Therapeutics (ACS protocol, Tables 4-14, 4-17, Figures 4-3 & 4-4)
- Goldman-Cecil Medicine International Edition (Chapters 57-58, NSTEMI/STEMI management)
- Rosen's Emergency Medicine (Chapter 64, ECG adjuncts, ACS management)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (ACS pharmacology)
- 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for Management of ACS (Rao SV et al., Circulation, 2025) - [PMID 40014670] - Note: An erratum was published (PMID: 41212941); verify specific recommendations against the corrected version.
This is a shared conversation. Sign in to Orris to start your own chat.