Explain me 10 common heart disease with ECG changes , & ECG image
Reading File
Finding Sources
Searching Images
ECG changes in myocardial infarction ST elevation
Searching Images
atrial fibrillation ECG electrocardiogram
Searching Images
heart block complete AV block ECG third degree
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
left bundle branch block LBBB ECG electrocardiogram
Finding Sources
Searching Images
Wolff-Parkinson-White WPW syndrome ECG delta wave
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
pericarditis ECG saddle-shaped ST elevation diffuse
Searching Images
hyperkalemia ECG peaked T waves wide QRS sine wave
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy
I now have excellent ECG images for all 10 conditions. Let me compile the comprehensive response.
10 Common Heart Diseases with ECG Changes
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery → transmural ischemia → necrosis of full myocardial thickness.
ECG Changes:
- Hyperacute T waves — earliest change; tall, broad, peaked T waves
- ST-segment elevation ≥ 1 mm in ≥ 2 contiguous limb leads or ≥ 2 mm in precordial leads (convex "tombstone" shape)
- Reciprocal ST depression in opposite leads
- Pathological Q waves (>40 ms wide, >25% QRS height) — evolve over hours/days
- T-wave inversion follows in the recovery phase
Territory localization:
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Anterior | V1–V4 | LAD (proximal) |
| Anterolateral | V1–V6, I, aVL | LAD |
| Inferior | II, III, aVF | RCA or LCx |
| Posterior | V1–V3 (depression + tall R) | LCx or RCA |
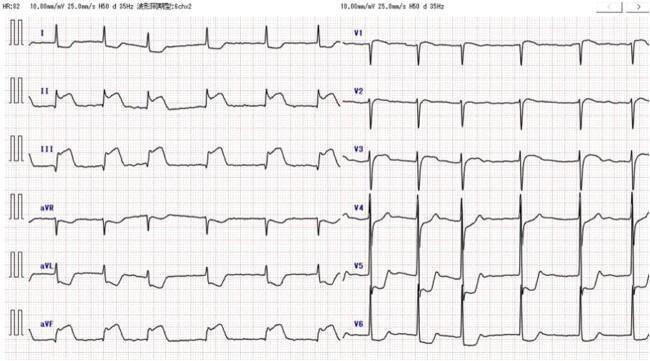
ECG — Anterolateral STEMI:

ECG — Inferior STEMI:
2. 🫀 Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized atrial electrical activity from multiple re-entrant wavelets → loss of coordinated atrial contraction → irregular ventricular response.
ECG Changes:
- Absent P waves — replaced by irregular fibrillatory (f) waves, best seen in V1
- Irregularly irregular R-R intervals (hallmark finding)
- Narrow QRS (unless aberrant conduction/BBB)
- Ventricular rate varies (bradycardic if controlled, tachycardic if uncontrolled)
- Baseline shows fine, chaotic oscillations (350–600 impulses/min from atria)
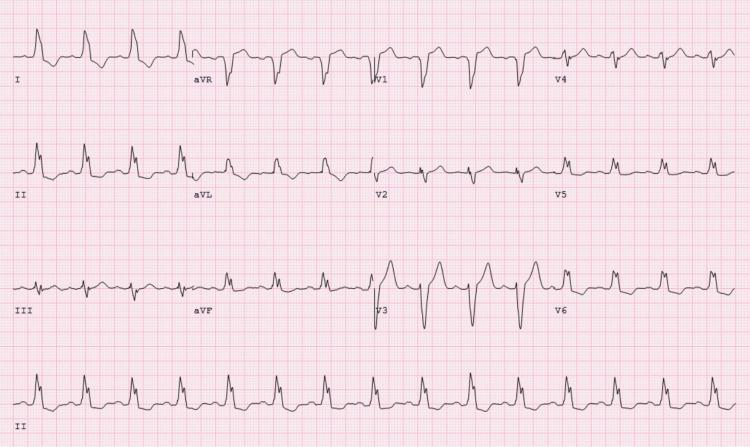
ECG — Atrial Fibrillation with rapid ventricular response:

3. 🫀 Complete (Third-Degree) AV Block
Pathophysiology: Complete failure of conduction through the AV node or His-Purkinje system → total dissociation between atrial and ventricular activity.
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes march independently
- Regular P-P intervals (atrial rate, typically 60–100 bpm)
- Regular R-R intervals (slow escape rhythm, typically 20–45 bpm)
- No constant PR interval — P waves can fall before, within, or after QRS
- Wide QRS if escape is ventricular (>120 ms); narrow QRS if junctional escape
- Requires urgent pacemaker implantation
ECG — Complete Third-Degree AV Block:

4. 🫀 Ventricular Tachycardia (VT)
Pathophysiology: Three or more consecutive ventricular ectopic beats at ≥100 bpm, arising below the His bundle. Most commonly occurs in structural heart disease (post-MI scar, dilated cardiomyopathy).
ECG Changes:
- Wide complex tachycardia (QRS ≥120 ms), rate 100–250 bpm
- Regular or slightly irregular rhythm
- AV dissociation (P waves independent of QRS) — pathognomonic when seen
- Fusion beats and capture beats (Dressler beats) — diagnostic
- Concordance — all precordial leads positive (positive concordance) or negative (negative concordance)
- Extreme axis deviation ("northwest" axis, −90° to ±180°)
- Brugada criteria and Vereckei criteria used to differentiate from SVT with aberrancy
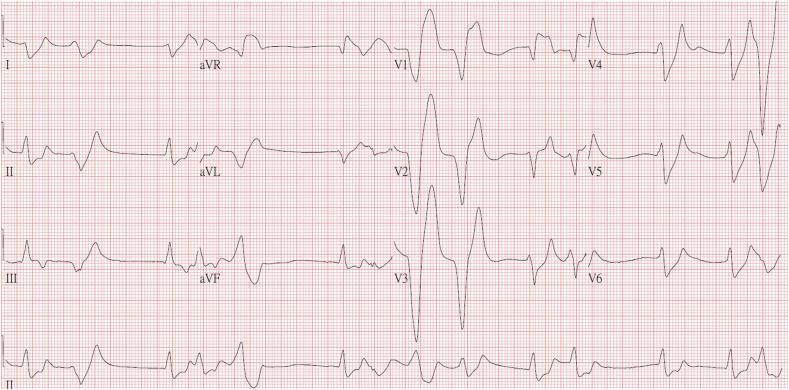
ECG — Ventricular Tachycardia (monomorphic wide complex):

5. 🫀 Left Bundle Branch Block (LBBB)
Pathophysiology: Failure of conduction through the left bundle branch → delayed depolarization of left ventricle → abnormal ventricular activation sequence. Can be caused by hypertension, CAD, cardiomyopathy, or acute MI (new LBBB = STEMI equivalent).
ECG Changes (WILLIAM mnemonic — W in V1, M in V6):
- QRS duration ≥120 ms
- Broad, notched (M-shaped) R waves in lateral leads (I, aVL, V5, V6)
- Deep, broad S waves or QS pattern in right precordial leads (V1, V2)
- No septal Q waves in I, V5, V6
- Discordant ST/T changes (ST and T in opposite direction to main QRS deflection — secondary repolarization change)
- Left axis deviation common
ECG — Left Bundle Branch Block:
6. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: Accessory pathway (Bundle of Kent) bypasses the AV node → pre-excitation of the ventricle before normal AV node conduction arrives → fusion QRS complex. At risk of rapid AF conducting via the accessory pathway → life-threatening.
ECG Changes (classic triad):
- Short PR interval (<120 ms) — bypass of AV nodal delay
- Delta wave — slurred upstroke at start of QRS (pre-excitation of ventricle)
- Wide QRS (>120 ms) — fusion of pre-excited and normally conducted activation
- Secondary ST/T changes discordant to delta wave
- Accessory pathway localization possible by delta wave polarity (negative delta in inferior leads → posteroseptal pathway; positive V1 → left-sided pathway)
ECG — Wolff-Parkinson-White Syndrome:

7. 🫀 Pulmonary Embolism (PE)
Pathophysiology: Acute obstruction of pulmonary vasculature → sudden increase in right ventricular afterload → acute RV strain and dilation → leftward septal shift, impaired LV filling.
ECG Changes:
- Sinus tachycardia — most common finding
- S1Q3T3 pattern (McGinn-White sign) — S wave in lead I + Q wave in lead III + inverted T wave in lead III
- Right axis deviation
- Incomplete or complete RBBB — due to RV strain
- T-wave inversions in V1–V4 — reflects right ventricular strain pattern
- P pulmonale (tall P in II >2.5 mm) — right atrial enlargement
- Atrial fibrillation may occur
- Normal ECG does NOT exclude PE
ECG — Pulmonary Embolism (S1Q3T3 pattern, annotated):

8. 🫀 Acute Pericarditis
Pathophysiology: Inflammation of the pericardium → diffuse superficial myocardial injury → characteristic widespread repolarization and depolarization changes distinct from MI.
ECG Changes (4 classic stages):
| Stage | Timing | ECG Change |
|---|---|---|
| I | Hours–days | Diffuse concave ("saddle-shaped") ST elevation + PR depression |
| II | Days–weeks | ST normalizes, PR still depressed |
| III | Weeks | Diffuse T-wave inversions |
| IV | Months | ECG normalizes |
- PR segment depression in most leads (II, V2–V6) — highly specific; aVR shows reciprocal PR elevation
- Diffuse ST elevation — concave upward, not confined to one coronary territory
- No reciprocal ST depression (except aVR and V1)
- Spodick's sign — downsloping TP segment
- No pathological Q waves (differentiates from MI)
ECG — Acute Pericarditis:

9. 🫀 Hyperkalemia
Pathophysiology: Elevated serum K⁺ → reduces resting membrane potential → slows conduction, impairs repolarization → progressive ECG changes correlating with serum K⁺ level, potentially fatal.
ECG Changes (progressive with rising K⁺):
| Serum K⁺ | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Peaked (tented) T waves — tall, narrow-based, most in V2–V4 |
| 6.5–7.5 mEq/L | PR prolongation, P wave flattening/disappearance |
| 7.0–8.0 mEq/L | QRS widening (intraventricular conduction delay) |
| >8.0–9.0 mEq/L | Sine-wave pattern — QRS merges with T waves |
| >9.0 mEq/L | Ventricular fibrillation / asystole |
ECG — Severe Hyperkalemia:
10. 🫀 Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Genetic (sarcomeric protein mutations) → asymmetric left ventricular hypertrophy (most commonly the interventricular septum) → increased QRS voltage, abnormal repolarization, myofiber disarray → arrhythmia risk and sudden cardiac death.
ECG Changes:
- LVH voltage criteria — Sokolow-Lyon: SV1 + RV5/V6 ≥35 mm; Cornell criteria >28 mm men / >20 mm women
- Deep, "giant" T-wave inversions in V2–V6 — especially in apical HCM (Yamaguchi syndrome); T waves can be >10 mm deep
- Deep, narrow Q waves in inferior (II, III, aVF) and lateral leads (V4–V6, I, aVL) — from septal hypertrophy
- Abnormal septal Q waves absent in I, V5, V6 (opposite of normal)
- ST-segment depression with lateral strain pattern
- Prolonged QTc in some variants
- Left axis deviation
- Increased risk of VT/VF → sudden cardiac death in young athletes
ECG — Hypertrophic Cardiomyopathy (HCM):
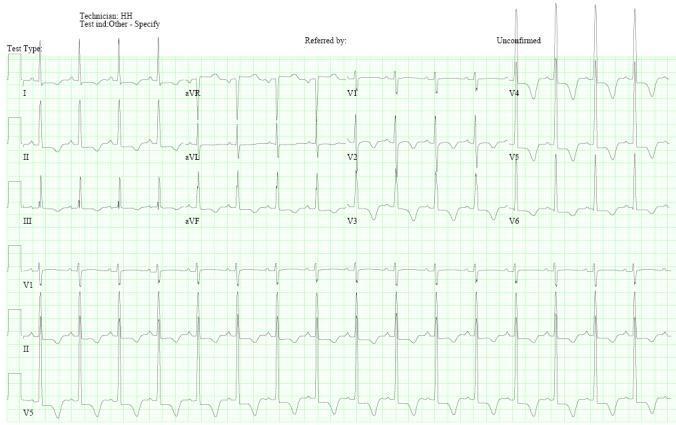
HCM ECG variants compared (concentric, septal, apical):
Quick Reference Summary
| # | Condition | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation (convex) in contiguous leads + reciprocal changes + Q waves |
| 2 | Atrial Fibrillation | No P waves + irregularly irregular rhythm |
| 3 | 3rd-Degree AV Block | Complete AV dissociation + slow escape rhythm |
| 4 | Ventricular Tachycardia | Wide complex tachycardia + AV dissociation + fusion beats |
| 5 | LBBB | QRS ≥120 ms + WiLLiaM pattern + discordant ST/T |
| 6 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 7 | Pulmonary Embolism | Sinus tachycardia + S1Q3T3 + RV strain (TWI V1–V4) |
| 8 | Acute Pericarditis | Diffuse saddle-shaped ST elevation + PR depression (no reciprocals) |
| 9 | Hyperkalemia | Peaked T waves → wide QRS → sine wave → VF |
| 10 | HCM | LVH voltage + giant T inversions V2–V6 + deep narrow Q waves |
Clinical Pearl: Always interpret ECGs in the clinical context. A single ECG can be normal even in serious disease (e.g., early STEMI, PE), and pathological findings (e.g., LBBB, LVH) require clinical correlation to guide management.
This is a shared conversation. Sign in to Orris to start your own chat.