Hyperparathyroidism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hyperparathyroidism"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content to write a full, well-structured answer. Here it is:
Hyperparathyroidism
Classification
Hyperparathyroidism is classified into three types based on the underlying mechanism:
| Type | Mechanism | Calcium | PTH |
|---|---|---|---|
| Primary | Autonomous PTH overproduction (adenoma/hyperplasia) | High | High or inappropriately normal |
| Secondary | Compensatory PTH hypersecretion in response to hypocalcemia | Low/normal | High |
| Tertiary | Autonomous PTH production arising from long-standing secondary hyperparathyroidism | High | High |
A normocalcemic variant of primary hyperparathyroidism also exists - normal serum calcium with persistently elevated intact PTH on at least two occasions over 3-6 months, in the absence of secondary causes. Its prevalence is <0.2% among those assessed for bone mineral density.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1010
- Goldman-Cecil Medicine, p. 2642
Primary Hyperparathyroidism
Epidemiology
- One of the most common endocrine disorders; affects ~3 in 1000 adults
- Estimated annual incidence of ~25 cases per 100,000 in the US and Europe
- More common in females than males (~4:1)
- Peak incidence in the 50s and older
- ~80% are identified incidentally via routine serum electrolyte panels
Causes
| Lesion | Frequency |
|---|---|
| Solitary parathyroid adenoma | 85-95% |
| Primary hyperplasia (diffuse or nodular) | 5-10% |
| Parathyroid carcinoma | ~1% |
Molecular pathogenesis of sporadic adenomas:
- Cyclin D1 (CCND1) inversions: A pericentromeric inversion on chromosome 11 repositions CCND1 adjacent to the PTH gene, causing PTH regulatory elements to drive cyclin D1 overexpression - promoting cell proliferation. Even without gene inversion, cyclin D1 is overexpressed in up to 40% of adenomas.
- MEN1 mutations: Loss-of-function mutations in the MEN1 tumor suppressor gene.
- CDC73 mutations: Encode parafibromin; mutated in ~70% of sporadic parathyroid carcinomas.
Familial syndromes (~10% of cases): MEN-1, MEN-2, MEN-4, and hyperparathyroidism-jaw tumor (HPT-JT) syndrome (germline CDC73 mutations, includes parathyroid carcinomas + ossifying jaw tumors).
Note: Familial hypocalciuric hypercalcemia (FHH) can mimic primary hyperparathyroidism - it is caused by heterozygous loss-of-function mutations in the calcium-sensing receptor (CASR), resulting in elevated calcium with nonsuppressed PTH, but without the downstream end-organ effects.
Morphology
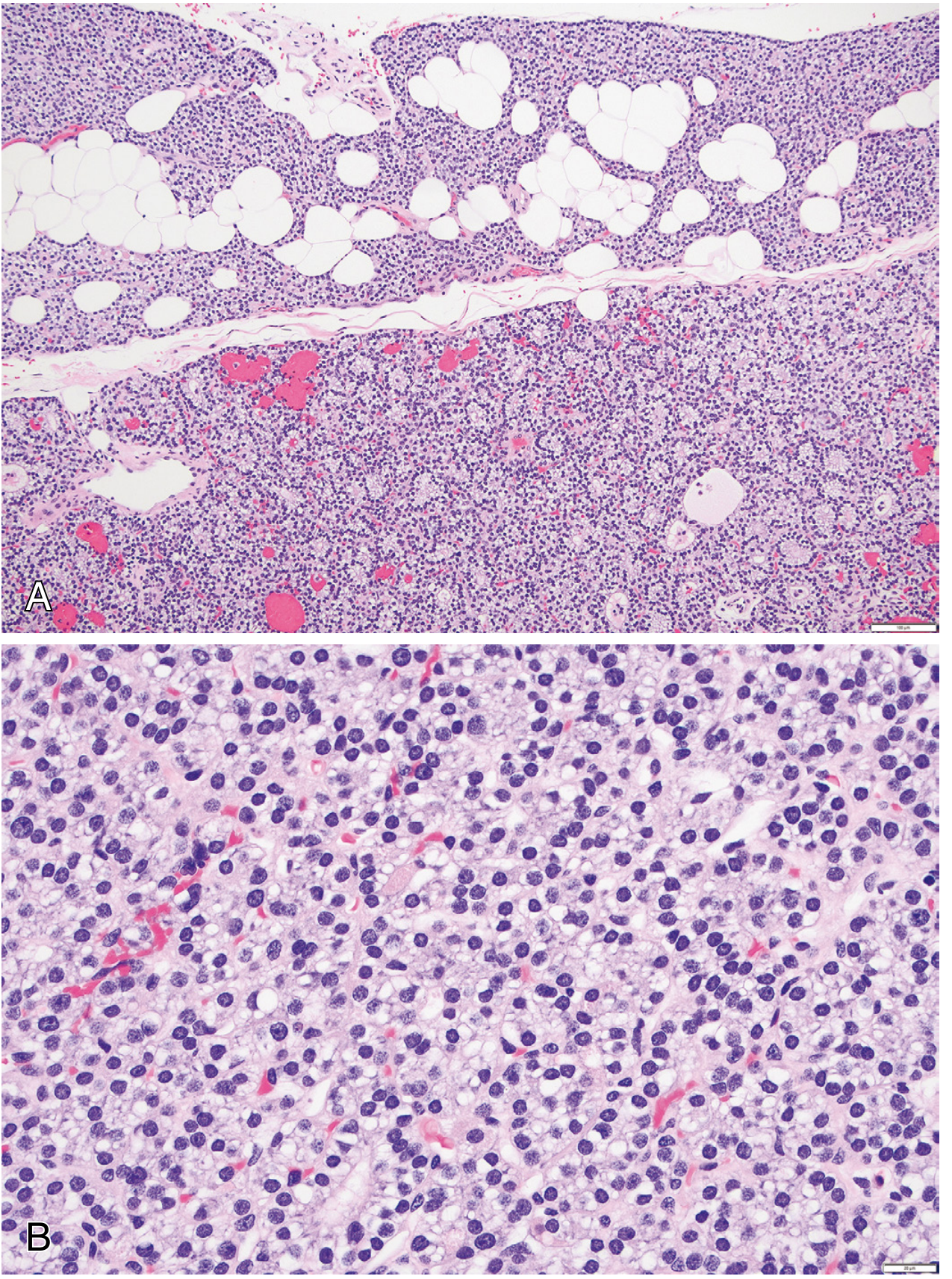
Parathyroid Adenoma
- Almost always solitary; 0.5-5 g; soft, tan-to-reddish-brown, well-circumscribed
- Non-neoplastic glands are normal or shrunken (feedback inhibition from hypercalcemia)
- Microscopy: sheets of uniform polygonal chief cells with small central nuclei; sparse adipose tissue; a rim of compressed normal tissue at the edge
- Bizarre/pleomorphic nuclei (endocrine atypia) may be present but are not a criterion for malignancy
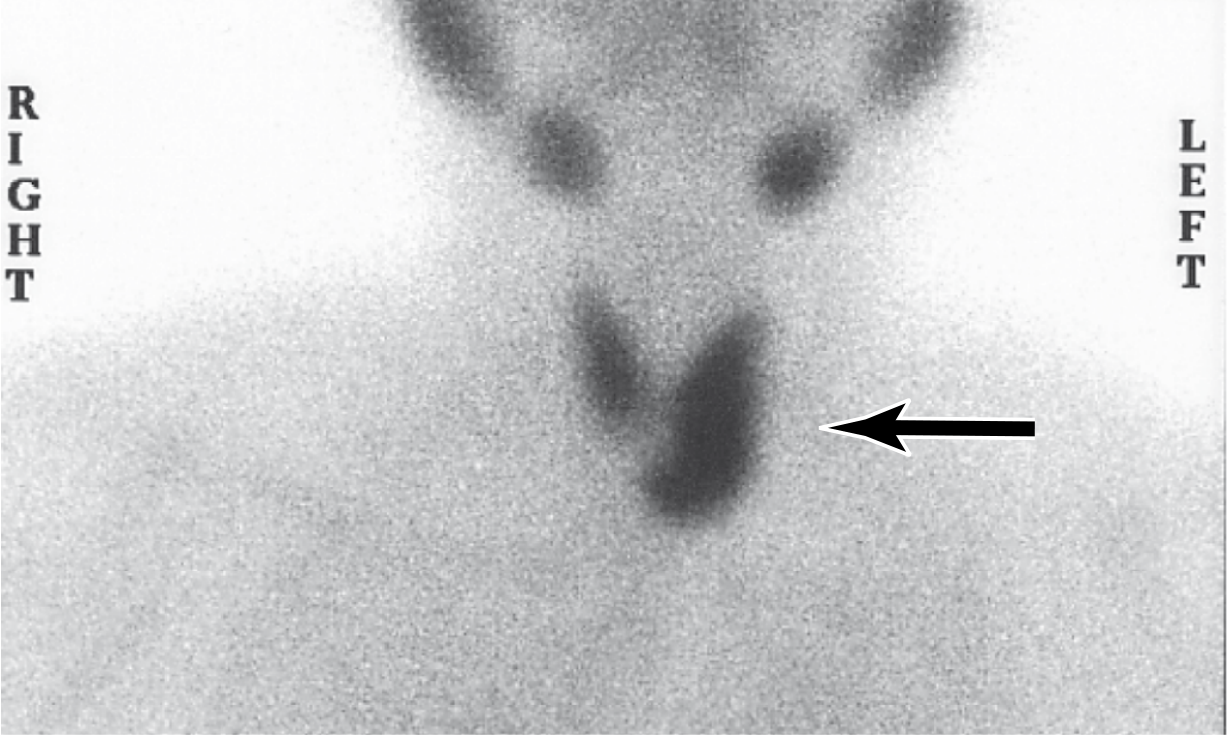
Sestamibi Scan Imaging
Tc-99m sestamibi radionuclide scanning is useful preoperatively to localize adenomas vs. hyperplasia (hyperplasia shows uptake in >1 gland):
Parathyroid Hyperplasia
- Classically all four glands involved, but asymmetry is common - making distinction from adenoma difficult
- Combined weight rarely exceeds 1 g
- Microscopy: chief cell hyperplasia (diffuse or multinodular); less commonly water-clear cell hyperplasia; stromal fat is inconspicuous
Parathyroid Carcinoma
- Defined by invasive growth and/or metastasis (cytology alone is unreliable)
- Gray-white irregular masses, sometimes >10 g
- Local recurrence in ~1/3; more distant dissemination in another third
Pathophysiology
PTH acts on bone, kidney, and intestine (indirectly):
- Bone: increases osteoclastic resorption → releases Ca²+ into blood
- Kidney: increases Ca²+ reabsorption, decreases phosphate reabsorption (phosphaturia), stimulates 1α-hydroxylase → activates vitamin D (1,25-dihydroxycholecalciferol)
- Intestine: indirectly increases Ca²+ absorption via activated vitamin D
Laboratory consequences:
- Hypercalcemia
- Hypophosphatemia (phosphaturia)
- Elevated urine Ca²+, phosphate, and cAMP
Why hypercalciuria despite PTH promoting Ca²+ reabsorption? The filtered calcium load is so high that it overwhelms tubular reabsorptive capacity, so excess Ca²+ spills into urine - hence nephrolithiasis.
- Costanzo Physiology 7th Edition, p. 383
Clinical Features
Classic Mnemonic: "Bones, Stones, Abdominal Groans, and Psychic Moans"
Today, most patients (>80%) are asymptomatic - discovered incidentally on routine blood work. Classic end-organ disease (osteitis fibrosa cystica, brown tumors, nephrocalcinosis) is now infrequent.
Bone disease:
- Decreased bone mineral density (especially cortical bone - distal 1/3 radius)
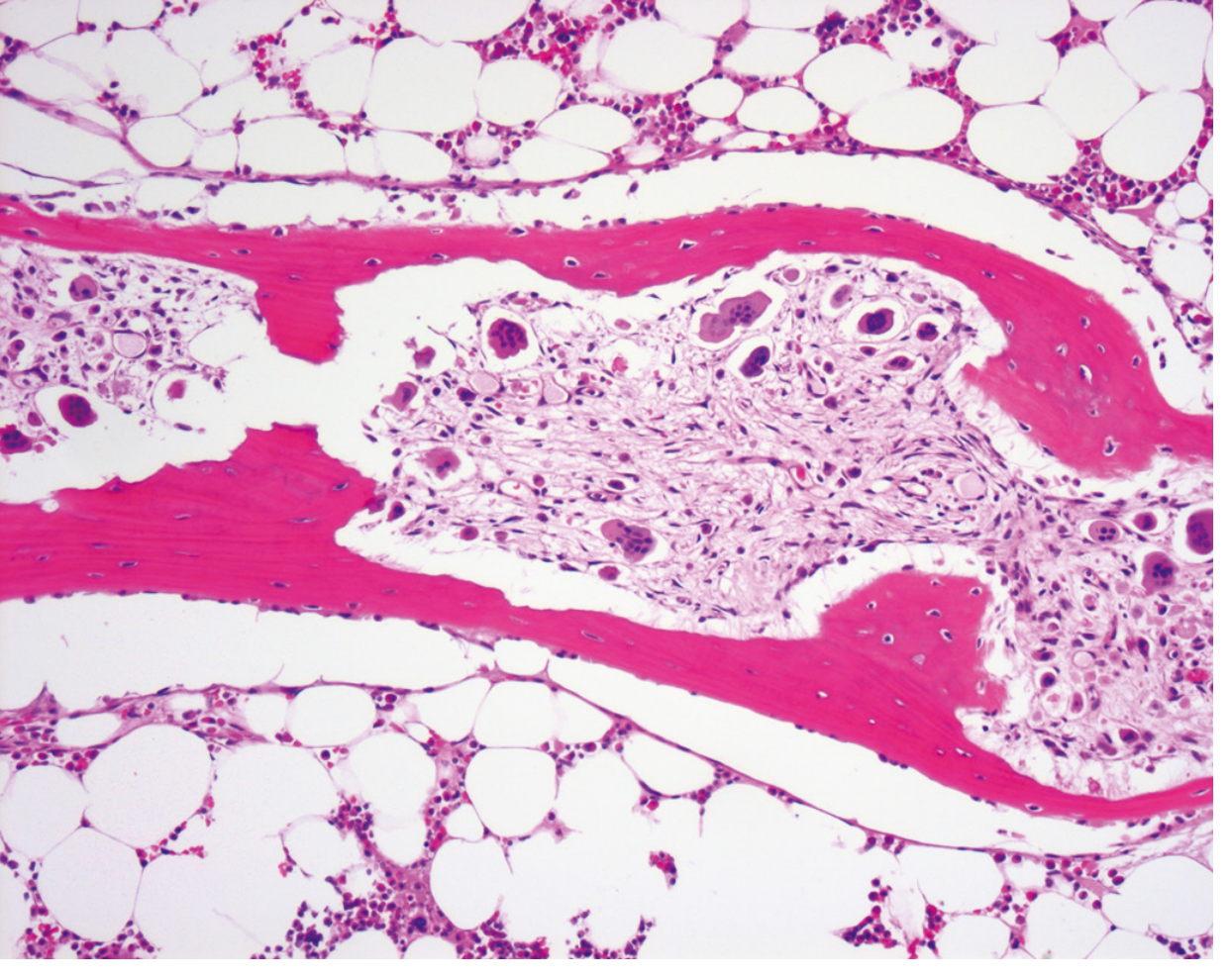
- Osteitis fibrosa cystica (severe cases): generalized osteitis with fibrous replacement of marrow
- Brown tumors (focal collections of osteoclasts, reactive giant cells, and hemorrhagic debris - appear brown due to hemosiderin)
- Subperiosteal bone resorption - classically on radial aspect of middle phalanges
- "Salt and pepper" skull on X-ray
Renal disease (stones):
- Nephrolithiasis (Ca²+-phosphate or Ca²+-oxalate)
- Nephrocalcinosis
- Polyuria and polydipsia (hypercalcemia impairs renal concentrating ability)
- Reduced creatinine clearance
Gastrointestinal (groans):
- Constipation, nausea, vomiting, anorexia
- Peptic ulcer disease (hypercalcemia stimulates gastrin)
- Acute pancreatitis
Neuromuscular/psychiatric (moans):
- Fatigue, weakness (proximal myopathy)
- Depression, anxiety, cognitive impairment, psychosis
- Hypercalcemic crisis (Ca²+ >14 mg/dL): confusion, coma
Laboratory Diagnosis
- Serum Ca²+: elevated (or inappropriately normal for PTH level)
- Intact PTH (iPTH): elevated or inappropriately normal
- Serum phosphate: low
- Urinary Ca²+ (24-hr): elevated
- 25-OH Vitamin D: often low (must check before labeling secondary HPT)
- Alkaline phosphatase: elevated if bone disease present
- PTH vs. PTHrP: essential to distinguish primary HPT from malignancy-related hypercalcemia (PTH is suppressed in malignancy; PTHrP is elevated)
Secondary Hyperparathyroidism
Causes: Chronic renal failure (most common), vitamin D deficiency, malabsorption
Mechanism (using CKD as example):
- Reduced renal 1α-hydroxylase → less activated vitamin D → decreased intestinal Ca²+ absorption
- Phosphate retention (reduced renal excretion) → drives down ionized Ca²+
- Both factors → hypocalcemia → stimulates PTH secretion
- PTH tries to restore Ca²+; results in bone resorption = renal osteodystrophy
Laboratory pattern: High PTH, low/normal Ca²+, high phosphate (in CKD)
Clinical features are dominated by the underlying cause. Bony changes (renal osteodystrophy) are managed by controlling the hyperparathyroidism.
Tertiary Hyperparathyroidism
Develops after prolonged secondary hyperparathyroidism (usually in dialysis patients) when the parathyroid glands become autonomous and continue secreting excess PTH even after correction of hypocalcemia. Results in hypercalcemia. Often requires parathyroidectomy.
Management of Primary Hyperparathyroidism
Indications for Parathyroidectomy (2022 Guidelines)
Surgery is recommended if the patient meets any one of:
- Any complication of primary HPT (nephrolithiasis, nephrocalcinosis, osteitis fibrosa cystica)
- Episode of life-threatening hypercalcemia
- Serum Ca²+ >1 mg/dL above the upper limit of normal
- Marked hypercalciuria (>400 mg/24hr in men; >300 mg/24hr in women) + increased nephrolithiasis risk by stone risk analysis
- Creatinine clearance <60 mL/min
- T-score below -2.5 at any site (lumbar spine, total hip, femoral neck, distal 1/3 radius) and/or prior vertebral fracture
- Age <50 years
- Surgery is also indicated when surveillance is not possible or desired
Adapted from Bilezikian et al., 2022 guidelines in J Bone Miner Res - as cited in Goldman-Cecil Medicine
Watchful Waiting (Asymptomatic Patients)
Only ~25% of asymptomatic patients show progressive disease (as bone mineral density loss) over 10 years. Annual monitoring should include:
- Serum Ca²+, PTH, 25-OH-D
- Creatinine clearance (formal, not eGFR)
- 24-hr urinary calcium
- Bone mineral density (DXA)
- Renal imaging if nephrolithiasis suspected
- Correct vitamin D deficiency cautiously (target 25-OH-D >50 nmol/L)
- Avoid thiazide diuretics, excess calcium intake, dehydration
Medical Therapy
| Drug | Effect | Note |
|---|---|---|
| Cinacalcet (calcimimetic) | Lowers serum Ca²+; modest PTH reduction | Approved for primary HPT if surgery contraindicated; also for dialysis patients with uncontrolled secondary HPT; or parathyroid carcinoma. Does NOT improve BMD alone. Dose: 30 mg twice daily up to 90 mg four times daily. |
| Alendronate (bisphosphonate) | Improves BMD at lumbar spine | Does not alter serum Ca²+ or PTH |
| Cinacalcet + Alendronate combined | Normalizes hypercalcemia AND improves BMD | Best of both |
| Denosumab (RANKL inhibitor) | Improves BMD | 60 mg SC every 6 months; alternative in osteoporotic patients |
| Estrogen (postmenopausal women) | Increases bone density | Only when other agents are contraindicated/unavailable |
- Goldman-Cecil Medicine, p. 2643-2644
Summary Table
| Feature | Primary HPT | Secondary HPT | Tertiary HPT |
|---|---|---|---|
| Cause | Adenoma/hyperplasia/carcinoma | CKD/Vit D def. | Long-standing secondary HPT |
| Ca²+ | High | Low/normal | High |
| PTH | High | High | High (autonomous) |
| Phosphate | Low | High (CKD) | Variable |
| Treatment | Parathyroidectomy/medical | Treat underlying cause, phosphate binders, activated Vit D, cinacalcet | Parathyroidectomy |
This is a shared conversation. Sign in to Orris to start your own chat.