Patient presented with bilateral Lower limb weakness no respiratory difficulty no fever no features of UTI but history of RTA 4days back no history of trauma to back. Now suddenly patient is unresponsive unable to speak weakness preogressed lower limb reflexes exaggerated however vitals are stable
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
vertebral artery dissection RTA cervical spine delayed neurological deterioration
Reading File
Reading File
Finding Sources
Searching PubMed
vertebral artery dissection blunt trauma delayed stroke
Loading Image
Reading File
Finding Sources
Finding Sources
I now have comprehensive information to deliver a thorough clinical analysis. Let me compile this into a structured response.
Clinical Analysis: Post-RTA Bilateral Lower Limb Weakness with Sudden Neurological Deterioration
Synthesizing the Clinical Picture
This is a neurological emergency with a classic evolution pattern. The timeline is critical:
- RTA 4 days ago → bilateral LL weakness with hyperreflexia (UMN pattern) → sudden unresponsiveness + inability to speak
- Vitals stable, no fever, no UTI, no direct back trauma
Most Likely Diagnosis: Vertebral Artery Dissection (VAD) → Basilar Artery Thrombosis / Posterior Circulation Stroke
This fits the entire clinical timeline with remarkable precision.
Why VAD?
Tintinalli's Emergency Medicine states:
"A history of neck trauma in the days to weeks prior to presentation is a prominent risk factor... The stroke may follow the dissection by days or weeks."
Adams & Victor's Neurology adds:
"The dissection most commonly originates at the C1-C2 segment... Symptoms have fluctuated over minutes and hours. The stroke may follow the dissection by days or weeks, obscuring the relationship."
The initial bilateral LL weakness with hyperreflexia could reflect:
- Cervical spinal cord ischemia — anterior spinal artery compromise from VAD causing an ascending myelopathy pattern
- OR an early posterior circulation TIA/ischemia preceding full basilar occlusion
The sudden unresponsiveness + inability to speak = basilar artery thrombosis (propagation of clot from the dissected vertebral artery into the basilar artery), causing:
- Loss of consciousness (reticular activating system involvement)
- Dysarthria/inability to speak (corticobulbar tracts, cranial nerve nuclei in the pons)
- Preserved vitals (early — cardiac and respiratory centers not yet fully compromised)
Differential Diagnoses (ranked by probability)
| Dx | Key Features Supporting | Against |
|---|---|---|
| VAD → Basilar thrombosis ✅ | RTA 4 days ago, bilateral UMN signs, delayed deterioration, posterior circulation syndrome | No occipital headache documented |
| Traumatic cervical spinal cord injury (TSCI) | Bilateral LL hyperreflexia, RTA | No back trauma, deterioration suggests rostral extension; doesn't explain unresponsiveness |
| Spinal epidural hematoma | RTA, UMN signs | No back pain documented, doesn't explain acute unresponsiveness |
| Central cord syndrome | Post-trauma UMN pattern | Disproportionate UL > LL weakness typical; doesn't explain unresponsiveness |
| Posterior fossa hemorrhage (traumatic) | RTA mechanism | Vitals stable makes major bleed less likely |
| Fat embolism / ICAD | Post-traumatic | Bilateral LL without respiratory features |
Immediate Management (Emergency)
1. Airway — PRIORITY
- Patient is unresponsive → secure airway immediately (intubation, but note cervical spine precautions if injury not excluded)
- SpO₂ monitoring + supplemental O₂
2. Investigations — Run in Parallel
| Investigation | Rationale |
|---|---|
| CT brain (non-contrast) | Rule out hemorrhage before anticoagulation/thrombolysis |
| CT Angiography neck + circle of Willis | Detect VAD, basilar occlusion — highest priority |
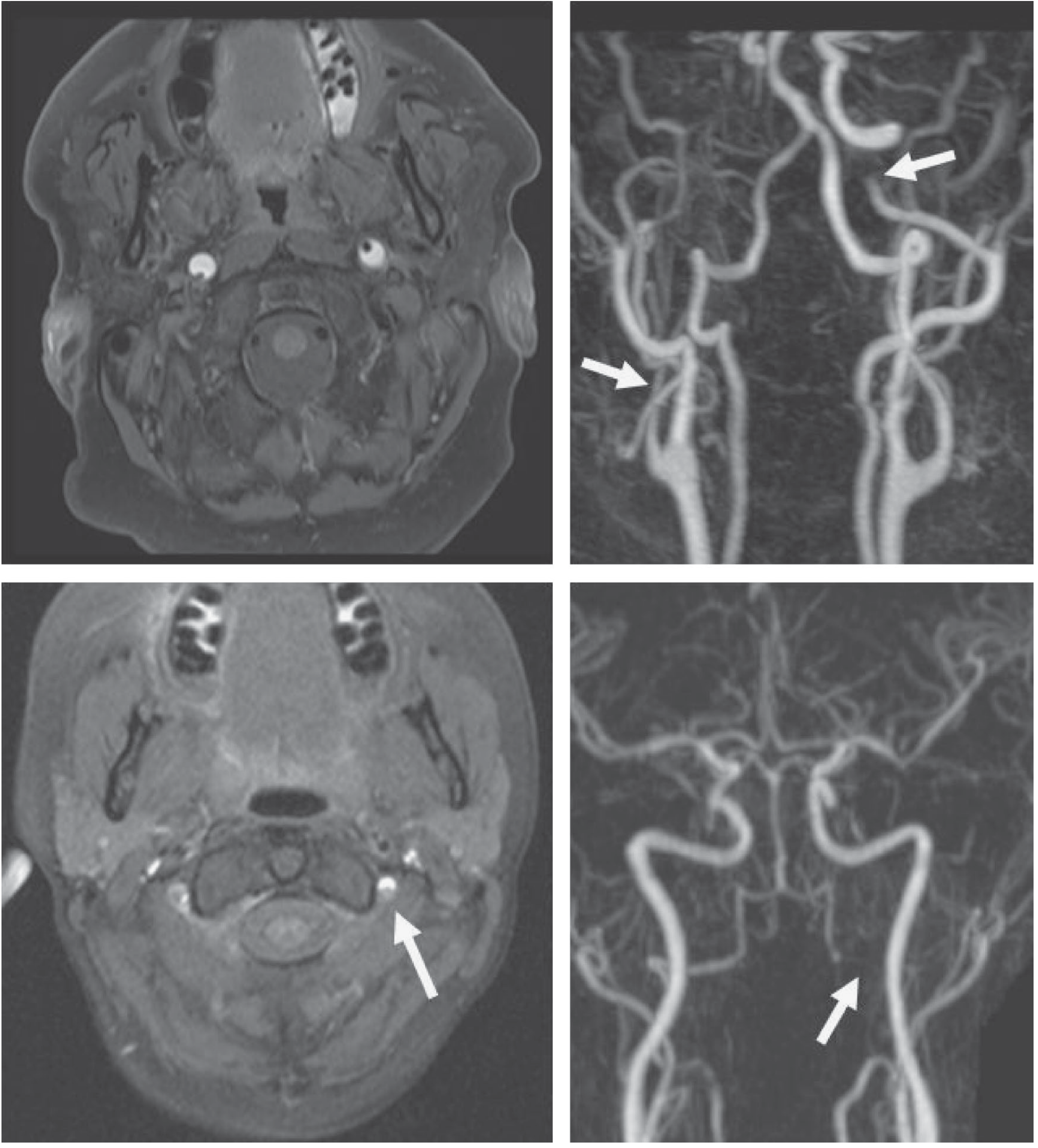
| MRI brain + MRA (if available) | T1 fat-sat shows false lumen; DWI shows acute ischemia |
| MRI cervical spine | Rule out spinal cord injury, epidural hematoma |
| ECG, cardiac monitoring | Rule out cardioembolism |
| CBC, BMP, coagulation profile, glucose | Standard stroke workup |
3. Time-Critical Interventions (if CT clears hemorrhage)
If basilar artery occlusion confirmed:
- IV tPA (alteplase) within window — Tintinalli's: "thrombolysis was equally efficacious in stroke from cervical artery dissection as in stroke from other causes, with no increased harm"
- Mechanical thrombectomy — immediately discuss with neurointerventionalist; basilar artery occlusion has high mortality without recanalization
- Anticoagulation (heparin → warfarin) OR antiplatelet therapy if not a thrombolysis candidate — both are equally effective per the CADISS trial
If spinal cord injury/epidural hematoma is identified:
- Urgent neurosurgical consultation
- Methylprednisolone is no longer standard (removed from most guidelines due to infection/sepsis risk)
4. Strict Monitoring
- Neurological observations q15 minutes
- Blood pressure management: avoid hypotension (maintain CPP); avoid hypertensive surges
- DVT prophylaxis once hemorrhage excluded
- Strict cervical spine immobilization until imaging clears
Key Clinical Clue: The 4-Day Gap
This is the textbook interval for VAD → stroke. The initial LL weakness was likely:
- A spinal cord TIA or anterior spinal artery syndrome from early VAD
- OR an early incomplete posterior circulation event
The sudden deterioration (unresponsive, unable to speak) marks basilar propagation — a neurosurgical emergency with a narrow treatment window.
"The stroke may follow the dissection by days or weeks, obscuring the relationship." — Adams & Victor's Principles of Neurology, 12th Ed.
Bottom Line
This is most likely post-traumatic vertebral artery dissection evolving to basilar artery thrombosis. The 4-day post-RTA interval, bilateral UMN signs, and sudden pontine/midbrain-level deterioration (unresponsive + mute) with stable vitals is a classic — and time-sensitive — posterior circulation emergency. Activate stroke protocol immediately. CT/CTA is the first test.
This is a shared conversation. Sign in to Orris to start your own chat.