Ataxia
Reading File
Finding Sources
Searching PubMed
"ataxia" AND ("classification" OR "management")
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Ataxia drawn from Bradley and Daroff's Neurology in Clinical Practice and Neuroanatomy through Clinical Cases, 3rd Edition.
Ataxia
Definition
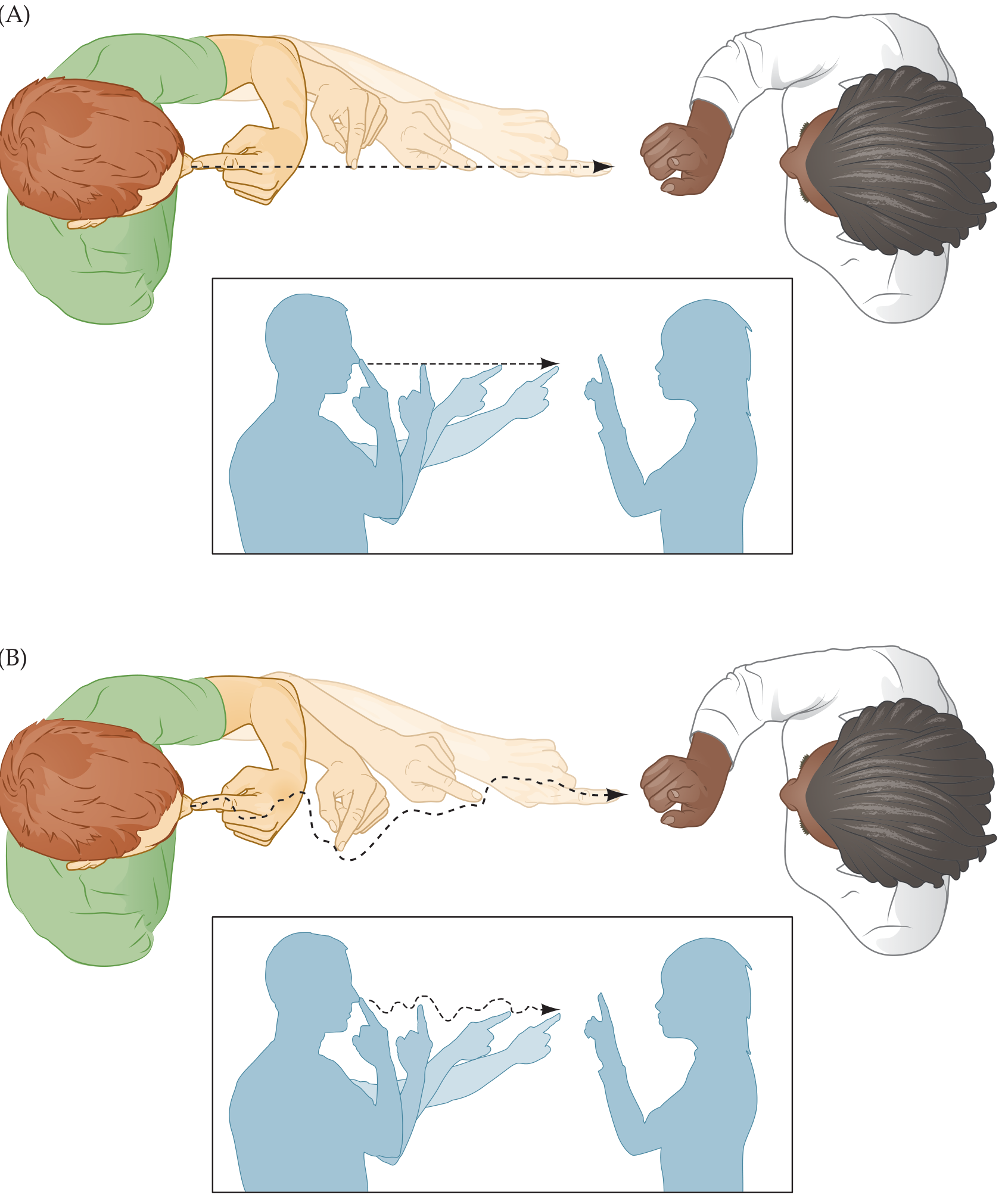
Ataxia (from the Greek "lack of order") refers to the disordered contractions of agonist and antagonist muscles and the lack of normal coordination between movements at different joints. Even simple movements require smooth coordination of multiple joints; in ataxia, movements follow an irregular, wavering course consisting of continuous overshooting, overcorrecting, and overshooting again around the intended trajectory. The fundamental defects are:
- Dysmetria - abnormal trajectories through space
- Dysrhythmia - abnormal timing of movements
Types of Ataxia
1. Cerebellar Ataxia
Caused by dysfunction of the cerebellar circuitry. The cerebellum functions as a neuronal learning machine (Marr-Albus-Ito theory), integrating sensorimotor inputs to generate predictive models for smooth movement. Dysfunction leads to erroneous motor learning and improper motor predictions.
2. Truncal vs. Appendicular Ataxia
| Feature | Truncal Ataxia | Appendicular Ataxia |
|---|---|---|
| Lesion site | Cerebellar vermis (medial) | Cerebellar hemispheres (lateral/intermediate) |
| Motor system affected | Medial motor system | Lateral motor system |
| Clinical presentation | Wide-based, unsteady "drunk-like" gait; difficulty sitting without support | Ataxia of extremity movements (dysmetria on finger-nose test) |
| Laterality | Bilateral deficit | Ipsilateral to the lesion |
3. Sensory Ataxia
Results from disruption of the posterior column-medial lemniscal pathway, causing loss of joint position sense (proprioception). Key distinguishing features:
- Impaired joint position sense on exam (unlike cerebellar ataxia)
- Worsens with eyes closed (Romberg positive)
- Improved significantly by visual feedback
4. Ataxia-Hemiparesis
A syndrome (often from lacunar infarcts) combining unilateral upper motor neuron signs with ataxia on the same side. Both deficits are contralateral to the lesion. Most commonly caused by lesions of the corona radiata, internal capsule, or pons.
Localization
- Cerebellar hemispheric lesions → ipsilateral limb ataxia
- Vermis lesions → truncal/gait ataxia (bilateral)
- Cerebellar peduncle lesions → ipsilateral ataxia (even without cerebellar hemisphere involvement)
- Frontopontine pathway lesions / hydrocephalus → gait abnormality resembling truncal ataxia ("false localization")
Signs and Symptoms
Early Symptoms
- Difficulty running, walking on high heels, or on stairs without holding railings
- Walking "as if drunk" (may be intermittent initially, triggered by even small amounts of alcohol)
- Slurred speech (scanning dysarthria) - from occasional word pronunciation difficulty to persistent problems
- Hand tremor and clumsiness, poor handwriting
- Dizziness (vertiginous or non-vertiginous)
- Diplopia (double vision), especially with quick head turns
Later Symptoms
- Falls
- Dysphagia (swallowing difficulty)
- Blurred vision
- Loss of hand dexterity for daily activities (dressing, using utensils)
Associated Neurological Signs (important diagnostic clues)
Peripheral neuropathy, parkinsonism, dystonia, tremor, sleep dysfunction, autonomic symptoms, seizures, hearing loss
Causes (by Time Course)
| Onset | Typical Causes |
|---|---|
| Acute | Vascular (stroke, hemorrhage), infectious, toxic (alcohol, drugs, heavy metals) |
| Subacute | Immune-mediated (paraneoplastic, autoimmune), Wernicke's encephalopathy, vitamin B12/E deficiency |
| Chronic/Progressive | Genetic (hereditary), degenerative (MSA-C, ILOCA), prion disease |
| Episodic | Episodic ataxia types 1 & 2, metabolic causes |
Key Acquired Causes
- Toxic: Alcohol, medications (phenytoin, lithium, chemotherapy), heavy metals
- Nutritional: Vitamin B1 (thiamine) deficiency - Wernicke's; Vitamin B12, Vitamin E deficiency
- Vascular: Cerebellar stroke or hemorrhage
- Immune/Paraneoplastic cerebellar degeneration (PCD): Most common paraneoplastic neurological syndrome (~24.3%); subacute onset over months; associated antibodies (anti-Yo, anti-Hu, etc.); associated with breast, ovarian, lung cancers
- Structural: Tumors (vermis tumors → gait ataxia; hemispheric → limb ataxia), hydrocephalus
Key Genetic Causes
- Autosomal recessive: Friedreich's ataxia (most common hereditary ataxia), ataxia-telangiectasia, POLG-ataxia, ataxia with vitamin E deficiency, abetalipoproteinemia
- Autosomal dominant: Spinocerebellar ataxias (SCAs) - >40 types; SCA1, 2, 3, 6, 7 most common
- Repeat expansion-associated: Must be screened before standard gene sequencing (conventional sequencing misses repeat expansions); includes SCA types and Friedreich's ataxia
- X-linked: FXTAS (Fragile X-associated tremor/ataxia syndrome)
- Other: CANVAS (cerebellar ataxia, neuropathy, vestibular areflexia syndrome)
Neurological Examination
Key tests:
- Gait assessment - wide-based gait, tandem walking
- Finger-nose-finger test - tests limb dysmetria
- Heel-shin test
- Rapid alternating movements - dysdiadochokinesia
- Romberg test - if positive (worsens with eyes closed), suggests sensory ataxia
- Eye movement examination - nystagmus, saccadic pursuit, gaze-evoked nystagmus
- Speech - scanning dysarthria
- SARA scale (Scale for the Assessment and Rating of Ataxia) - standardized rating
Also assess for mimickers: tremor, dystonia, myoclonus, parkinsonism, sensory neuropathy, muscle weakness, pyramidal signs.
Diagnostic Workup
Step-by-step approach (Bradley & Daroff):
- Recognize signs/symptoms and associated neurological features
- Determine chronicity (acute / subacute / chronic) and rate of progression
- Exclude structural, nutritional, and immunological causes (MRI brain, vitamin levels, autoimmune antibody panel)
- Screen for repeat expansion disorders (BEFORE gene sequencing): Friedreich's ataxia (GAA repeat in FXN), SCAs, FXTAS
- Next-generation sequencing (WES/WGS) if repeat expansions excluded
- Degenerative causes (MSA-C, ILOCA) considered when all else is negative, especially late onset
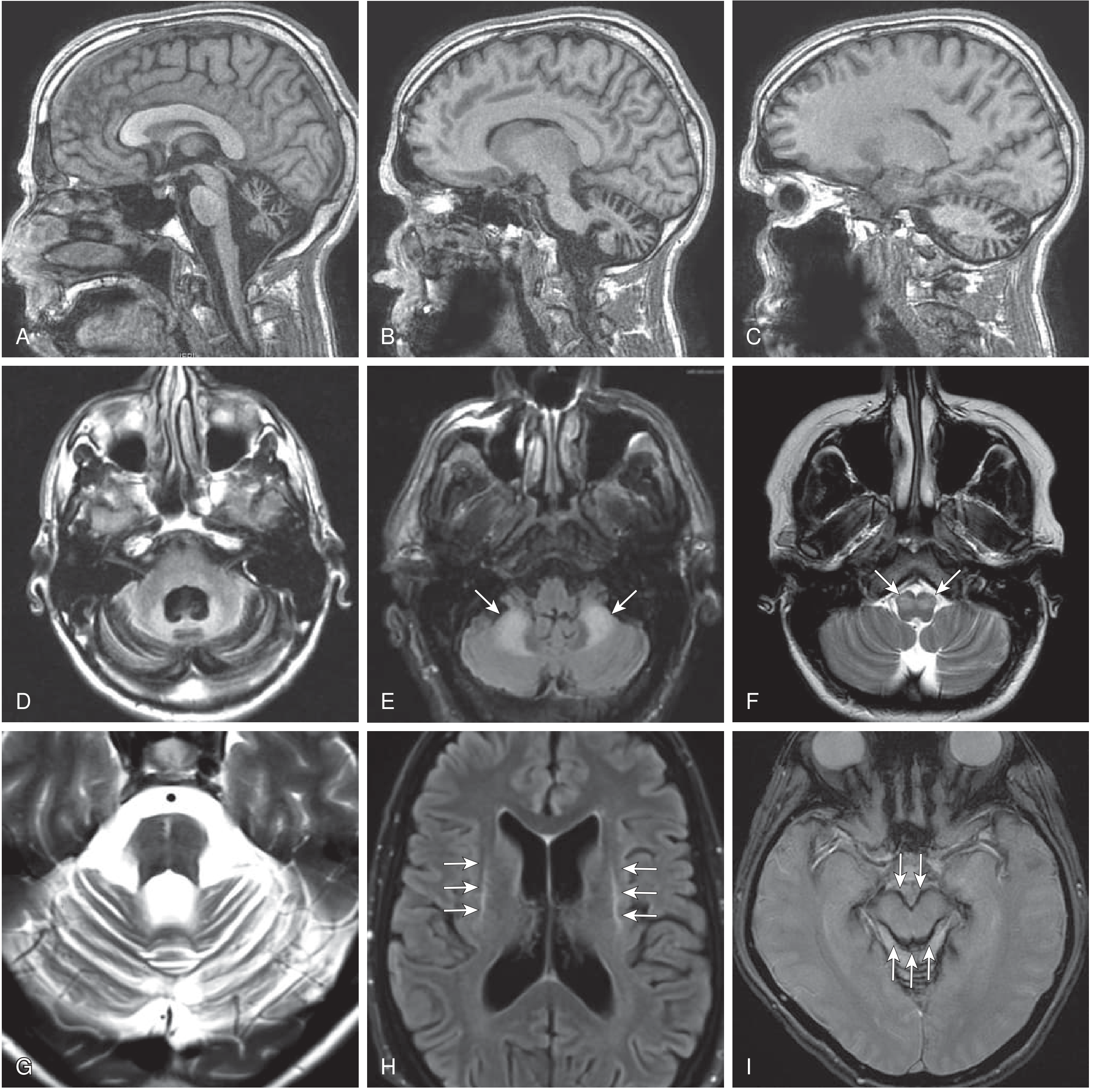
MRI Findings
Management
Pharmacological
- Treat reversible causes aggressively (thiamine for Wernicke's, immunotherapy for paraneoplastic/autoimmune, remove offending toxins)
- Symptomatic: riluzole and valproate have shown modest benefit in some cerebellar ataxias
- Tremor component: weighted wrist cuffs reduce kinetic tremor amplitude (added inertia dampens oscillation)
Non-Pharmacological
- Gait ataxia: mobility aids (cane, walker, wheelchair), fall prevention
- Displacing center of gravity forward (raising heel height, lowering walker height) helps elderly patients with postural instability
- Speech therapy for dysarthria
- Occupational therapy for hand dexterity
Targeted Molecular Therapy
- Emerging RNA-based and small molecule approaches for specific genetic ataxias (e.g., antisense oligonucleotides for SCA3)
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, Ch. 23 (Cerebellar Ataxia)
- Neuroanatomy through Clinical Cases, 3rd Edition, Ch. 15 (Cerebellar localization)
This is a shared conversation. Sign in to Orris to start your own chat.