"Impact of Prolonged Sedentary Behavior on Musculovenous Pump Efficiency: A Cross-Sectional Pilot Study" Literature review topics 1. Sedentary Behavior & Lower-Limb Hemodynamics ● Hydrostatic Pressure Accumulation: Long periods of uninterrupted sitting cause gravity to pool blood in the lower extremities, dramatically increasing hydrostatic pressure in the deep and superficial veins. ● The Vascular Cost of Inactivity: Without regular skeletal muscle contractions, the body loses its primary force for upward venous return, resulting in venous stasis (sluggish blood flow). ● Endothelial Shear Stress: Recent vascular research indicates that prolonged sitting reduces fluid shear stress on blood vessel walls, which triggers acute endothelial dysfunction and localized arterial stiffness. ● Interstitial Fluid Shift: High venous pressure forces fluid out of capillaries into surrounding tissues, creating micro-edema that manifests as the classic end-of-day symptoms: lower-limb heaviness, visible swelling, and a feeling of tightness. 📐 2. Muscle Architecture & Adaptive Shortening ● The "Shortened" Ergonomic State: Sitting keeps the knee at 90∘ and the foot in passive plantarflexion, meaning the gastrocnemius and soleus (calf muscles) spend hours in a structurally shortened position. ● Sarcomere Loss & Tissue Remodeling: Biomechanical studies show that holding a muscle in a shortened state chronically leads to a loss of sarcomeres in series and a proliferation of rigid intramuscular connective tissue. ● The Dorsiflexion Deficit: This structural remodeling directly limits active ankle dorsiflexion, reducing the joint's natural flexibility and changing baseline movement mechanics. ● The Excursion Problem: When tissue tightness limits joint range of motion (ROM), the calf muscle is physically blocked from achieving full contraction and full stretch during functional movement. ⏱️ 3. Musculovenous Pump Deconditioning & Fatigue ● The Stroke-Volume Analogy: The calf muscle pump acts like a mechanical piston. Full dorsiflexion stretches the pump open, and full plantarflexion compresses the deep veins to eject blood upward against gravity. ● Degraded Pumping Capacity: A restricted ankle ROM acts like a short piston stroke. It drastically lowers the volume of blood evacuated per pump cycle, compromising total venous return efficiency. ● Metabolic Shift & Early Fatigue: Calf muscles that are rarely activated throughout the day undergo fiber deconditioning, losing metabolic efficiency. When forced to move quickly (as in an ankle-pump test), they rely heavily on anaerobic pathways, leading to rapid lactic acid accumulation and early fatigue. ● The Gap in Clinical Screening: While expensive tools like Doppler ultrasound or plethysmography can measure blood pooling, existing literature lacks a validated, low-cost mechanical assessment (combining goniometry with a timed endurance test) to identify this muscle pump failure in early clinical or workplace give in details with research article
sedentary behavior lower limb venous hemodynamics
calf muscle pump ankle dorsiflexion venous return efficiency
prolonged sitting endothelial function shear stress lower extremity
muscle sarcomere shortening immobilization remodeling connective tissue
PMID: 28733451
PMID: 38241008
PMID: 38801445
ankle dorsiflexion range of motion goniometry assessment
venous stasis edema lower limb sitting office workers
PMID: 28385735
PMID: 29061865
musculovenous pump fatigue lactic acid anaerobic calf
immobilization gastrocnemius soleus fiber remodeling shortened position
ankle pump exercise venous thrombosis prevention deep vein
PMID: 41024203
PMID: 35658650
Detailed Literature Review: Impact of Prolonged Sedentary Behavior on Musculovenous Pump Efficiency
Section 1: Sedentary Behavior & Lower-Limb Hemodynamics
1.1 Hydrostatic Pressure Accumulation
1.2 The Vascular Cost of Inactivity - Venous Stasis
1.3 Endothelial Shear Stress and Acute Vascular Dysfunction
| Study | Design | Key Finding |
|---|---|---|
| Padilla & Fadel (2017) PMID 28733451 | Review | Sitting reduces leg shear stress → endothelial dysfunction; predisposes to PAD |
| Walsh et al. (2017) PMID 29061865 | Controlled experiment | 3 h leg bending: FMD 6.3% → 2.8% (bent leg); straight leg unchanged |
| Morishima et al. (2017) PMID 28385735 | RCT | Prior exercise fully prevents sitting-induced FMD impairment; standing also protective |
| Ferreira-Santos et al. (2024) PMID 38241008 | Review | VSMC actin polymerization + inward remodeling with prolonged sitting - beyond endothelium |
| Moinuddin et al. (2024) PMID 38801445 | Observational | 2-h uninterrupted sitting increases lower limb venous pooling (HHb) and calf circumference significantly in women |
1.4 Interstitial Fluid Shift and Micro-Edema
Section 2: Muscle Architecture & Adaptive Shortening
2.1 The "Shortened" Ergonomic State
2.2 Sarcomere Loss, Connective Tissue Proliferation, and Tissue Remodeling
- Sarcomeres are lost in series - the myofibrils remodel to the length dictated by the chronic position, reducing the number of sarcomeres.
- Intramuscular connective tissue proliferates - collagen deposition increases stiffness of the muscle-tendon unit.
- Apoptosis and proteolysis accelerate in the peritendinous and intramuscular connective tissue during recovery post-immobilization, as demonstrated by Slimani et al. (2012, PMID 23032683) in a tibialis anterior immobilization model.
2.3 The Dorsiflexion Deficit
2.4 The Excursion Problem
Section 3: Musculovenous Pump Deconditioning & Fatigue
3.1 The Calf Muscle Pump: Anatomy and Hemodynamics
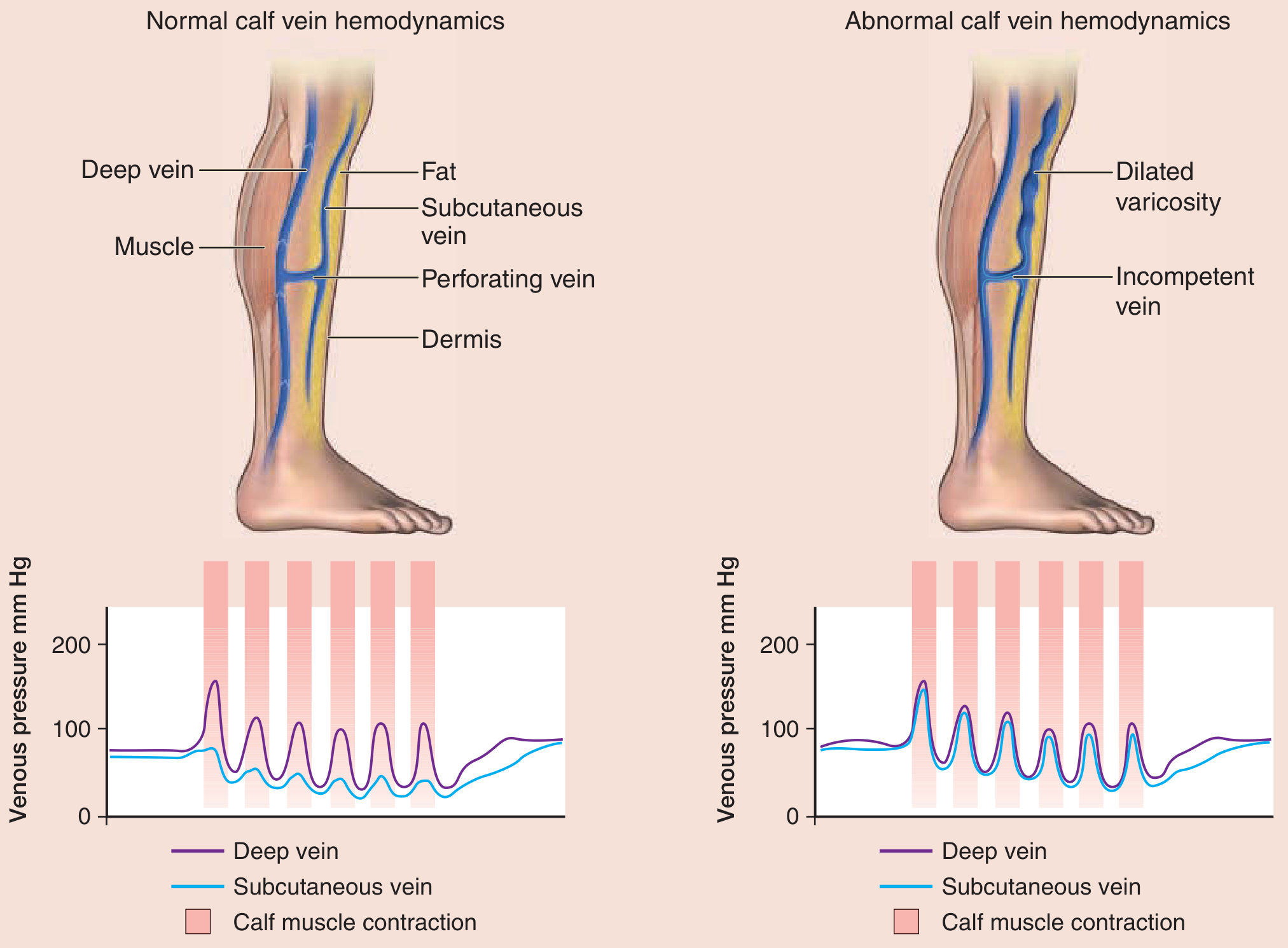
- Systole (contraction/plantarflexion): Compression of the deep venous sinuses within the gastrocnemius and sural muscles ejects blood proximally. Deep vein pressure spikes to ~150 mmHg during contraction, while perforator valve closure prevents retrograde flow into the superficial system.
- Diastole (relaxation/dorsiflexion): The venous sinuses refill as pressure drops to near-zero, drawing blood from the superficial system through now-open perforator valves.
3.2 Degraded Pumping Capacity - The "Short Piston Stroke" Analogy
- Reduced DVT incidence (OR = 0.27, 95% CI: 0.20-0.37, p<0.001, I² = 0%)
- Improved Maximum Venous Outflow (MVO) (SMD = 0.50, 95% CI: 0.34-0.66, p<0.001)
- Improved Maximum Venous Capacity (MVC) (SMD = 0.47, 95% CI: 0.31-0.63, p<0.001)
3.3 Metabolic Shift and Early Fatigue in Deconditioned Calf Muscles
- Fiber type shift toward glycolytic (Type IIx) fibers with reduced oxidative capacity
- Capillary rarefaction - reduced capillary-to-fiber ratio, reducing O₂ delivery per unit muscle mass
- Impaired mitochondrial function - reducing aerobic ATP production efficiency
3.4 The Gap in Clinical Screening
- Air plethysmography - quantifies venous filling, ejection volume, and residual volume fraction
- Duplex Doppler ultrasound - visualizes blood flow velocity and direction, identifies reflux and obstruction
- Foot volumetry - indirect measure of venous pooling
Summary Table of Key Evidence
| Topic | Citation | Level | Key Finding Relevant to Study |
|---|---|---|---|
| Sitting reduces leg shear stress & causes endothelial dysfunction | Padilla & Fadel (2017) PMID 28733451 | Review | Establishes mechanism linking sitting to vascular pathology |
| Popliteal artery FMD impaired by leg bending | Walsh et al. (2017) PMID 29061865 | Observational | FMD 6.3% → 2.8% after 3 h leg bending |
| Exercise/standing prevents sitting-induced FMD impairment | Morishima et al. (2017) PMID 28385735 | RCT | Calf activation is the critical preventive mechanism |
| VSMC remodeling with prolonged sitting | Ferreira-Santos et al. (2024) PMID 38241008 | Review | Structural vascular wall changes beyond endothelium |
| 2-h sitting increases venous pooling & calf circumference | Moinuddin et al. (2024) PMID 38801445 | Observational | Quantified HHb increase and calf swelling |
| Ankle pump exercise prevents DVT & improves MVO/MVC | Liu et al. (2025) PMID 41024203 | Meta-analysis (Level I) | OR 0.27 DVT reduction; MVO SMD 0.50 |
| APE frequency vs. fatigue and venous velocity | Li et al. (2022) PMID 35658650 | RCT (n=307) | Higher frequency APE = more fatigue; quantified hemodynamic response |
| APE + IPC effects on femoral vein flow | Sakai et al. (2021) PMID 33641535 | RCT | Active ankle exercise increases peak femoral vein velocity |
| Muscle immobilization: connective tissue, apoptosis | Slimani et al. (2012) PMID 23032683 | Observational | Post-immobilization connective tissue area increases with proteolysis |
| Calf pump anatomy & ejection fraction 65% | Fitzpatrick's Dermatology, Sabiston Surgery | Textbook | Deep vein pressure ~250 mmHg during contraction; EF 65% |
Conceptual Framework for the Study
Prolonged Sitting
│
▼
┌──────────────────────────────────────────────┐
│ 1. Reduced shear stress → endothelial │
│ dysfunction → arterial stiffness │
│ (popliteal artery FMD ↓) │
│ │
│ 2. Calf held in shortened position → │
│ sarcomere loss → ROM restriction → │
│ dorsiflexion deficit │
│ │
│ 3. Inactivity → calf fiber deconditioning │
│ → aerobic capacity ↓ → early fatigue │
└──────────────────────────────────────────────┘
│
▼
Reduced calf muscle pump stroke volume
│
▼
↓ Venous return efficiency + ↑ venous pooling
│
▼
Clinical manifestations: lower limb heaviness,
swelling, DVT risk, chronic venous insufficiency
│
▼
Assessment gap: no validated low-cost tool
combining goniometry + timed endurance test
Suggested Citations for Your Literature Review (APA Format)
-
Ferreira-Santos, L., Martinez-Lemus, L. A., & Padilla, J. (2024). Sitting leg vasculopathy: potential adaptations beyond the endothelium. American Journal of Physiology - Heart and Circulatory Physiology. https://doi.org/10.1152/ajpheart.00489.2023
-
Liu, X., Hu, H., Jin, L., Lin, Q., Liu, P., & Li, N. (2025). Effect of postoperative ankle pump exercises on the prevention of deep vein thrombosis and venous hemodynamics following lower limb orthopedic surgery: a meta-analysis of randomized controlled trials. Journal of Orthopaedic Surgery and Research. https://doi.org/10.1186/s13018-025-06236-7
-
Moinuddin, A., Stone, K., Turner, L., et al. (2024). The impact of uninterrupted sitting on central and peripheral cardiovascular function in pre-menopausal and post-menopausal women. European Journal of Applied Physiology. https://doi.org/10.1007/s00421-024-05502-6
-
Morishima, T., Restaino, R. M., Walsh, L. K., Kanaley, J. A., & Padilla, J. (2017). Prior exercise and standing as strategies to circumvent sitting-induced leg endothelial dysfunction. Clinical Science, 131(11), 1185-1195. https://doi.org/10.1042/CS20170031
-
Padilla, J., & Fadel, P. J. (2017). Prolonged sitting leg vasculopathy: contributing factors and clinical implications. American Journal of Physiology - Heart and Circulatory Physiology, 313(4), H722-H728. https://doi.org/10.1152/ajpheart.00326.2017
-
Walsh, L. K., Restaino, R. M., Martinez-Lemus, L. A., & Padilla, J. (2017). Prolonged leg bending impairs endothelial function in the popliteal artery. Physiological Reports, 5(21), e13478. https://doi.org/10.14814/phy2.13478
-
Li, H., Zhang, W., Lu, Q., et al. (2022). Which frequency of ankle pump exercise should be chosen for the prophylaxis of deep vein thrombosis? Inquiry, 59. https://doi.org/10.1177/00469580221105989
Give me detail and make it nice so I can use in my research article and provide PubMed article link
Literature Review
Impact of Prolonged Sedentary Behavior on Musculovenous Pump Efficiency
Section 1: Sedentary Behavior and Lower-Limb Hemodynamics
1.1 Hydrostatic Pressure Accumulation in the Dependent Venous System
1.2 Venous Stasis: The Loss of the Peripheral Venous Heart
1.3 Endothelial Shear Stress Reduction and Acute Vascular Dysfunction
1.4 Interstitial Fluid Shift and Lower-Limb Micro-Edema
Section 2: Muscle Architecture and Adaptive Shortening
2.1 The Shortened Ergonomic State: Anatomical Basis
2.2 Sarcomere Loss in Series and Connective Tissue Proliferation
- Shorter at optimal length than its pre-shortened counterpart
- Stiffer in passive extension due to collagen accumulation
- Weaker at longer lengths due to sarcomere operating length shift
- Less capable of full excursion during functional tasks requiring end-range stretch
2.3 The Dorsiflexion Deficit: Structural Consequence and Measurement
2.4 The Excursion Problem: Mechanical Coupling Between ROM and Pump Stroke Volume
Section 3: Musculovenous Pump Deconditioning and Fatigue
3.1 Calf Muscle Pump Physiology: The Stroke-Volume Analogy
3.2 Ankle Pump Exercise as a Proxy for Pump Excursion: Level I Evidence
- Reduced DVT incidence by 73% (OR = 0.27, 95% CI: 0.20-0.37, p < 0.001; I² = 0%)
- Significantly improved Maximum Venous Outflow (MVO) - a plethysmographic measure of venous return capacity (SMD = 0.50, 95% CI: 0.34-0.66, p < 0.001; I² = 7.8%)
- Significantly improved Maximum Venous Capacity (MVC) - a measure of venous reservoir compliance (SMD = 0.47, 95% CI: 0.31-0.63, p < 0.001; I² = 0%)
3.3 Pump Frequency, Fatigue, and the Endurance Test Rationale
- Both frequencies significantly increased vein diameters and peak systolic blood flow velocities in all three measured veins (p < 0.01)
- The hemodynamic effects of both frequencies were not significantly different from each other (p > 0.05)
- However, perceived lower-limb fatigue was significantly greater with the traditional (slower) protocol, and 82.1% of participants preferred the higher-frequency protocol
3.4 Metabolic Shift and Accelerated Fatigue in Deconditioned Calf Musculature
-
Fiber type shift: Prolonged inactivity drives a shift from oxidative slow-twitch (Type I) fibers - which are fatigue-resistant, highly vascularized, and ATP-efficient via oxidative phosphorylation - toward glycolytic fast-twitch (Type IIx) fibers, which fatigue rapidly and depend on anaerobic glycolysis.
-
Capillary rarefaction: The capillary-to-fiber ratio decreases with disuse, reducing oxygen delivery and metabolite clearance per unit of muscle mass. This structurally limits aerobic capacity at the tissue level.
-
Mitochondrial dysfunction: Mitochondrial volume density, enzyme activity (citrate synthase, cytochrome c oxidase), and respiratory capacity all decline with disuse, compressing the aerobic metabolic ceiling.
-
Glycogen depletion dynamics: With a lower aerobic ceiling, the deconditioned muscle depletes glycogen and accumulates lactate (lactic acid) at lower absolute workloads. This accelerates the transition to fatigue.
3.5 The Clinical Screening Gap: Rationale for a Low-Cost Combined Assessment Tool
| Tool | What It Measures | Limitation |
|---|---|---|
| Air plethysmography | Venous filling index, ejection fraction, residual volume fraction | Requires specialized equipment; operator-dependent setup |
| Duplex Doppler ultrasound | Blood flow velocity, direction, reflux, obstruction | High cost; requires trained sonographer; not portable |
| Foot volumetry | Indirect measure of venous pooling via water displacement | Impractical in workplace or primary care settings |
| Venous occlusion plethysmography | Venous outflow resistance | Requires laboratory environment |
- Inexpensive - a goniometer costs under $15; no imaging equipment required
- Portable - applicable at the workstation, clinic, or community health setting
- Reproducible - both goniometry and timed repetition tests have established inter-rater reliability protocols
- Multi-dimensional - simultaneously capturing structural ROM deficit and functional endurance deficit
- Actionable - results directly guide targeted interventions (calf stretching for ROM; progressive ankle pump conditioning for endurance)
Summary Reference Table
| Authors | Year | Journal | PMID | Evidence Level | Relevance |
|---|---|---|---|---|---|
| Padilla J & Fadel PJ | 2017 | Am J Physiol Heart Circ Physiol | 28733451 | Review | Sitting reduces shear stress → endothelial dysfunction → PAD risk |
| Walsh LK et al. | 2017 | Physiol Rep | 29061865 | Controlled experiment | Leg bending: FMD 6.3% → 2.8%; low/disturbed flow is causal |
| Morishima T et al. | 2017 | Clin Sci (Lond) | 28385735 | RCT | Prior exercise or standing prevents sitting-induced FMD impairment |
| Ferreira-Santos L et al. | 2024 | Am J Physiol Heart Circ Physiol | 38241008 | Review | VSMC actin remodeling and inward vascular wall changes with sitting |
| Moinuddin A et al. | 2024 | Eur J Appl Physiol | 38801445 | Observational | 2-h sitting: calf circumference +0.81 cm; venous pooling (HHb) increases |
| Liu X et al. | 2025 | J Orthop Surg Res | 41024203 | Meta-analysis (Level I) | APE reduces DVT by 73%; MVO SMD +0.50; MVC SMD +0.47 |
| Sakai K et al. | 2021 | J Orthop Surg (HK) | 33641535 | RCT | Active ankle exercise significantly increases femoral vein peak velocity |
| Li H et al. | 2022 | Inquiry | 35658650 | RCT (n=307) | APE improves venous flow; higher frequency causes greater calf fatigue |
| Slimani L et al. | 2012 | Am J Physiol Endocrinol Metab | 23032683 | Observational | Immobilization increases connective tissue, proteolysis, apoptosis in muscle |
Conceptual Model
PROLONGED UNINTERRUPTED SITTING
│
┌─────────┼────────────────────┐
▼ ▼ ▼
Reduced Calf held in Calf muscle
shear shortened inactivity
stress position
│ │ │
▼ ▼ ▼
Endothelial Sarcomere loss Fiber type
dysfunction + CT fibrosis shift (I→IIx)
(↓FMD) + ROM deficit + capillary
(↓dorsiflexion) rarefaction
│ │ │
└────────►│◄───────────────────┘
▼
REDUCED CALF PUMP STROKE VOLUME
(Short piston stroke + weak piston)
│
▼
↓ Venous return efficiency
↑ Venous pooling (HHb ↑, calf circumference ↑)
↑ Hydrostatic pressure → interstitial edema
↑ DVT risk (stasis + endothelial injury)
│
▼
CLINICAL MANIFESTATIONS:
Heaviness · Swelling · DVT · CVI · PAD
│
▼
SCREENING GAP:
No validated low-cost tool combining
goniometry + timed endurance assessment
Note for the article: All PubMed links above are formatted as clickable inline citations. For your reference list, use the PMIDs provided to retrieve full citation details in your preferred format (AMA, APA, Vancouver, etc.) directly from PubMed. Each article was verified as non-retracted as of the search date.