Penile fracture
Reading File
Finding Sources
Searching PubMed
"penile fracture" management
Reading File
Finding Sources
Searching PubMed
"penile fracture" surgery outcomes
Reading File
Reading File
Reading File
I now have comprehensive textbook content. Let me compile the full answer.
Penile Fracture
Definition and Anatomy
Penile fracture is a traumatic disruption of the tunica albuginea - the thick fibrous sheath surrounding the corpora cavernosa. The tunica albuginea is 2-3 mm thick in the flaccid state but thins to less than 0.5 mm during erection, making it vulnerable to sudden angular force. The injury strictly requires an erect penis, as the flaccid tunica is too thick and elastic to fracture.
Epidemiology and Mechanism
- Most commonly caused by excessive, sudden angulation of the erect penis against the perineum or partner's perineum during vigorous vaginal intercourse
- Also reported with masturbation, rolling over onto an erect penis, or forceful bending
- The laceration is classically found on the pendulous/distal shaft, though more proximal tears occur
- There is frequently a delay in presentation due to patient embarrassment
Clinical Features
Classic Presentation - the "3 P's":
- Pop/crack - audible snapping sound as the tunica tears
- Pain - immediate sharp pain
- Penile swelling + rapid detumescence - the erection instantly deflates
Physical Examination
- "Eggplant deformity" (also called "aubergine penis"): swollen, ecchymotic, dark-colored penile shaft from expanding hematoma
- Deviation of the penis away from the side of the tear (the "rolling sign")
- The fracture line may be palpable as a defect in the tunica
- A clot often overlies the cavernosal rupture site
- If Buck's fascia (the deep fascia) is intact, hematoma stays confined to the penile shaft; if it ruptures, bruising spreads to the scrotum, perineum, or lower abdomen in a "butterfly" distribution
Associated Urethral Injury
- Occurs in approximately 20% of cases
- Suggested by: hematuria, inability to void, blood at the urethral meatus
- Requires retrograde urethrography (RUG) to rule out
Diagnosis
Penile fracture is a clinical diagnosis - history and physical examination are usually sufficient and definitive. Imaging is reserved for unclear cases.
| Modality | Role |
|---|---|
| Clinical exam | Primary - usually diagnostic |
| Ultrasound (high-freq) | Confirms tear location; useful when diagnosis is uncertain; guides incision choice |
| MRI | Most accurate non-invasive modality; recommended by AUA guidelines when ultrasound is equivocal |
| Cavernosography | Discouraged - time-consuming, unfamiliar to most surgeons, and offers no advantage |
| RUG | Performed if urethral injury suspected (hematuria, meatal blood, retention) |
False fracture (rupture of dorsal penile artery or vein) can mimic penile fracture with swelling, ecchymosis, and even a "snap-pop" sensation - surgical exploration or MRI is indicated in these ambiguous cases.
Management
Surgical (Standard of Care)
Immediate exploration and surgical repair is mandatory. Non-operative management is contraindicated - it leads to fibrosis, Peyronie-like plaques, penile curvature, abscess, and missed urethral injury.
Surgical approach options:
| Approach | When Used |
|---|---|
| Ventral vertical penoscrotal incision | Most common - ideal since most fractures are ventral or lateral |
| Small lateral incision | Localized hematoma or palpable defect |
| Distal circumcising incision | Allows inspection of the full length of both corpora cavernosa and urethra |
Operative steps:
- Deglove penis via circumcising subcoronal incision OR penoscrotal incision
- Evacuate hematoma
- Identify and inspect the full length of both corpora and urethra
- Close corporeal laceration with absorbable sutures (e.g., 2-0 or 3-0 PDS or Vicryl) in interrupted or running fashion
- If urethral injury present: repair over a catheter
- Skin closure
Non-operative Management
Non-operative management (ice, anti-inflammatory medications, splinting) is associated with:
- High rates of penile curvature (Peyronie's disease)
- Abscess formation
- Erectile dysfunction
- Prolonged recovery
- This approach is not recommended by any major guideline.
Outcomes
Patients who undergo expedient surgical repair have:
- Low complication rates
- Good erectile function preservation
- Avoidance of disabling penile curvature
Delayed repair or non-operative management results in significantly higher rates of long-term erectile dysfunction and penile deformity.
Complications
| Complication | Notes |
|---|---|
| Penile curvature | Most common long-term complication; related to fibrotic scar |
| Erectile dysfunction | Especially with delayed or missed repair |
| Peyronie's disease | Fibrotic plaque formation at the tunica laceration site |
| Abscess | Rare with prompt surgical treatment |
| Urethral stricture | If urethral injury is missed or inadequately repaired |
Key Points Summary
- Fracture of the tunica albuginea of the erect penis
- Classic triad: pop + pain + rapid detumescence with "eggplant deformity"
- 20% have associated urethral injury - always evaluate
- Diagnosis is clinical; imaging (US, MRI) reserved for equivocal cases
- Immediate surgical repair is the treatment of choice
- Non-operative management should not be performed
Sources: Fischer's Mastery of Surgery (8th ed.); Campbell-Walsh-Wein Urology (11th ed.); Smith & Tanagho's General Urology (19th ed.)
IBS
Finding Sources
Searching PubMed
"irritable bowel syndrome" management treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, rich content. Let me compile the full answer.
Irritable Bowel Syndrome (IBS)
Definition
IBS is a disorder of gut-brain interaction (formerly called "functional bowel disorder") characterized by chronic or recurrent abdominal pain associated with alterations in stool form and/or frequency. It is not a structural or biochemical disease - no pathognomonic organic abnormality has been identified. IBS sits within a spectrum of functional bowel disorders that also includes functional constipation, functional diarrhea, and functional abdominal bloating.
Epidemiology
- Worldwide prevalence: 4.1% (Rome IV criteria); higher with older Rome III criteria (~9%)
- More common in women (5.2%) than men (2.9%)
- Estimated incidence: ~38 per 10,000 person-years
- Up to 50% of affected individuals never seek care, yet IBS generates ~4.4 million physician visits/year in the US
- Associated with significant healthcare costs, absenteeism, and impaired work productivity
- Patients are more likely to undergo unnecessary diagnostic tests and surgeries
Subtypes (Rome IV)
| Subtype | Abbreviation | Prevalence |
|---|---|---|
| Predominant diarrhea | IBS-D | 35-40% |
| Mixed bowel habits | IBS-M | 35-40% |
| Predominant constipation | IBS-C | ~25% |
| Unclassified | IBS-U | <5% |
Subtypes are classified by stool form (Bristol Stool Scale), not frequency. They can transition over time in the same patient.
Pathophysiology
IBS results from dysregulation of gut-brain interactions, with contributions from multiple mechanisms:
1. Visceral Hypersensitivity
- The primary and most consistent finding
- Lowered pain thresholds to intestinal distention (allodynia/hyperalgesia)
- Mediated through sensitized afferent neurons and altered CNS processing
2. Altered Motility
- Colonic transit is generally slower in IBS-C and faster in IBS-D
- No single motility pattern is specific to IBS
- Exaggerated responses to meals, CCK, and mechanical stimuli are reported
3. Gut Microbiota (Dysbiosis)
- Colonization of germ-free animals with IBS microbiota induces visceral hypersensitivity, impairs intestinal permeability, and alters GI transit
- Gram-negative dysbiosis downregulates the serotonin reuptake transporter (SERT) in the mucosa
4. Abnormal Serotonin Pathways
- Serotonin-containing enterochromaffin cells are increased in IBS-D
- Postprandial serotonin levels are elevated in IBS-D patients
- TPH1 (tryptophan hydroxylase 1) polymorphisms are associated with IBS subtypes
5. Mucosal Immune Activation
- Low-grade mucosal inflammation with mast cell activation
- Increased cytokines/chemokines may explain extra-GI symptoms (fatigue, myalgia, anxiety)
6. Increased Intestinal Permeability
- "Leaky gut" allows antigen exposure to immune cells in the lamina propria
7. Altered CNS Modulation
- Abnormal central processing of visceral pain signals
- Strong association with psychosocial factors (anxiety, depression, trauma)
8. Bile Acids
- Up to 25% of IBS-D patients have idiopathic bile acid diarrhea
- Reduced FGF-19 synthesis by the ileal mucosa impairs negative feedback on bile acid synthesis
- Excess colonic bile acids accelerate transit, increase permeability, and cause visceral hypersensitivity
Risk Factors
- Genetic predisposition (familial clustering; 1.75-2.75x increased risk in relatives)
- Adverse childhood experiences
- Post-infectious IBS (after acute gastroenteritis - well established)
- Food triggers
- Psychological stress
Diagnostic Criteria
Rome IV Criteria (2016) - Current Standard
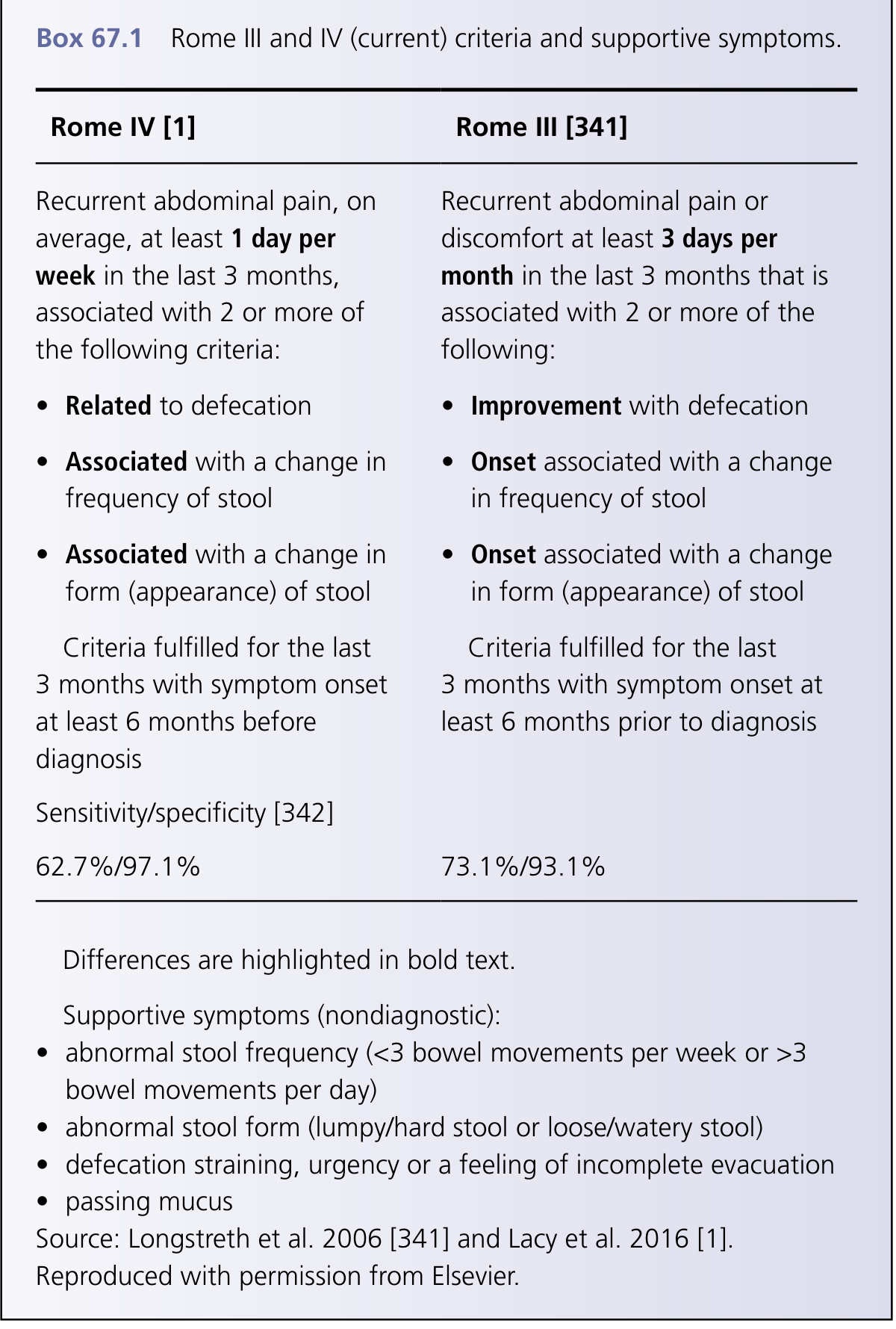
Rome IV requires: Recurrent abdominal pain, on average at least 1 day per week in the last 3 months, associated with 2 or more of:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
Criteria must be fulfilled for the last 3 months with symptom onset at least 6 months before diagnosis.
Key change from Rome III: frequency threshold increased from "3 days/month" to "1 day/week," and "discomfort" was removed from the definition (only "pain" qualifies). This is why Rome IV prevalence is roughly half of Rome III.
Supportive (non-diagnostic) symptoms:
- Abnormal stool frequency (<3/week or >3/day)
- Abnormal stool form (hard/lumpy or loose/watery)
- Defecation straining, urgency, or incomplete evacuation
- Passing mucus
Clinical Features
GI Symptoms
- Crampy, lower abdominal pain - often postprandial
- Pain attacks: median 5.4/month, median duration 2.8 hours
- Bloating and abdominal distension (more prominent in IBS-C)
- Altered bowel habits - diarrhea, constipation, or both
- Mucus in stool
- Sensation of incomplete evacuation
Extra-GI Symptoms (very common)
IBS patients carry substantially increased burden of non-GI symptoms:
| Symptom | Prevalence in IBS |
|---|---|
| Fatigue | 36-63% |
| Back pain | 27-81% |
| Urinary frequency/urgency | 21-61% |
| Dyspareunia | 9-42% |
| Headache | 23-45% |
| Myalgia | 29-36% |
| Dizziness | 11-27% |
Features Supporting IBS
- Recurrence over time without progression
- Onset during periods of stress
- Absence of fever, weight loss, bleeding
- Small-volume stools without blood
- Symptoms improve (or worsen) with bowel movements
Alarm Features (argue AGAINST IBS)
- First onset after age 40-50
- Progressive course
- Rectal bleeding
- Significant unexplained weight loss
- Nocturnal diarrhea
- Steatorrheal stools
- Persistent diarrhea despite 48-hour fast
- Anemia, elevated ESR/CRP, leukocytes/blood in stool
- Stool volume >200-300 mL/day
- Family history of colorectal cancer, IBD, or celiac disease
Differential Diagnosis
| Category | Conditions |
|---|---|
| Inflammatory | IBD (Crohn's, UC), microscopic colitis |
| Infectious | Giardia, parasites, SIBO |
| Malabsorptive | Celiac disease, lactase deficiency |
| Endocrine | Hypothyroidism, hyperthyroidism, hypoparathyroidism |
| Structural | Colorectal cancer, diverticular disease |
| Other | Biliary tract disease, gastroparesis, bile acid diarrhea, acute intermittent porphyria, lead poisoning |
Diagnostic Workup
Minimal evaluation (no alarm features, typical presentation)
- CBC
- Fecal calprotectin or lactoferrin (to screen for IBD, especially in IBS-D)
- CRP (in IBS-D)
- Celiac serology (anti-tTG IgA + total IgA) in IBS-D populations where celiac prevalence ≥1%
Additional tests (when indicated)
- Stool ova and parasites (if endemic area or exposure history)
- Hydrogen breath test (lactose) or 3-week lactose-free trial
- Glucose hydrogen breath test (SIBO)
- Colonoscopy with random biopsies: indicated with alarm features, onset >40, or treatment failure; biopsies rule out microscopic colitis
- Upper GI endoscopy: for concurrent dyspepsia symptoms
- Abdominal ultrasound: if right upper quadrant pain suggests biliary disease
Treatment
Treatment is stratified by severity and subtype.
Step 1: Education, Reassurance, Lifestyle
- Explain the functional/brain-gut nature of the disorder
- Identify and eliminate individual food triggers
- Stress management
- Exercise (low risk, overall benefit)
- Avoid nutritionally depleted diets
Step 2: Dietary Interventions
Low-FODMAP Diet (strongest dietary evidence)
FODMAP = Fermentable Oligosaccharides, Disaccharides, Monosaccharides, And Polyols
High-FODMAP foods are poorly absorbed in the small intestine and fermented by colonic bacteria, producing gas and osmotically active carbohydrates - causing bloating, flatulence, and diarrhea. They may also fuel dysbiosis and mucosal dysfunction.
Response rate: 50-80% of IBS patients. A network meta-analysis of 13 RCTs showed low-FODMAP was superior to all other dietary interventions (2025, Lancet Gastroenterol Hepatol, PMID 40258374).
Three-step implementation:
- Restriction phase (2-6 weeks): eliminate all 5 FODMAP subgroups
- Reintroduction phase: challenge individual FODMAPs to identify personal triggers
- Maintenance phase: personalized long-term diet
Caution: avoid in patients with eating disorders or avoidant/restrictive eating behaviors.
Fiber
- Soluble fiber (psyllium): effective for IBS-C; reduces perception of rectal distention
- Insoluble fiber (wheat bran): not supported by evidence, may worsen symptoms
- Start low, titrate slowly to 20-30 g/day total
Step 3: Symptom-Targeted Pharmacotherapy
For IBS-D (diarrhea-predominant)
| Drug | Class | Notes |
|---|---|---|
| Loperamide | Opioid receptor agonist | First-line; reduces stool frequency and urgency; does NOT improve pain |
| Rifaximin | Non-absorbable antibiotic | Effective for bloating and global IBS-D; typically 2-week course |
| Alosetron | 5-HT3 antagonist | Severe IBS-D in women only; restricted use (ischemic colitis risk) |
| Eluxadoline | Mixed opioid receptor agent | IBS-D; contraindicated in those without a gallbladder (pancreatitis risk) |
| Bile acid sequestrants | e.g., cholestyramine | For bile acid diarrhea subtype |
| TCAs (low-dose) | e.g., amitriptyline | For pain and diarrhea; central and peripheral mechanisms |
For IBS-C (constipation-predominant)
| Drug | Class | Notes |
|---|---|---|
| Linaclotide | Guanylate cyclase-C agonist | Reduces pain and increases secretion; first-line for IBS-C |
| Plecanatide | Guanylate cyclase-C agonist | Similar to linaclotide |
| Lubiprostone | Chloride channel activator | Stimulates intestinal fluid secretion |
| Tenapanor | NHE3 inhibitor | Reduces sodium/fluid absorption |
| Tegaserod | 5-HT4 agonist | Reintroduced in US for women <65 with IBS-C; limited cardiac history |
| Osmotic laxatives | PEG, lactulose | Improve stool consistency but not pain |
| SSRIs | Antidepressants | Improve global symptoms and constipation |
For Abdominal Pain/Cramps (all subtypes)
| Drug | Class | Notes |
|---|---|---|
| Antispasmodics | e.g., dicyclomine, hyoscine | 30 min before meals for postprandial pain; inhibit gastrocolic reflex |
| Low-dose TCAs | e.g., amitriptyline, nortriptyline | Central neuromodulation; best for IBS-D with pain |
| SNRIs/SSRIs | Antidepressants | Useful when comorbid depression/anxiety; SSRIs preferred in IBS-C |
| Peppermint oil | Smooth muscle relaxant | Reduces calcium influx; modest evidence for pain/bloating |
Step 4: Psychological/Brain-Gut Behavioral Treatments
A 2024 network meta-analysis (PMID 38777133) and a 2025 Lancet network meta-analysis (PMID 41077057) confirm behavioral therapies are effective for IBS:
| Therapy | Evidence |
|---|---|
| Cognitive Behavioral Therapy (CBT) | Strongest evidence; improves pain, quality of life |
| Gut-directed hypnotherapy | Well-evidenced; durable effects |
| Mindfulness-based therapy | Effective for pain and psychological comorbidity |
| Psychodynamic/interpersonal therapy | Effective in refractory cases |
Recommended especially in moderate-severe IBS with comorbid anxiety, depression, or when GI symptoms are closely linked to stress.
Prognosis
- IBS is a chronic, relapsing condition but is not associated with increased mortality or risk of IBD/colorectal cancer
- Subtypes can shift over time in the same patient
- ~30-40% of patients have symptom remission over years
- Quality of life impairment can be substantial
- Comorbid psychological disorders worsen prognosis
Sources: Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology 7e; Sleisenger & Fordtran's GI and Liver Disease
Recent evidence updates:
- Low-FODMAP diet is now the best-supported dietary intervention - superior to others in a 2025 network meta-analysis (PMID 40258374, Lancet Gastroenterol Hepatol)
- Brain-gut behavioral therapies (CBT, gut-directed hypnotherapy) confirmed effective in 2024-2025 network meta-analyses (PMID 38777133, PMID 41077057)
- Global IBS prevalence 4.1% by Rome IV in a 2025 meta-analysis of 2006-2024 data (PMID 40359286)
Liver hemangioma
Finding Sources
Searching PubMed
"hepatic hemangioma" diagnosis management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content with excellent imaging. Let me compile the full, well-structured answer.
Hepatic Hemangioma
Overview
Hepatic hemangioma is the most common benign liver lesion, occurring in 5-20% of the general population. It is a congenital vascular malformation - not a true neoplasm - comprising blood-filled cavernous spaces lined by a single layer of endothelial cells and separated by fibrous septa. The vast majority are found incidentally, are asymptomatic, and require no treatment.
Key reassuring facts:
- No malignant potential - there has never been a reported case of malignant degeneration
- Extremely low risk of spontaneous rupture or hemorrhage (in contrast to hepatic adenoma)
- Most remain stable or grow very slowly over time
Gross Pathology
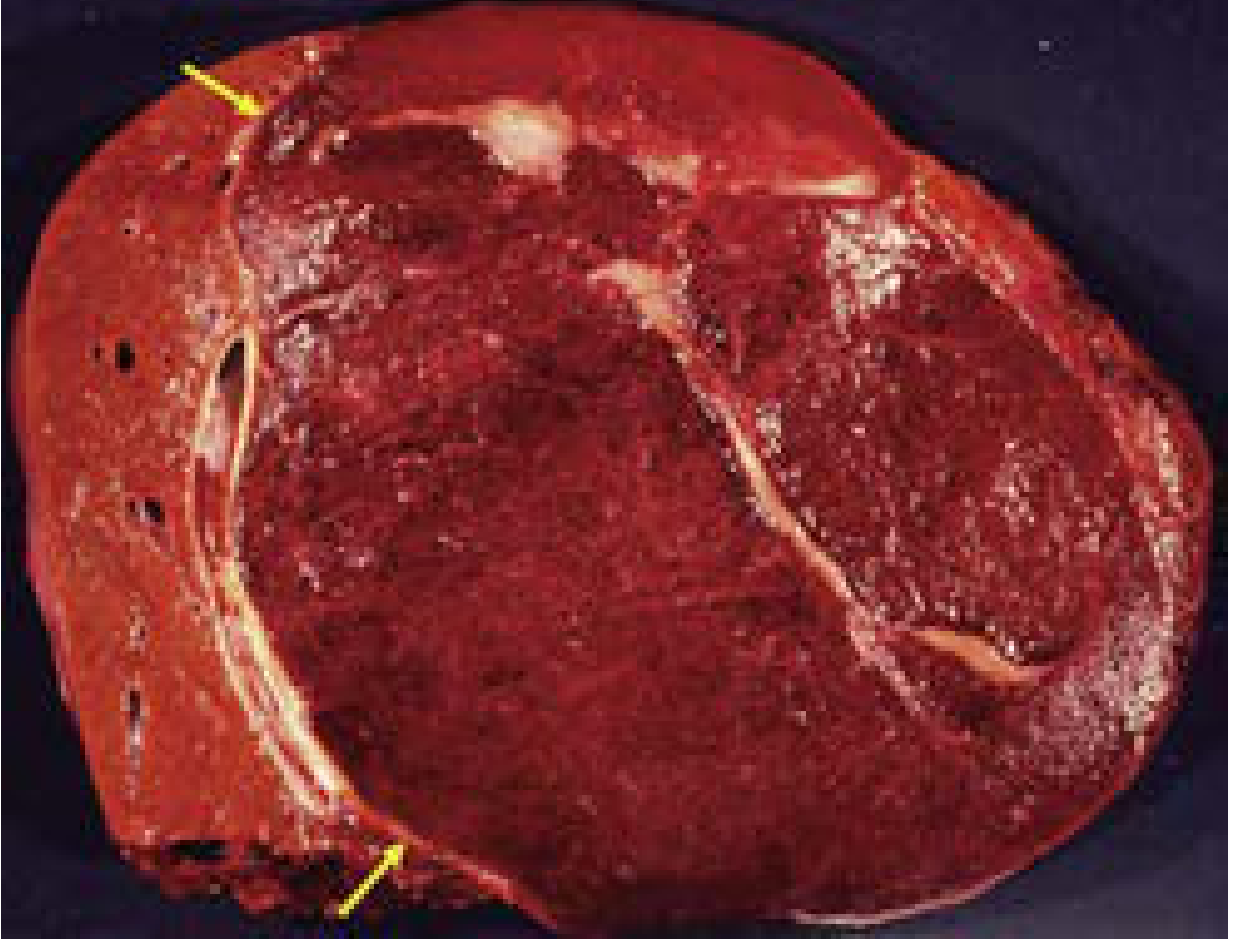
Gross specimen of hepatic hemangioma: dark red, spongy blood-filled lesion. Yellow arrows indicate the surrounding pseudocapsule, which is the dissection plane used for enucleation.
Microscopically:
- Cavernous vascular spaces filled with blood
- Single layer of flat endothelial cells lining each space
- Fibrous stroma separating the spaces
- May contain organizing thrombi or calcifications
- Surrounded by a pseudocapsule formed by compressed liver parenchyma (not a true capsule)
Epidemiology and Demographics
- Prevalence: 5-20% of the general population
- Predominant in women aged 20-50
- Most patients have a single lesion (90%); 10% have multifocal disease
- Size ranges from millimeters to >10 cm
- Giant hemangioma: currently defined as >10 cm (the threshold was previously 5 cm)
- No estrogen receptors identified, but estrogen exposure (e.g., oral contraceptives, pregnancy) may lead to higher rates of enlargement without increased rupture risk
Clinical Presentation
The vast majority are asymptomatic and found incidentally during imaging performed for unrelated reasons (e.g., trauma, nephrolithiasis, abdominal pain workup).
Symptoms (when present)
- Vague abdominal pain or discomfort
- Early satiety
- Nausea and vomiting
- Fullness or pressure sensation in the right upper quadrant
Proposed mechanism: distension and stretch of Glisson's capsule (which is innervated). However, the majority of patients with capsular involvement are still asymptomatic, and ~50% of patients presenting with symptoms attributed to a hemangioma will have an alternative cause found on thorough workup.
Rare Complications
| Complication | Features |
|---|---|
| Kasabach-Merritt syndrome | Thrombocytopenia + consumptive coagulopathy (hypofibrinogenemia, elevated FDPs) within a giant hemangioma; rare; more common in children |
| Biliary obstruction | From mass effect of giant hemangioma |
| Hepatic venous compression | Can cause Budd-Chiari syndrome; exceedingly rare |
| Spontaneous rupture/hemorrhage | Extremely rare; more common with trauma |
| Congestive heart failure (children) | From arteriovenous shunting in large childhood hemangiomas |
Imaging
Imaging is the cornerstone of diagnosis. Percutaneous biopsy is NOT recommended - it is potentially dangerous (bleeding risk), inaccurate, and rarely necessary.
Ultrasound
First-line, most cost-effective modality.
- Appearance: well-demarcated, homogeneous, hyperechoic (bright) lesion
- No posterior acoustic shadowing
- Most accurate for lesions <3 cm
- Contrast-enhanced ultrasound (CEUS): shows early peripheral nodular enhancement with progressive centripetal fill-in; avoids radiation and can be used when CT/MRI contrast is contraindicated
CT (Triple-phase/Multiphase)
Classic enhancement pattern - highly diagnostic:
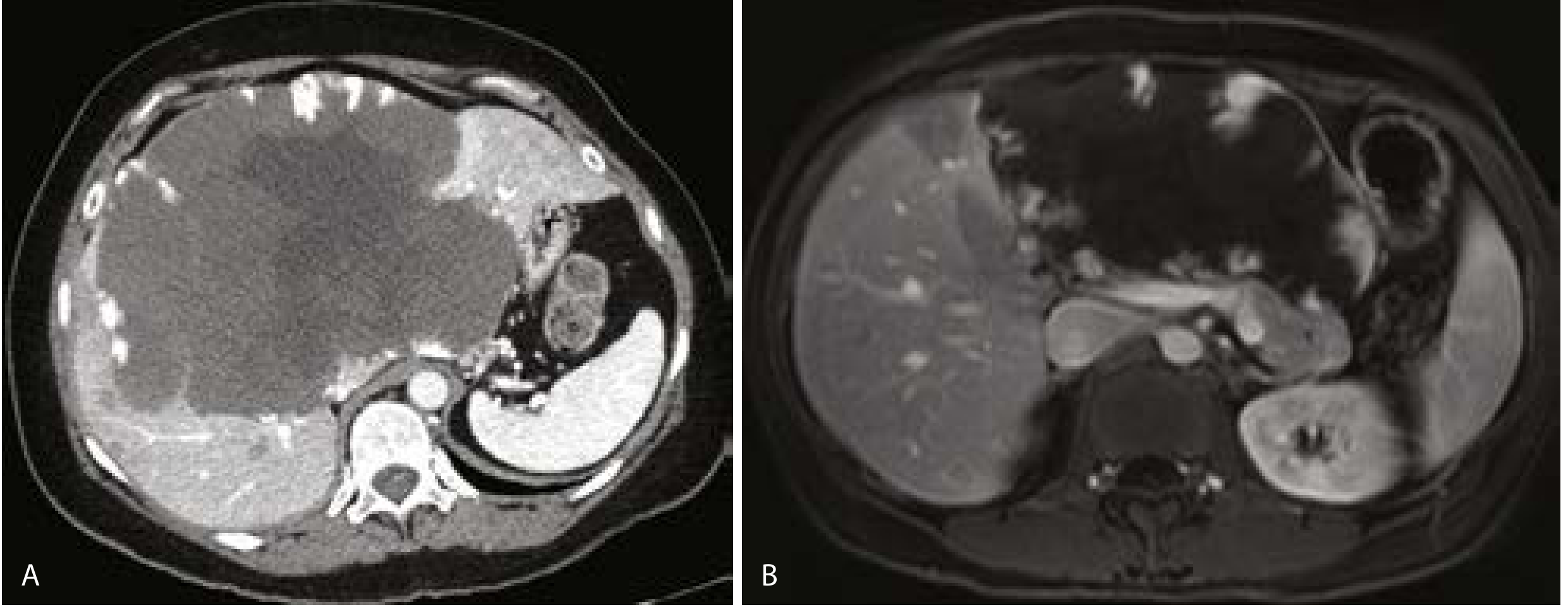
Left (CT arterial phase): large hepatic hemangioma showing peripheral nodular enhancement. Right (MRI post-gadolinium): corresponding MRI appearance.
Three diagnostic CT criteria:
- Pre-contrast: well-defined, hypodense (hypointense) lesion
- Arterial phase: early discontinuous peripheral nodular enhancement ("cotton wool" or "globular" enhancement)
- Venous/delayed phases: progressive centripetal fill-in - contrast moves from periphery inward - with eventual isodense or hyperdense appearance ("fill-in pattern")
Atypical patterns:
- Small hemangiomas (<1.5 cm) may fill in so rapidly that the nodular pattern is missed
- Large hemangiomas may show incomplete fill-in or central scarring/fibrosis
MRI
Most accurate modality (sensitivity ~90%, specificity approaching 100%). Used when US/CT is atypical or inconclusive.
| Sequence | Appearance |
|---|---|
| T1-weighted | Hypointense relative to liver |
| T2-weighted | Markedly hyperintense ("light bulb" sign - brighter than spleen or CSF-equivalent) |
| DWI | Hyperintense due to T2 shine-through |
| Post-gadolinium | Peripheral nodular enhancement with progressive centripetal filling (same as CT pattern) |
MRI with vascular contrast (gadolinium) is preferred over hepatobiliary contrast agents for hemangioma characterization.
Nuclear Medicine
- Technetium-99m-labeled red blood cell (RBC) scan: historically accurate but now rarely needed given high-quality CT/MRI availability
Summary: Imaging Algorithm
Incidentally found liver lesion
↓
Ultrasound (first-line)
Typical hyperechoic lesion < 3 cm in healthy patient?
↓ Yes ↓ Atypical / >3 cm / known malignancy
Diagnosis secure Multiphase CT or MRI
No further workup needed ↓
MRI most accurate
(sensitivity 90%, specificity ~100%)
↓ Still uncertain
CEUS or surgical/biopsy
Differential Diagnosis
| Lesion | Key distinguishing features |
|---|---|
| Hepatocellular carcinoma (HCC) | Arterial hyperenhancement + washout on delayed phase; elevated AFP; cirrhotic background |
| Metastasis | Known primary malignancy; may be hypo- or hyperechoic; lacks typical centripetal fill |
| Hepatic adenoma | Young women on OCP; risk of hemorrhage; arterial enhancement without centripetal fill |
| Focal nodular hyperplasia (FNH) | Central scar on MRI; hepatobiliary phase uptake; T2 isoechoic |
| Cholangiocarcinoma | Peripheral washout; associated ductal dilation |
| Sclerosed hemangioma | Atypical US/CT/MRI appearance; may require resection for diagnosis |
Management
The overriding principle: >90% of patients require no treatment, regardless of size.
Four Key Management Principles (Current Surgical Therapy, 14e)
- The majority of hemangiomas, regardless of size, are asymptomatic and do not require intervention
- Always consider a broad differential for symptoms in patients with incidentally found hemangioma - an alternative etiology is found in ~50% of cases
- The ability to perform minimally invasive resection should not expand the indications for surgery
- Operative treatment fails to improve symptoms in approximately 30-50% of carefully selected symptomatic patients
Observation (Standard for Most)
Indications for observation only:
- Asymptomatic patients with secure diagnosis - no surveillance needed
- Asymptomatic patients regardless of lesion size
- Women of childbearing age - no need to stop OCP or modify pregnancy plans
- Small (<5 cm) lesions with typical imaging features
Routine surveillance imaging is not warranted in asymptomatic patients with a confirmed hemangioma.
For diagnostic uncertainty or larger lesions (>5 cm), follow-up imaging in 3-6 months is reasonable.
Indications for Treatment (Narrow)
Treatment is only considered for:
- Severe persistent symptoms with no other identifiable etiology after thorough workup
- Intraparenchymal or intraperitoneal hemorrhage (exceedingly rare; often associated with Kasabach-Merritt)
- Biliary obstruction or hepatic venous compression (Budd-Chiari)
- Diagnostic uncertainty with inability to exclude malignancy
Surgical Treatment
Option 1 - Enucleation (preferred when technically feasible)
- Exploits the pseudocapsule as a natural dissection plane
- Incise Glisson's capsule adjacent to tumor, develop the peritumoral plane
- Preserves maximum functional liver parenchyma
- Vascular structures are displaced (not invaded) and can be preserved
- Associated with lower postoperative complication rates vs. formal resection
- Best for sublobar, peripheral hemangiomas
Option 2 - Anatomic resection
- Necessary for lobar hemangiomas or those involving central hepatic structures
- Ipsilateral hepatic artery ligation facilitates decompression
- Preoperative arterial embolization (day before) may be used for massive lesions
General surgical principles:
- Low central venous pressure anesthesia
- Pringle maneuver (hepatic inflow occlusion) for visualization
- Cell salvage/autotransfusion
- Laparoscopic or robotic approach preferred when feasible
- Operative mortality: <1%
Non-surgical Interventions
| Modality | Role |
|---|---|
| Hepatic arterial embolization | Preoperative (reduce intraoperative bleeding in giant hemangiomas) or palliative in non-surgical candidates; does NOT cure |
| Radiofrequency ablation (RFA) | Reported in selected cases; limited evidence |
| Radiation therapy | Historically used; now rarely employed |
| Liver transplantation | Exceptional cases with unresectable symptomatic giant hemangiomas |
Pediatric Hemangiomas
- Account for ~12% of all childhood hepatic tumors
- Usually multifocal; may involve other organs
- Large lesions can cause congestive heart failure (arteriovenous shunting)
- Untreated symptomatic childhood hemangiomas carry high mortality
- Small capillary hemangiomas: almost all spontaneously resolve
- Treatment: embolization for symptoms; medical therapy for CHF; resection for rupture or failure of conservative measures
Lab Values
- LFTs: usually normal
- Tumor markers (AFP, CEA, CA19-9): normal
- In Kasabach-Merritt: thrombocytopenia, elevated FDPs, hypofibrinogenemia, prolonged clotting times
Prognosis and Natural History
- Benign course in the vast majority
- Most remain stable; slow growth may occur
- No malignant transformation - ever
- Spontaneous rupture: exceedingly rare
- Estrogen exposure may accelerate enlargement but does not increase rupture risk
- Excellent surgical outcomes when intervention is needed (mortality <1%)
Sources: Current Surgical Therapy 14e; Sabiston Textbook of Surgery; Sleisenger & Fordtran's GI and Liver Disease
Recent literature: A 2022 systematic review (PMID 35705835) confirms the conservative management approach with surgery reserved for truly symptomatic cases. A 2024 imaging review (PMID 38541175) highlights the growing role of CEUS as an alternative to CT/MRI for characterization, reducing radiation exposure.
This is a shared conversation. Sign in to Orris to start your own chat.