Hemorrhage (Bleeding). Definition. Classification. Clinical features.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough, well-illustrated response. Let me compile the full answer.
Hemorrhage (Bleeding)
Definition
Hemorrhage is defined as the extravasation (escape) of blood from the cardiovascular system - i.e., from blood vessels into the surrounding tissues, body cavities, or outside the body entirely.
It results from damage to blood vessel walls and may be exacerbated by defects in blood clotting (coagulopathy). Although capillary bleeding can occur in chronically congested tissues, significant hemorrhage typically requires trauma, atherosclerotic erosion, inflammatory/neoplastic vessel wall destruction, or a coagulation disorder. The risk of hemorrhage after even minor injury is significantly elevated in conditions collectively termed hemorrhagic diatheses, which include inherited or acquired defects in vessel walls, platelets, or coagulation factors.
Robbins & Kumar Basic Pathology - "Hemorrhage, defined as the extravasation of blood from vessels, results from damage to blood vessels and may be exacerbated by defects in blood clotting."
Classification
Hemorrhage can be classified across several dimensions:
1. By Location / Form
| Type | Description |
|---|---|
| External hemorrhage | Blood escapes the body surface (wound, GI tract, respiratory tract, etc.) |
| Internal hemorrhage / Hematoma | Blood accumulates within tissues. Ranges from trivial (bruise) to fatal (retroperitoneal hematoma from aortic rupture) |
| Hemothorax | Blood in the pleural cavity |
| Hemopericardium | Blood in the pericardial sac |
| Hemoperitoneum | Blood in the peritoneal cavity |
| Hemarthrosis | Blood in a joint space |
2. By Size of Cutaneous/Mucosal Hemorrhage
| Term | Size | Characteristics |
|---|---|---|
| Petechiae | 1-2 mm | Pinpoint hemorrhages into skin, mucous membranes, or serosal surfaces. Caused by thrombocytopenia, defective platelet function, or loss of vascular wall support (e.g., scurvy) |
| Purpura | 3-5 mm | Slightly larger. Causes overlap with petechiae; also seen in vasculitis, trauma, and increased vascular fragility |
| Ecchymosis | 1-2 cm | Subcutaneous hematomas ("bruises"). Extravasated RBCs undergo enzymatic degradation: hemoglobin (red-blue) → bilirubin (blue-green) → hemosiderin (golden-brown) - accounting for the characteristic color changes |
3. By Rate (Acuity)
- Acute hemorrhage - rapid, large-volume blood loss (e.g., traumatic arterial injury, ruptured aneurysm)
- Chronic/recurrent hemorrhage - slow or intermittent blood loss (e.g., peptic ulcer, menstrual bleeding) leading to iron deficiency anemia from hemoglobin-iron loss. Note: internal bleeds (hematomas) do NOT cause iron deficiency because iron is efficiently recycled from phagocytosed RBCs.
4. By Source (Vessel Type)
- Arterial - bright red, pulsatile, high pressure, life-threatening
- Venous - dark red, continuous flow, lower pressure
- Capillary - oozing, often self-limiting
5. ATLS Classification of Hemorrhagic Shock (American College of Surgeons)
This is the most clinically used classification, based on a 70-kg adult with ~5 L blood volume:
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | Up to 750 | 750-1,500 | 1,500-2,000 | >2,000 |
| Blood loss (% vol) | Up to 15% | 15-30% | 30-40% | >40% |
| Heart rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >40 |
| Urine output (mL/hr) | >30 | 20-30 | 5-15 | Negligible |
| Mental status | Slightly anxious | Mildly anxious | Confused | Lethargic |
- Class I: minimal - self-compensated
- Class II: mild - usually managed with crystalloid
- Class III: moderate - requires blood transfusion
- Class IV: life-threatening - immediate transfusion + surgical/interventional control
(Mulholland and Greenfield's Surgery, 7e; Rockwood and Green's Fractures in Adults, 10e)
Clinical Features
Local / Morphological Features
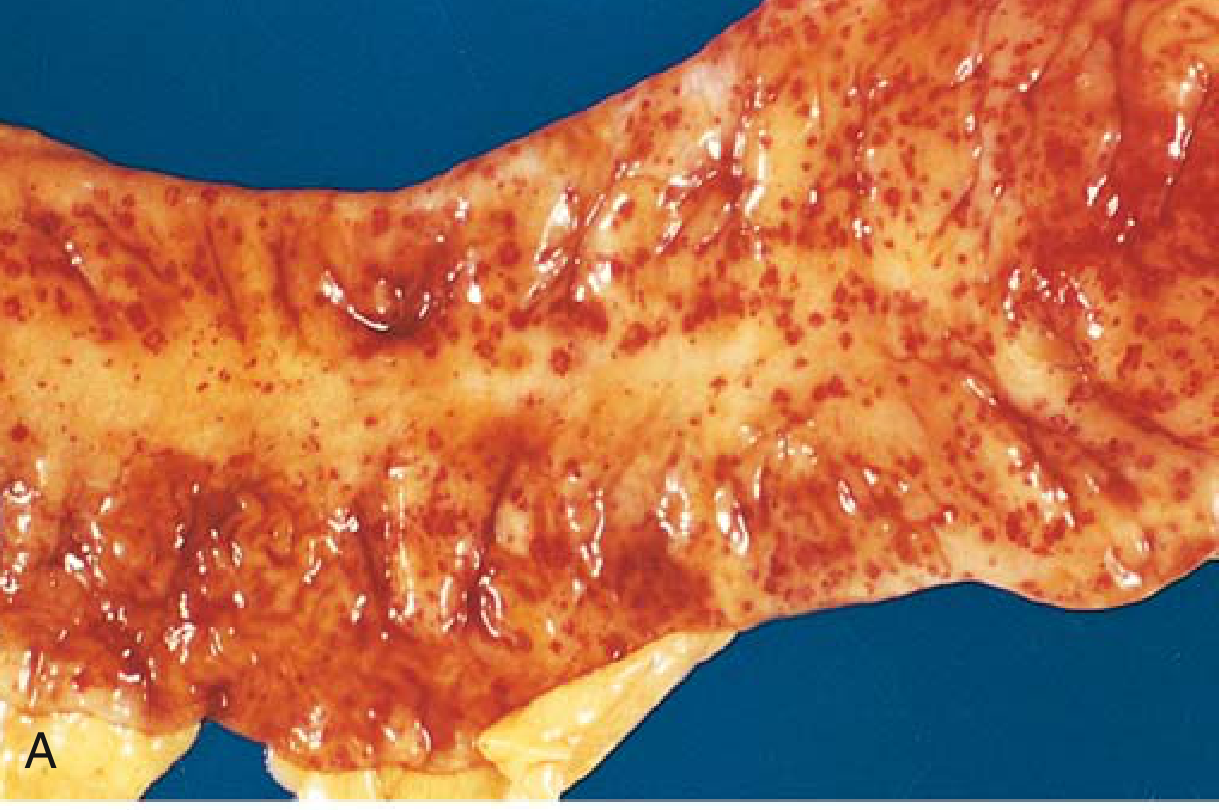
Petechial hemorrhages (colonic mucosa in thrombocytopenia):
Fatal intracerebral hemorrhage (a bleed trivial in subcutaneous tissue may be fatal in the brain):
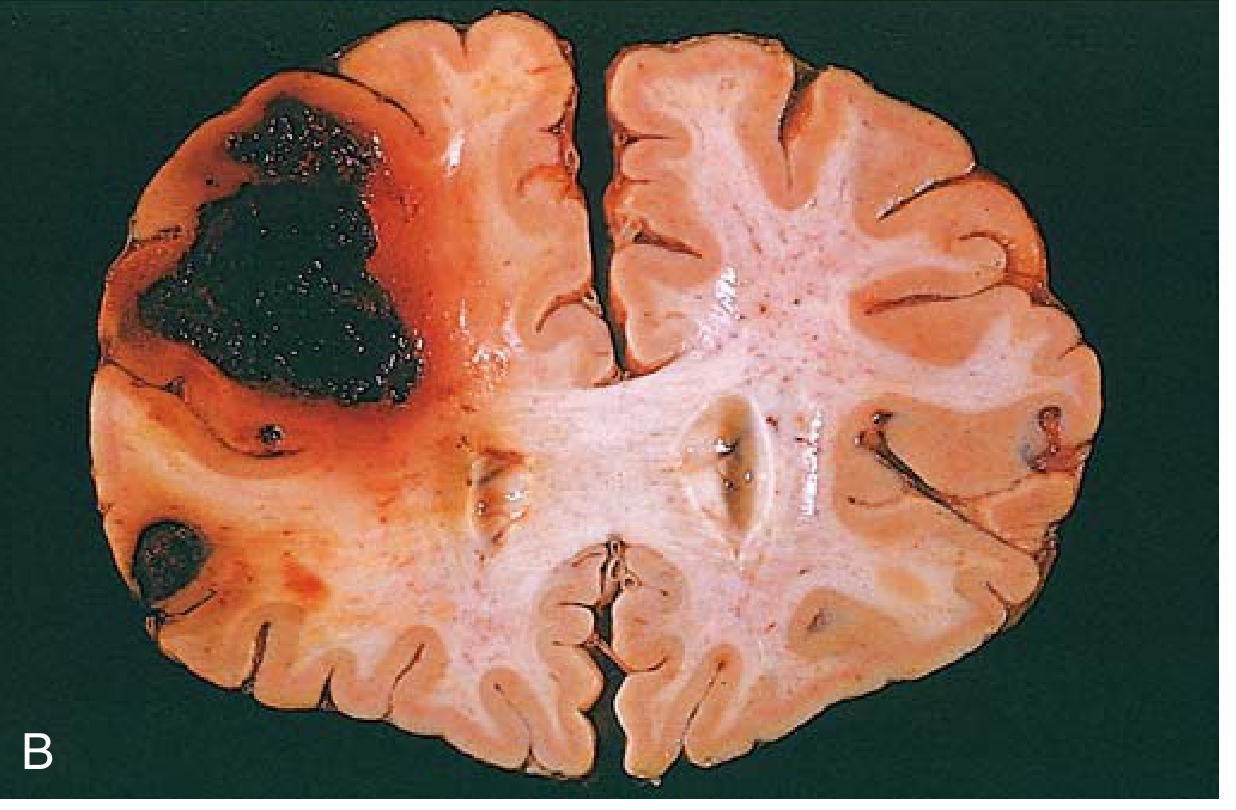
FIG. 3.4 (A) Punctate petechial hemorrhages of the colonic mucosa in thrombocytopenia. (B) Fatal intracerebral hemorrhage. - Robbins & Kumar Basic Pathology
Systemic Clinical Features
The clinical impact depends on four key factors:
- Volume of blood lost
- Rate of bleeding
- Location of the bleed
- Pre-existing health status
Cardiovascular signs:
- Tachycardia (early compensatory response)
- Hypotension (systolic BP falls significantly at Class III, >30% loss)
- Narrowed pulse pressure (reduced stroke volume + increased peripheral resistance)
- Weak, thready pulse in severe hemorrhage
Respiratory signs:
- Tachypnea (compensatory, to improve O2 delivery)
- Increased depth of breathing
Neurological/Mental status:
- Anxiety, restlessness (early - catecholamine release)
- Confusion, combativeness (Class III)
- Lethargy, obtundation (Class IV)
Peripheral perfusion:
- Skin: pale, cool, clammy (vasoconstriction to maintain core perfusion)
- Delayed capillary refill (>2 seconds)
- Cold extremities
Renal:
- Reduced urine output (oliguria: 20-30 mL/hr in Class II; <5 mL/hr in Class IV)
Other systemic effects:
- Hemorrhagic (hypovolemic) shock - rapid loss of >20% blood volume can cause cardiovascular decompensation even in healthy adults
- Jaundice - large hemorrhages can occasionally cause jaundice as RBCs are phagocytosed and hemoglobin is degraded to bilirubin by macrophages
- Iron deficiency anemia - chronic external blood loss (peptic ulcer, menorrhagia) leads to iron depletion since hemoglobin-iron is not recovered
- Death - even modest bleeds in critical locations (e.g., intracerebral, pericardial tamponade) can be rapidly fatal
Individual Variation
Clinical presentation varies considerably based on:
- Age (elderly may have attenuated sympathetic response; young patients may compensate until abrupt collapse)
- Pre-existing disease (cardiac/respiratory disease worsens tolerance)
- Medications (beta-blockers blunt tachycardic response; anticoagulants worsen bleeding)
- Pregnancy (increased blood volume alters thresholds)
Sources:
- Robbins & Kumar Basic Pathology, p. 82 (Hemorrhage, Petechiae, Purpura, Ecchymosis, Clinical Impact)
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e, p. 530-531 (ATLS Classification of Hemorrhagic Shock)
- Rockwood and Green's Fractures in Adults, 10e, p. (Table 14-2, Classification for Hemorrhagic Shock)
- Goldman-Cecil Medicine, p. (Hemorrhage in upper GI bleeding)
Hemorrhage (Bleeding) in Surgery. Definition. Classification. Clinical features.
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.