Tb of kidney radiology rguhs pg ans
renal tuberculosis radiology RGUHS PG exam answer imaging features IVU USG CT
https://radiopaedia.org/articles/renal-tuberculosis?lang=us
https://pmc.ncbi.nlm.nih.gov/articles/PMC3737619
https://rcastoragev2.blob.core.windows.net/d549234ecca0b4413…
Radiology of Renal Tuberculosis (TB of Kidney) - RGUHS PG Answer
Introduction
Radiological Investigations
1. Plain X-ray KUB (Kidney, Ureter, Bladder)
- Lobar (lobular) calcification - pathognomonic of end-stage renal TB. Calcium deposits follow the lobar architecture of the kidney ("putty kidney" or autonephrectomy pattern)
- Scattered intraparenchymal calcifications or "pseudo-calculi" (calcified caseous material)
- Ureteral calcification (intramural, in nondilated ureters - distinguishes from schistosomiasis where calcified ureters are dilated)
- Calcified psoas abscess (in cases with perinephric spread)
- Renal calculi have higher incidence in TB
Key sign: Lobar pattern of calcification is pathognomonic of end-stage/healed renal TB on plain film
2. Intravenous Urography (IVU) / CT Urogram
Early Changes:
| Finding | Description |
|---|---|
| Loss of calyceal sharpness | Earliest change - mucosal edema causes minor calyceal blurring |
| Calyceal dilatation | Minimal dilatation of minor calyces |
| Papillary necrosis | Irregular, fuzzy, "moth-eaten" calyceal outline |
| "Feathery" or "frayed" calyces | Due to contrast tracking into necrotic papilla |
Late/Advanced Changes:
| Finding | Description |
|---|---|
| Cavitation | Calyceal cavity communicating with parenchyma |
| Phantom calyx | Non-visualization of a calyx due to infundibular stricture |
| Uneven caliectasis | Multiple calyces dilated to varying degrees (pathognomonic combination) |
| Infundibular strictures | Multiple pelvi-infundibular narrowings |
| "Hiked-up" renal pelvis | Upward displacement due to polar scarring |
| Autonephrectomy | Non-functioning kidney with lobar calcification (end stage) |
| Perinephric abscess | Mass effect, deviation of ureter |
Ureteral Changes (IVU):
- Multiple ureteric strictures (commonest finding after calyceal changes)
- "Beaded" or "corkscrew" ureter
- Ureteral calcification (in nondilated ureter - unlike schistosomiasis)
- Hydronephrosis/hydroureter distal to stricture
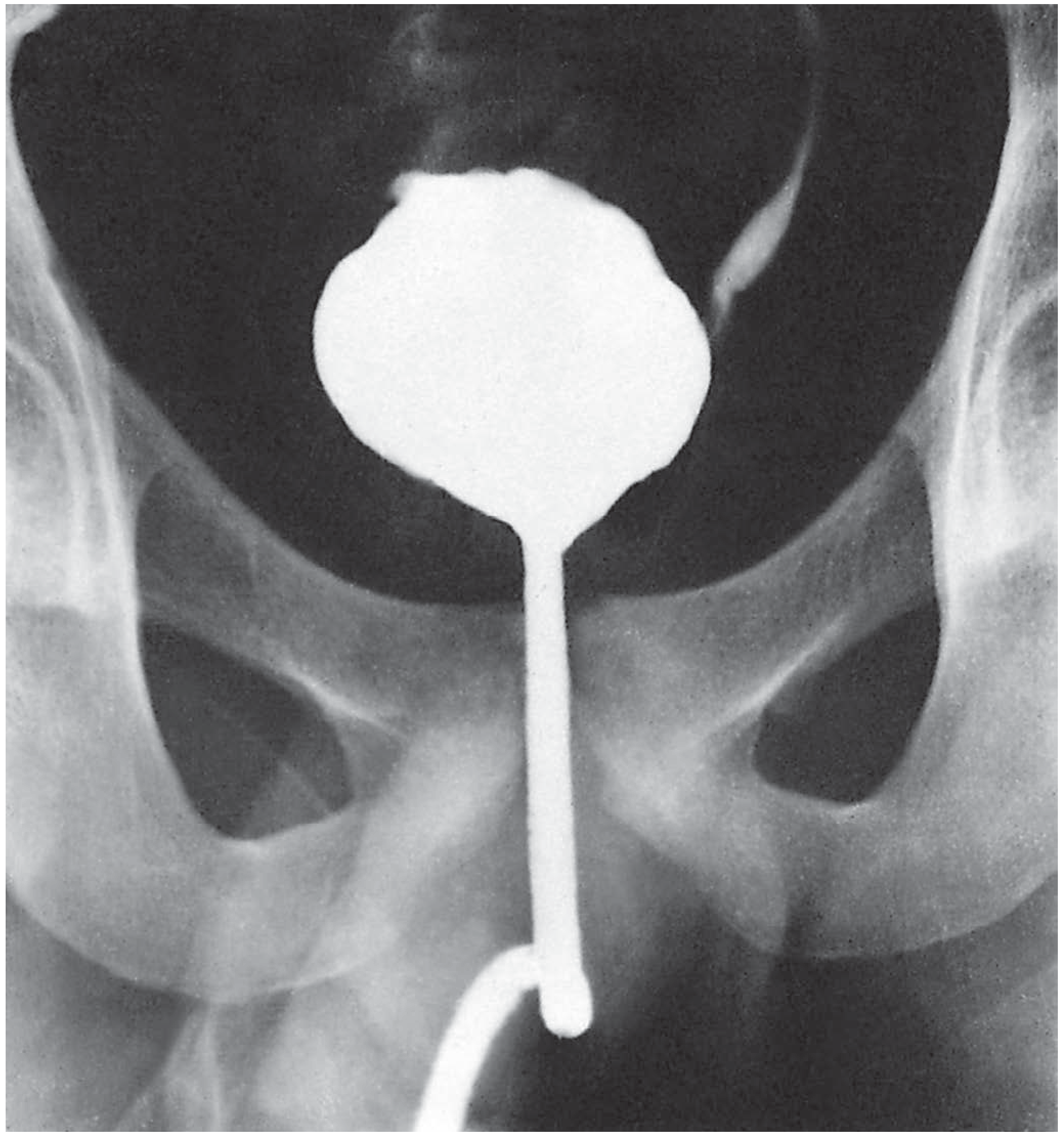
Bladder (Cystogram):
- Reduced bladder capacity - "Thimble bladder" (contracted fibrosed bladder) - classic late finding
- Irregular bladder wall with filling defects (ulcers/tubercles initially around ureteric orifices and trigone)
3. Ultrasonography (USG)
| Pattern | Features |
|---|---|
| Infiltrative pattern (more common) | Increased parenchymal echogenicity, calcifications with shadowing, loss of corticomedullary differentiation |
| Mass/granuloma pattern | Solid hypoechoic/isoechoic parenchymal mass (may be missed if isoechoic) |
| Cavities | Hypoechoic/complex cystic areas in parenchyma |
| Urothelial thickening | Thickened calyceal/pelvic walls |
| Lobar caseation | Hyperechoic solid wedge-shaped lesion in a renal lobe |
| Uneven caliectasis without pelvic dilatation | Characteristic USG finding in TB |
| Normal sonogram + non-functioning kidney on IVU | Classic combination suggesting TB (parenchymal infiltration without gross distortion) |
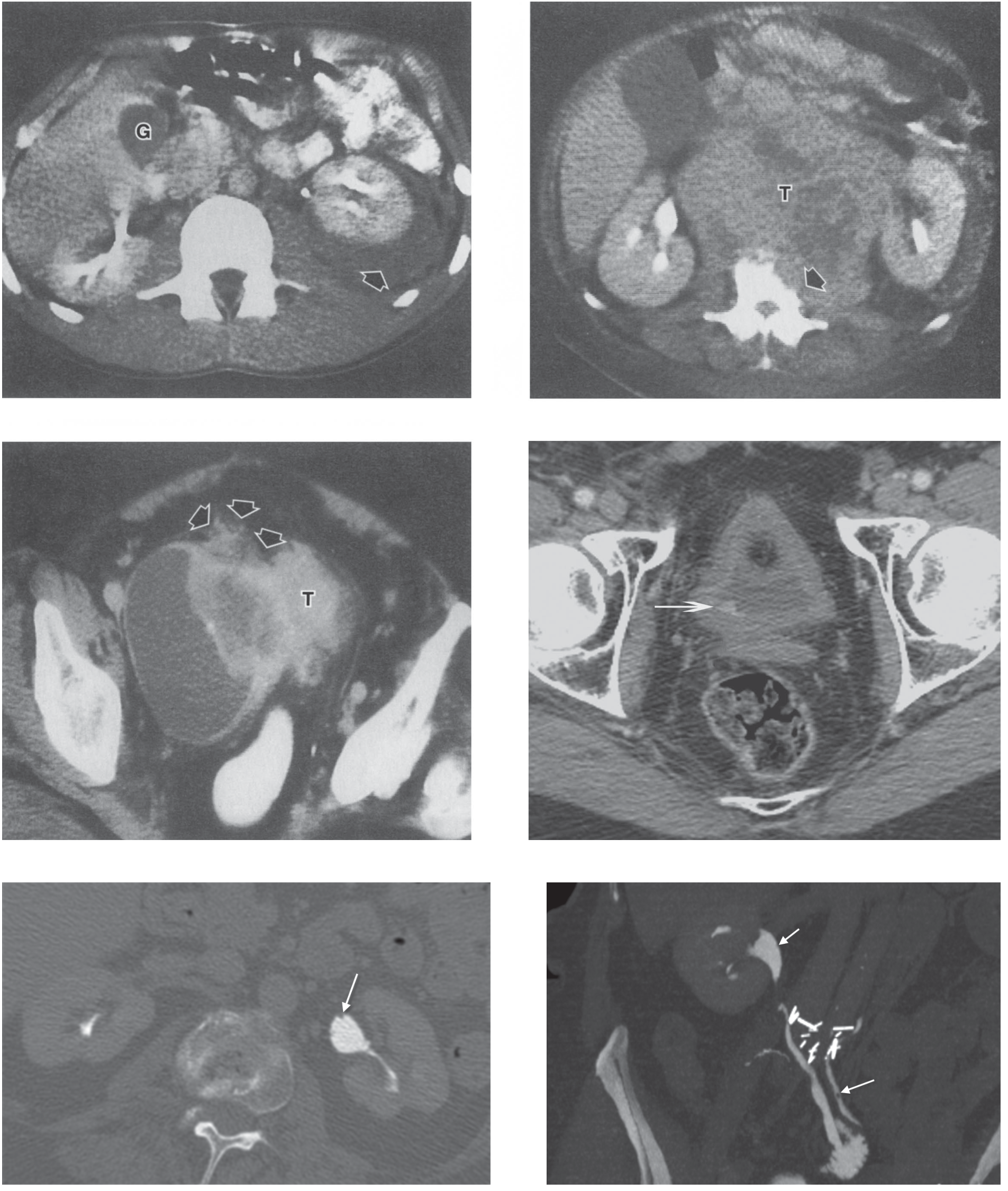
4. CT Scan (CT Urogram / MDCT)
| Feature | Detail |
|---|---|
| Parenchymal calcifications | Punctate, lobar, or diffuse ("dystrophic" calcification) |
| Lobar caseation | Low-density wedge-shaped parenchymal lesion with post-contrast rim enhancement |
| Cavities | Hypodense cavities with irregular walls; communication with collecting system |
| Infundibular/ureteric strictures | Well demonstrated on CT urogram - multiple sites |
| Uneven caliectasis | Varying degrees of calyceal dilatation |
| Renal scars | Cortical scarring at sites of healed infection |
| Urothelial thickening | Circumferential wall thickening with post-contrast enhancement of calyces, pelvis, ureter |
| Hydronephrosis / pyonephrosis | Dilated collecting system with dependent debris |
| Perinephric spread | Perinephric stranding, abscess, psoas abscess, fistula |
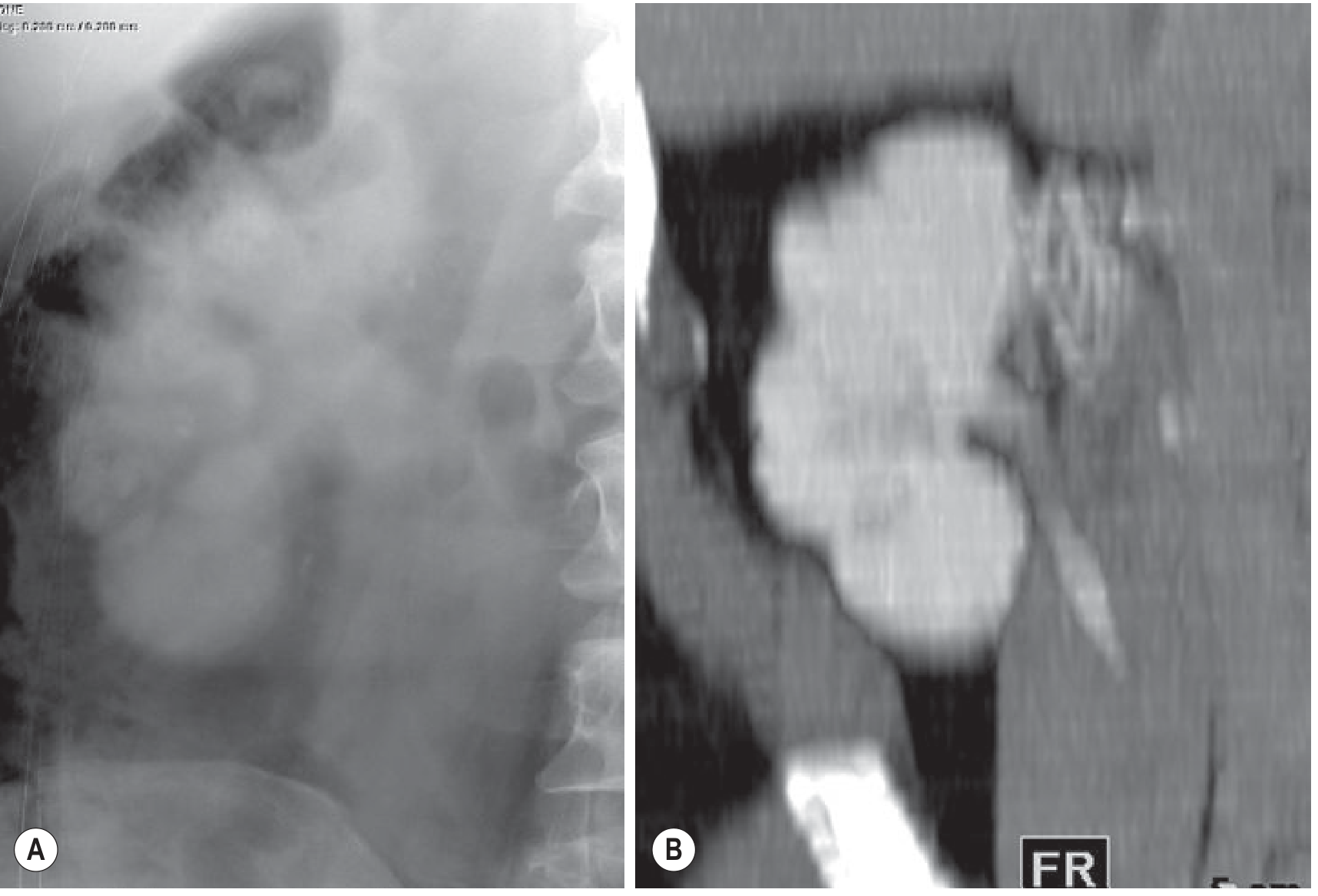
| Autonephrectomy | Completely calcified, non-enhancing kidney ("putty kidney") |
Key CT advantage: CT identifies calcifications, renal scars, and urothelial lesions better than any other modality; can substitute for retrograde pyelography when ureteric orifice is strictured.
5. MRI
- Limited role compared to CT
- Useful when CT is contraindicated (e.g., contrast allergy, pregnancy)
- T2W: Hyperintense cavities; low signal calcifications
- Post-gadolinium: Enhancement of urothelium and granulomas
- Diffusion-weighted imaging (DWI): Restricted diffusion in granulomas
6. Nuclear Medicine (DMSA Scan)
- Assesses differential renal function
- Important before deciding on nephrectomy (function <10-15% in affected kidney = poor prognosis)
- Shows reduced uptake in areas of scarring/non-function
Summary: Radiological Staging (IVU/CT)
| Stage | Findings |
|---|---|
| Early | Calyceal blurring, papillary necrosis, minor calyceal dilatation |
| Moderate | Cavitation, phantom calyx, infundibular strictures |
| Advanced | Uneven caliectasis, ureteric strictures, cortical scars |
| End-stage | Autonephrectomy, putty kidney (lobar calcification), thimble bladder |
Pathognomonic Signs (High-Yield for RGUHS)
| Sign | Modality | Significance |
|---|---|---|
| Lobar calcification | Plain X-ray | Pathognomonic of end-stage TB |
| Moth-eaten calyx | IVU | Papillary necrosis - earliest calyceal change |
| Phantom calyx | IVU/CT | Infundibular stricture with non-visualization |
| Thimble bladder | Cystogram/CT | Contracted fibrosed bladder - late TB |
| Putty kidney | Plain X-ray | Complete dystrophic calcification = autonephrectomy |
| Uneven caliectasis without pelvic dilatation | USG/CT | Characteristic of TB (vs. obstruction) |
References
- Bailey and Love's Short Practice of Surgery, 28th Edition (GUTB chapter)
- Merchant S, et al. "Tuberculosis of the genitourinary system - Urinary tract tuberculosis: Part I & II." Indian Journal of Radiology and Imaging, 2013
Use onlt standard radiology tectbooks and do only tb of kidney
Radiology of Tuberculosis of the Kidney
Introduction & Pathogenesis
General Imaging Principles
- Papillary necrosis and parenchymal destruction
- Presence of three or more of the following is highly suggestive of TB:
- Pelvicalyceal thickening
- Ulceration
- Fibrosis with or without stricture
- Calcification occurs in 40-70% of cases
Modality-by-Modality Imaging Findings
1. Plain Radiograph (X-ray KUB)
- Renal calcification - may be focal, multifocal, or complete
- Putty kidney (end-stage): reniform-shaped radio-opaque calcified mass occupying the entire kidney - dystrophic calcifications fill the entire non-functioning kidney
2. Intravenous Urography (IVU) / Excretory Urography
- Loss of calyceal sharpness (mucosal oedema)
- Minor calyceal dilatation
- Papillary necrosis - moth-eaten appearance of calyces (contrast tracks into necrotic papilla)
- Infundibular strictures - obstruct renal segments, creating phantom calyx against a background of normal renal tissue
- Strictures distort the collecting system, creating cavities and contour deformities
- Ureteric strictures (multiple sites, beaded/corkscrew appearance)
- Hydronephrosis / hydroureter
- Poor or non-functioning kidney (autonephrectomy)
- Calcification - thin rim around a necrotic area or complete parenchymal replacement
- Autonephrectomy - completely non-functioning calcified kidney
- IVU can detect parenchymal calcification, cavitary lesions, infundibular stenosis with amputated calyces, or pelvicalyceal stenosis with hydronephrosis
Note: CT is not as sensitive as excretory urography for detecting early urothelial changes
3. Computed Tomography (CT) - Investigation of Choice
| Finding | Detail |
|---|---|
| Striated nephrogram | Reactivated disease causes inflammation and vasoconstriction → hypoperfusion → striated pattern on contrast-enhanced CT |
| Papillary necrosis | Moth-eaten calyceal appearance |
| Parenchymal calcification | Focal, lobar, or complete (dystrophic) |
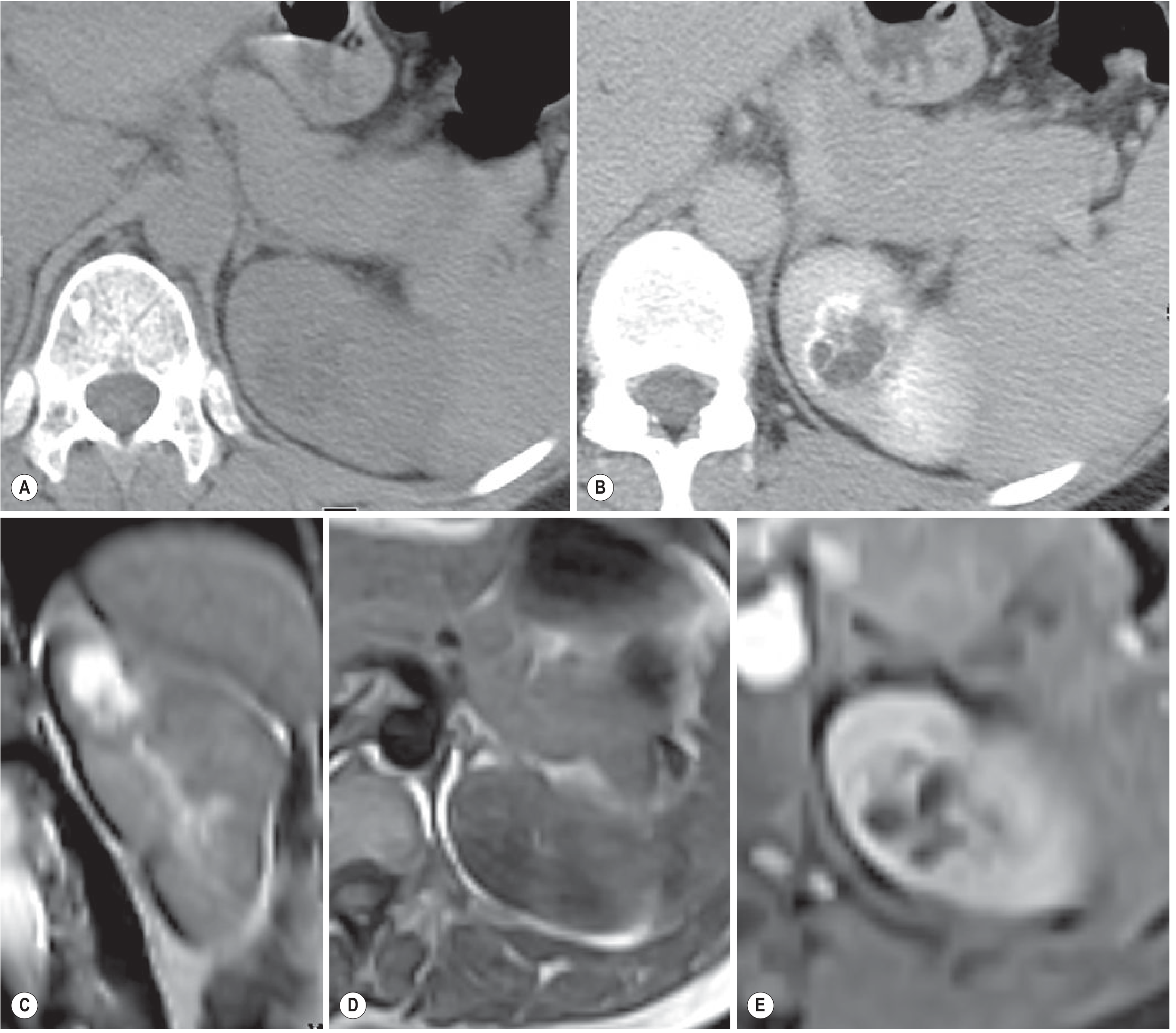
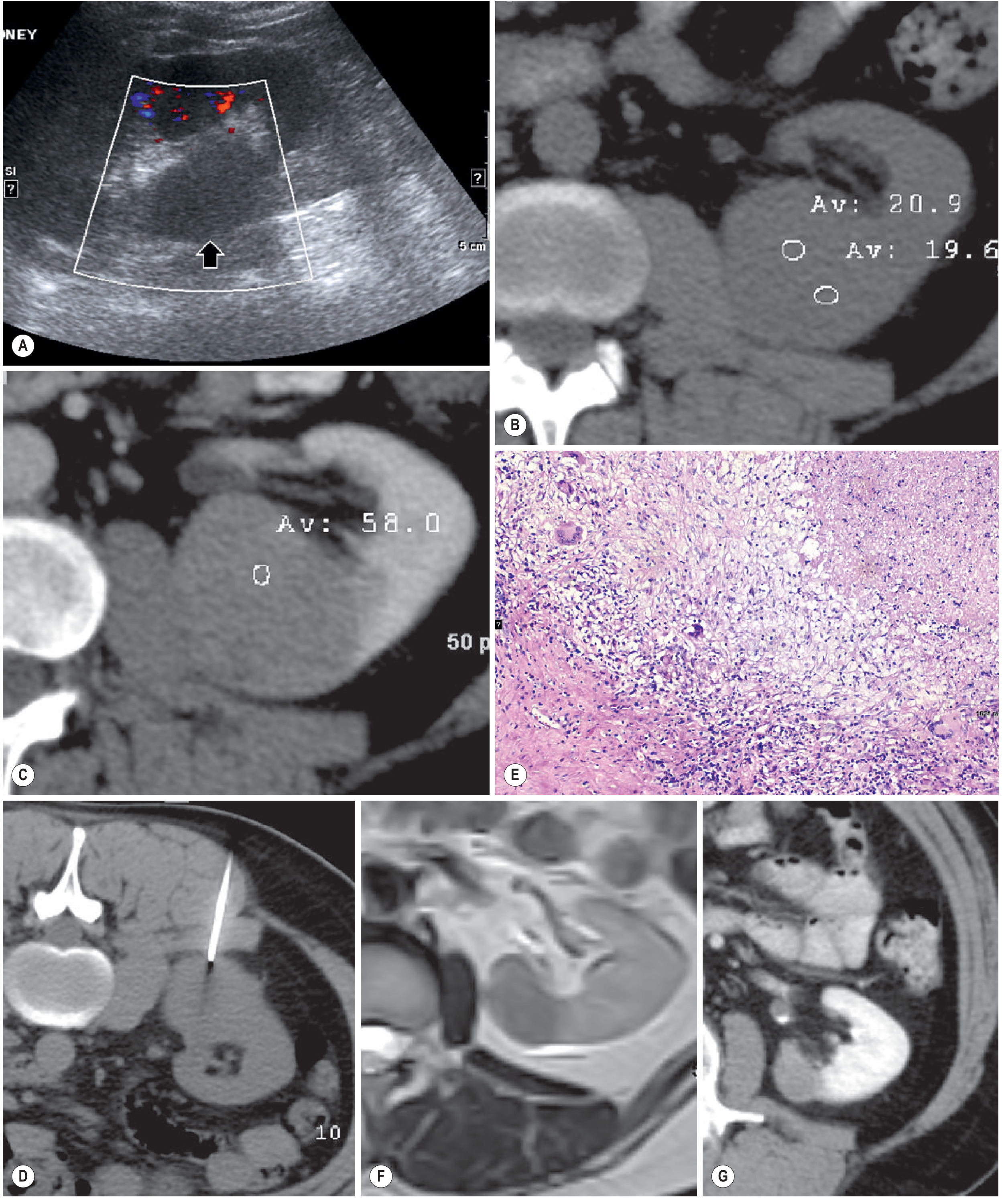
| TB granulomas | Hypodense lesions with caseous material or calcification; mild rim enhancement on post-contrast CT |
| Infundibular/ureteric strictures | Fibrotic strictures of infundibula, renal pelvis, and ureters - highly suggestive of TB |
| Phantom calyx | Calyx not opacified due to infundibular stricture |
| Cavities | Hypodense cavities communicating with collecting system |
| Contour deformities/scarring | Parenchymal thinning and cortical scars |
| Uneven caliectasis | Varying degrees at different sites due to fibrosis |
| Autonephrectomy | Non-functioning kidney with complete calcification |
| Putty kidney | Hyperdense calcific material filling dilated calyces and upper ureter on unenhanced CT |
| Perinephric spread | Perinephric stranding, abscess, fistula, retroperitoneal involvement |

4. Ultrasonography (USG)
- Focal hyperechoic or hypoechoic renal masses (granulomas/tuberculomas)
- Diffuse parenchymal hyperechogenicity from calcification
- Renal abscess formation
- Loss of corticomedullary differentiation
- Urothelial thickening of the collecting system
- Hydronephrosis
- A lesion may be missed if isoechoic to the parenchyma
Limitation: USG is less sensitive than IVU or CT for subtle urothelial changes and early calcification
5. Magnetic Resonance Imaging (MRI)
- Depicting TB cavities, sinus tracts, and fistulous communications
- Assessing extrarenal spread
- T1W: Hypointense (lesion); may be isointense to parenchyma
- T2W: Thick, irregular, hypointense peripheral wall with intralesional fluid-debris level
- Post-Gd contrast: Rim enhancement and subtle internal septal enhancement
- TB granulomas appear as mildly enhancing soft-tissue masses
End-Stage Renal TB: Putty Kidney / Autonephrectomy
| Term | Description | Modality |
|---|---|---|
| Putty kidney | Reniform mass with complete calcification of a non-functioning kidney | Plain X-ray + CT |
| Autonephrectomy | Completely calcified non-functioning kidney | CT: hyperdense calcific material filling dilated calyces and upper ureter |
High-Yield Summary for RGUHS
| Sign | Modality | Significance |
|---|---|---|
| Moth-eaten calyx | IVU/CT | Papillary necrosis - earliest calyceal change |
| Phantom calyx | IVU/CT | Infundibular stricture, non-visualised calyx |
| Striated nephrogram | Contrast CT | Reactivated TB (hypoperfusion) |
| Fibrotic infundibular/ureteric strictures | IVU/CT | Highly suggestive of TB |
| Rim-enhancing granuloma | CT/MRI | Caseous TB granuloma |
| Putty kidney / Autonephrectomy | Plain X-ray/CT | End-stage renal TB |
| T2 hypointense peripheral wall + fluid-debris | MRI | Macronodular tuberculoma |
| Sterile pyuria + calcification | Clinical + imaging | Classic TB combination |
Key point (Grainger & Allison): "The presence of three or more of the following is highly suggestive of TB: pelvicalyceal thickening; ulceration; and fibrosis with or without stricture."
Tb of ureter bladder and urethra radiology my style
TB of Ureter, Bladder and Urethra - Radiology
TUBERCULOSIS OF THE URETER
Pathological basis
Plain X-ray KUB
- Ureteral calcification - intramural, in a nondilated ureter
This distinguishes TB from schistosomiasis (where the calcified ureter is dilated)
- Faint upper ureteral calcification alongside any renal calcification = good marker of renal TB
IVU / CT Urogram - Ureteric Findings
| # | Sign | Description |
|---|---|---|
| 1 | Irregular ureter | Mucosal irregularity from granulomatous ulceration |
| 2 | Corkscrew ureter | Alternating areas of stricture and segmental dilatation |
| 3 | Pipe-stem ureter | Diffusely thickened, shortened and rigid ureter due to fibrosis - late change |
| 4 | Multiple ureteric strictures | Predominantly at lower third and ureteropelvic junction - highly suggestive of TB |
| 5 | Distal ureteric narrowing | Stricture at ureterovesical junction (UVJ) |
| 6 | Hydroureter / hydronephrosis | Secondary to obstructing strictures |
| 7 | Ureteral calcification | Intramural, in nondilated ureter |
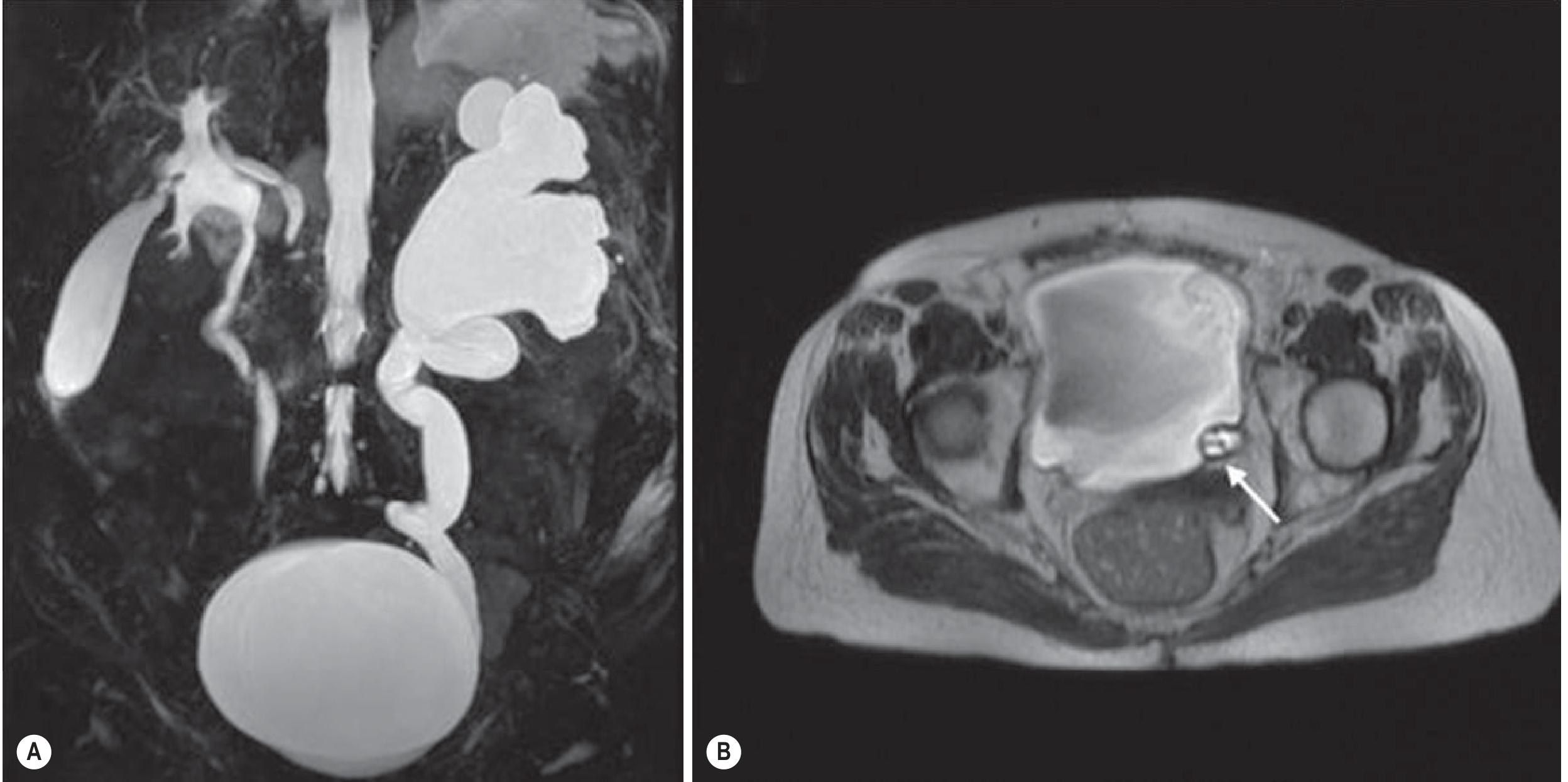
MRI - Ureteric TB
- Severe hydronephrosis and hydroureter proximal to stricture (T2W coronal MIP)
- Complex obstructing ureterocele in the distal ureter with internal "webs"
- Ureteric wall thickening with enhancement
TUBERCULOSIS OF THE BLADDER
Pathological basis
- Hyperaemia near the ureteral orifice
- Superficial ulcers + granulomatous changes involving all layers (pancystitis)
- Healing by fibrosis at the ureteral orifice → refluxing "golf-hole" ureter
- Extensive fibrosis of the bladder wall → "thimble bladder" (capacity <20 mL in severe cases)
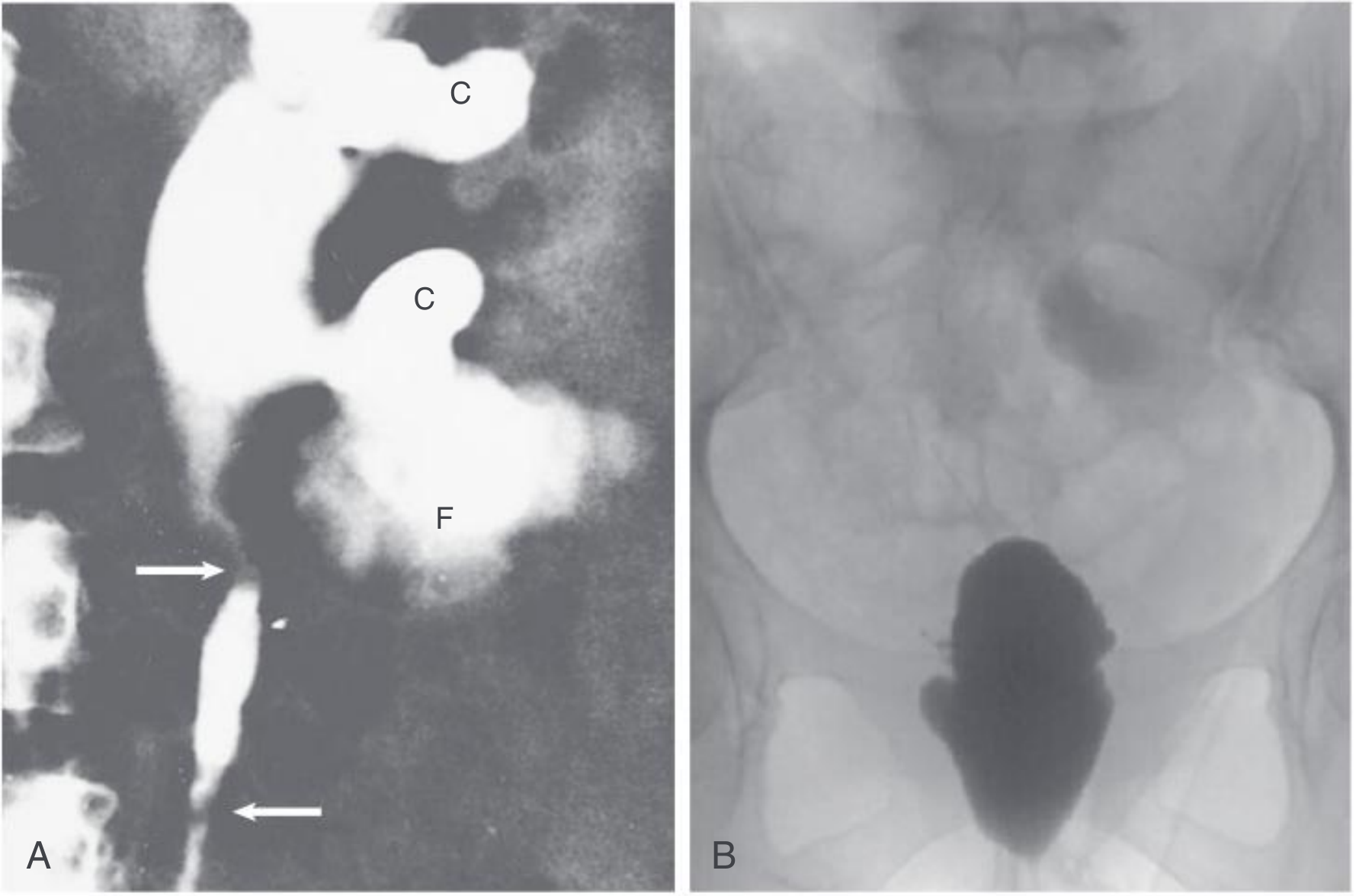
IVU / Cystogram Findings
| # | Sign | Description |
|---|---|---|
| 1 | Mucosal irregularity | Early - cobblestoned/irregular mucosal pattern |
| 2 | Reduced bladder capacity | Progressive luminal contraction |
| 3 | "Thimble bladder" | Small-capacity, thick-walled bladder with elevated bladder base - late/end-stage TB |
| 4 | "Golf-hole" ureter | Fibrosis at ureteral orifice causing a gaping, funnel-shaped opening |
| 5 | Vesicoureteric reflux (VUR) | Due to incompetent "golf-hole" ureteric orifice |
| 6 | Elevated bladder base | Due to fibrosis and contraction |
| 7 | Bladder calcification | Dystrophic calcification of bladder wall - late finding |

CT Findings - Bladder TB
- Diffuse circumferential mural thickening with post-contrast enhancement
- Small bladder capacity
- Dystrophic bladder wall calcification (late)
- Perivesical stranding if perivesical inflammation present
- Fistula formation (vesico-colic, vesico-cutaneous) - late complication
- CT can identify calculi, diverticula and complications including fistula/abscess
USG - Bladder TB
- Thickened bladder wall (>5 mm with full bladder)
- Reduced bladder capacity
- Post-void residual urine elevated
- Hyperechoic foci in wall = calcification
MRI - Bladder TB
- Diffuse mural thickening
- T2W: thickened wall with intermediate signal
- Gadolinium: differential enhancement - generally less enhancement than urothelial tumour
- Sagittal MRI best demonstrates bladder capacity and wall thickening
TUBERCULOSIS OF THE URETHRA
- Rare - usually secondary to bladder or prostatic TB
- Urethral stricture: single or multiple
- May present as urinary obstruction, poor urinary stream
- IVU / Urethrogram (RGU/MCU): urethral narrowing, irregular stricture
- Associated periurethral abscess or fistula can occur
- In males - periurethral abscess, fistula formation
- CT/MRI: periurethral soft tissue thickening, abscess, fistulous tracts
Summary of Named Signs - High Yield
| Sign | Structure | Modality | Meaning |
|---|---|---|---|
| Corkscrew ureter | Ureter | IVU/CT | Alternating strictures + dilatation |
| Pipe-stem ureter | Ureter | IVU/CT | Diffuse fibrosis, rigid/shortened ureter |
| Golf-hole ureter | Ureteric orifice | Cystoscopy/Cystogram | Gaping, fibrosed ureteric orifice with reflux |
| Thimble bladder | Bladder | Cystogram/CT | End-stage contracted bladder (<20 mL) |
| Pancystitis | Bladder | Pathology/CT | Full-thickness granulomatous bladder involvement |
Key teaching point (Grainger & Allison): Fibrotic strictures of infundibula, renal pelvis and ureters are highly suggestive of TB. The presence of three or more features (pelvicalyceal thickening, ulceration, fibrosis ± stricture) is needed for imaging diagnosis.
- Grainger & Allison's Diagnostic Radiology (Ch. 26 & 27) - Renal TB, MR Urography
- Comprehensive Clinical Nephrology, 7th Edition (Ch. 54) - Urinary TB: Pathogenesis, IVU findings
- Bailey & Love's Short Practice of Surgery, 28th Ed. (Ch. 81, 83) - Cystogram images
Pyleoureteritis. Cystica from standard radiology textbooks for of exam for 15 marks. Search easily drawsble diagrams as well for all answers now on this shud be the format
pyeloureteritis cystica radiology IVU CT findings filling defects ureter renal pelvis
https://radiologykey.com/ureter
pyeloureteritis cystica pathology Brunn nests histology radiology differential diagnosis easily drawable diagram
https://clinicalimagingscience.org/ureteritis-cystica-a-radi…
Pyeloureteritis Cystica - Radiology (15 Marks)
Definition
Pathology / Histological Basis
(Knowing this is essential for understanding the imaging)
- Cyst walls are transparent macroscopically
- Contents: mucoproteinaceous fluid
- Surrounding stroma: lymphocytic infiltrate
- No atypia, no goblet cells, no malignant features
✏️ DRAWABLE DIAGRAM 1 - Pathogenesis (Cross-Section of Urothelium)
UROTHELIUM (transitional cells)
│
│ Chronic irritation (stones/UTI)
▼
┌────────────────────────────────────────────┐
│ NORMAL │ VON BRUNN'S NESTS formed │
│ SURFACE │ → buds into lamina propria│
│ UROTHELIUM │ │
│──────────────│─────────────────────────────│
│ │ ┌──────┐ ┌──────┐ │
│ LAMINA │ │ cyst │ │ cyst │ │
│ PROPRIA │ │(fluid│ │(fluid│ │
│ │ └──────┘ └──────┘ │
│──────────────│─────────────────────────────│
│ MUSCULARIS │ │
└────────────────────────────────────────────┘
Cysts project INWARD into lumen
→ filling defects on IVU/CT urogram
Aetiology / Associations
| Factor | Detail |
|---|---|
| Chronic UTI | E. coli (most common), Proteus, Enterococcus |
| Urolithiasis | Stones cause repeated mucosal trauma |
| Prior ureteric instrumentation | Stent placement, ureteroscopy |
| Schistosomiasis | Ova cause chronic irritation |
| Mycobacterium tuberculosis | Can co-exist |
| Diabetes mellitus | Predisposes to recurrent UTI |
| Demographics | Older women > men (due to recurrent UTI predisposition) |
Clinical Features
- Most often an incidental finding
- Symptoms are those of the underlying cause (UTI, stones)
- Haematuria (microscopic/gross)
- Diagnosis confirmed on ureteroscopy or imaging
Radiological Findings
1. Intravenous Urography (IVU) / Retrograde Pyelography (RGP)
| # | Feature | Description |
|---|---|---|
| 1 | Multiple small filling defects | 2-3 mm in diameter in the ureter; up to 2 cm in the renal pelvis |
| 2 | Smooth, round to oval | Well-defined, rounded lucent defects projecting into the contrast-filled lumen |
| 3 | Hemispherical shape | Cysts appear hemispherical (not completely round like air bubbles) |
| 4 | Scalloping of ureteric margins | When seen in profile, the submucosal cysts produce smooth scalloped margins - a characteristic feature |
| 5 | Bead-like appearance | Multiple cysts along the ureteric wall give a "string of beads" / "bead-like" pattern |
| 6 | Bilateral involvement | Often affects both ureters |
| 7 | No obstruction | Ureter is NOT dilated - this is a key distinguishing feature from tumour |
| 8 | Proximal ureter predominance | Cysts are most common in the proximal ureter |
| 9 | Renal pelvis involvement | Smooth rounded lucent defects in the pelvicalyceal system |
| 10 | Stable over time | Unlike tumours, the filling defects remain unchanged on follow-up studies |
✏️ DRAWABLE DIAGRAM 2 - IVU Appearance
RENAL PELVIS
┌──────────────────┐
│ ○ ○ ○ ○ │ ← smooth round lucent filling defects
│ ○ ○ │ in renal pelvis = PYELITIS CYSTICA
└────────┬─────────┘
│ URETER (not dilated)
───────┤○──────
───────┤ ○───── ← smooth oval filling defects
───────┤○────── projecting inward
───────┤ ○───── = "scalloping" of walls
───────┤○────── ← bead-like / string of beads
───────┤ ○─────
│
BLADDER
2. CT Urogram (CTU) - Now the Preferred Modality
| Phase | Finding |
|---|---|
| Non-contrast | Ureteric wall appears normal; cysts not visible |
| Nephrographic phase | Cysts may be subtle / missed |
| Excretory / delayed phase | The diagnostic phase - multiple punctate rounded filling defects clearly visible in contrast-filled collecting system |
- Punctate rounded filling defects (2-3 mm) in the collecting system on excretory phase
- Best visualised in bone window settings - uniform tiny filling defects are clearly resolved
- Cysts contain fluid density (too small to measure HU reliably)
- No ureteric wall thickening (unlike ureteritis/TB)
- No perinephric stranding
- No obstruction / hydroureter
- CT is superior to IVU for detecting associated stones/cause
3. Ultrasound (USG)
- Limited utility for this condition
- May show subtle echogenic foci along the urothelial lining
- Cysts are too small to individually characterise on USG
- Can identify hydronephrosis if present (though usually absent)
- Useful for identifying associated stones (the causative factor)
4. MRI
- Not routinely used
- May show subtle filling defects on MR urography (T2W heavily weighted sequences)
- Role is mainly for equivocal cases or when CT is contraindicated
Differential Diagnosis of Multiple Filling Defects in Ureter / Renal Pelvis
| Condition | Distinguishing Feature |
|---|---|
| Urothelial carcinoma (TCC) | Irregular, asymmetric defects; causes obstruction/hydroureter; progresses on follow-up; enhances on CT |
| Blood clots | Change in position/disappear on repeat imaging; no fixed relationship to wall |
| Air bubbles | Perfectly round (not hemispherical); change position with posture |
| Radiolucent stones | Single or few; fixed position; visible on unenhanced CT |
| Fibroepithelial polyp | Single, elongated, smooth "worm-like" filling defect |
| Vascular impressions | Linear/extrinsic; related to vessel course |
| Tuberculosis | Associated papillary necrosis, calcification, strictures, non-dilated calcified ureter |
| Sloughed renal papillae | Triangular/ring-shadow defect; associated papillary necrosis |
✏️ DRAWABLE DIAGRAM 3 - Key Differentiating Features
MULTIPLE FILLING DEFECTS IN URETER
┌─────────────────────────────────────────────────────────┐
│ │
│ SMOOTH + UNIFORM + SMALL (2-3mm) │
│ + NO OBSTRUCTION + BILATERAL + STABLE │
│ ↓ │
│ PYELOURETERITIS CYSTICA ✓ │
│ │
├─────────────────────────────────────────────────────────┤
│ │
│ IRREGULAR + ASYMMETRIC + ENHANCING │
│ + CAUSES OBSTRUCTION + PROGRESSES │
│ ↓ │
│ UROTHELIAL CARCINOMA ✗ │
│ │
├─────────────────────────────────────────────────────────┤
│ │
│ CHANGE POSITION / DISAPPEAR on repeat imaging │
│ ↓ │
│ CLOTS / AIR BUBBLES ✗ │
│ │
└─────────────────────────────────────────────────────────┘
Key Radiological Points to Emphasise in Exam
- Pyeloureteritis cystica is listed as a false positive for upper tract urothelial carcinoma (Grainger & Allison, Table 31.2) - making correct recognition clinically important
- IVU demonstrates it well due to small lesion size - IVU is stated as particularly useful for "pyeloureteritis cystica" in Smith & Tanagho's General Urology (p. 104)
- CTU excretory/delayed phase is the modern investigation of choice - bone window settings improve detection
- Stability on follow-up and negative urine cytology are reassuring features
- No treatment required for PUC itself - treat the underlying cause (stones, UTI)
Summary Box (15-Mark Answer Checklist)
| Topic | Points |
|---|---|
| Definition + spectrum (pyelitis / ureteritis / PUC) | 1 |
| Pathology - von Brunn's nests, cystic degeneration | 2 |
| Aetiology - UTI, stones, instrumentation | 1 |
| IVU findings - smooth, round, bilateral, non-obstructing, hemispherical | 3 |
| CT urogram - excretory phase, punctate defects, bone windows | 2 |
| USG / MRI findings | 1 |
| Differential diagnosis with distinguishing features | 3 |
| Prognosis / clinical significance | 1 |
| Drawable diagram | ✓ |
| Total | 15 |
- Grainger & Allison's Diagnostic Radiology - Table 31.2 (False-positive UTUC diagnoses, including ureteritis cystica)
- Smith & Tanagho's General Urology, 19e - IVU clinical applications + Fig. 6-33 (CTU ureteritis cystica)
- Journal of Clinical Imaging Science - Radiologic-Pathologic Correlation of Ureteritis Cystica