Maintenance of ph of body physiology short notes easy words
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here are your complete, easy-to-understand short notes on Maintenance of pH of the Body.
Maintenance of pH of the Body - Short Notes
What is pH and Why Does It Matter?
- pH is a measure of how acidic or basic a fluid is.
- Normal blood (arterial) pH = 7.35 to 7.45 (slightly alkaline)
- Intracellular pH = 7.0 to 7.3
- Even small changes outside this range can disrupt enzymes, proteins, and cell function - this is why the body controls pH so tightly.
How Much Acid Does the Body Produce Daily?
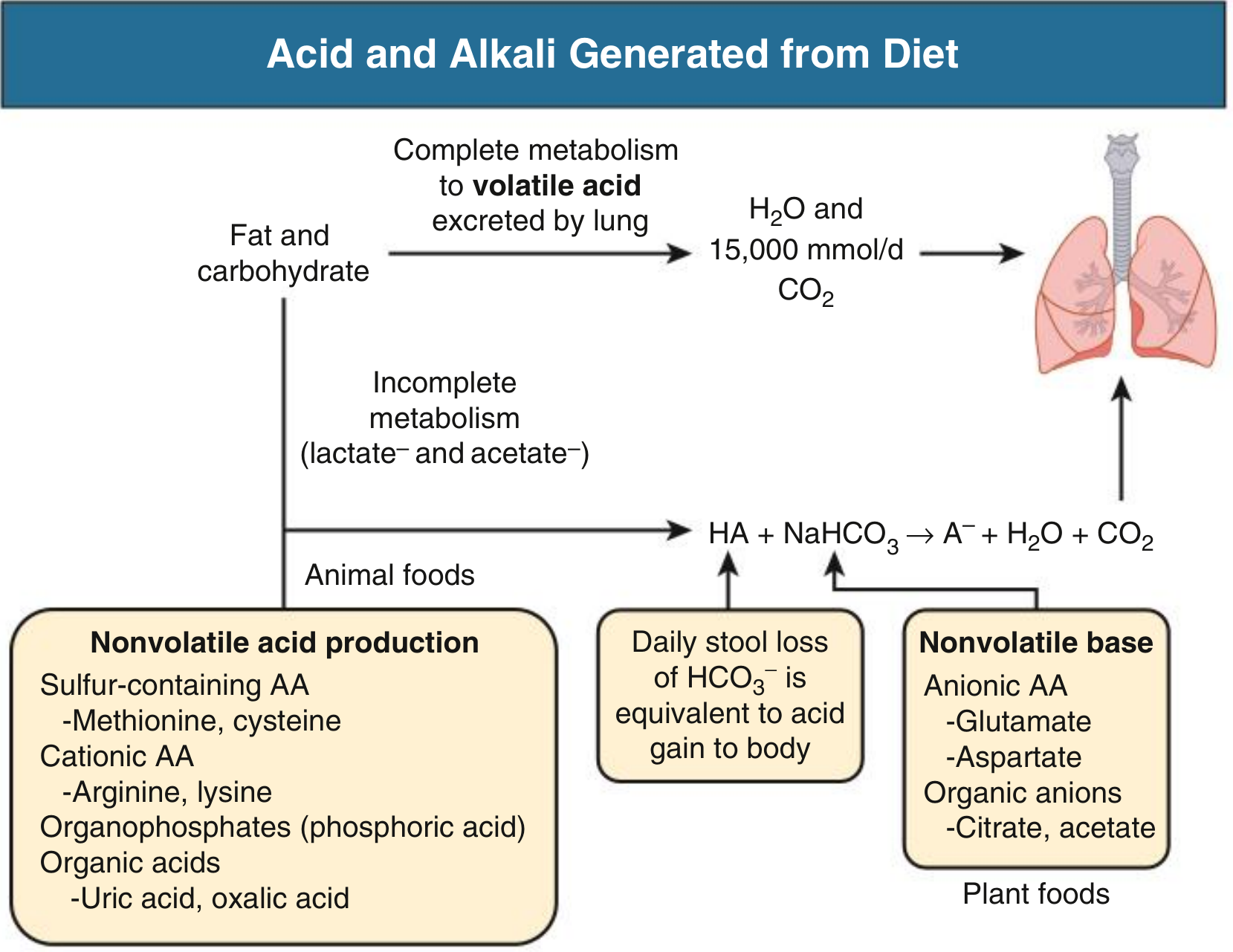
The body constantly produces acid from normal metabolism:
| Source | Type of Acid |
|---|---|
| Fat and carbohydrate metabolism | CO2 (volatile acid) - 15,000 mmol/day |
| Protein (methionine, cysteine) | Sulfuric acid (H2SO4) |
| Organophosphates | Phosphoric acid (H3PO4) |
| Incomplete metabolism | Lactic acid, acetic acid |
- Animal food = net acid load
- Plant food = net alkaline load
- Net non-volatile acid production = ~1 mmol H+ per kg body weight per day
3 Main Ways the Body Maintains pH
1. Buffer Systems (First Line of Defense - Fastest)
A buffer is like a sponge - it soaks up extra acid or base so pH does not change dramatically.
Most important buffer: Bicarbonate - CO2 system (HCO3- / CO2)
- When acid (HA) is added:
HA + NaHCO3 → NaA + H2O + CO2
- The CO2 is blown off by the lungs, keeping pH stable.
- HCO3- acts as the "sponge" that absorbs the acid.
Other buffers:
- Plasma proteins - in the blood
- Phosphate ions - in blood and urine
- Hemoglobin - inside red blood cells
- Bone - in chronic metabolic acidosis, bone dissolves to release alkali (but causes osteoporosis long-term)
- Intracellular buffers - hemoglobin, cell proteins, organophosphates
Buffers only minimize pH change - they do NOT remove acid from the body.
2. Respiratory System (Second Line - Acts Within Minutes)
The lungs control CO2 levels. CO2 behaves like an acid (CO2 + H2O → H2CO3).
Key equation (Henderson-Hasselbalch):
pH depends on the ratio of HCO3- to CO2
- Acidosis (low pH) → brain detects it → breathing speeds up → more CO2 blown out → pH rises back up
- Alkalosis (high pH) → breathing slows down → CO2 retained → pH falls back down
Numbers to remember:
- In metabolic acidosis: for every 1 mmol/L fall in HCO3-, PaCO2 drops by 1.2 mmHg
- In metabolic alkalosis: for every 1 mmol/L rise in HCO3-, PaCO2 rises by 0.7 mmHg
Respiratory compensation is fast but usually does not fully normalize pH on its own.
3. Kidneys (Third Line - Slowest but Most Powerful)
The kidneys are the only organs that actually remove excess acid from the body. They do this through Net Acid Excretion (NAE):
NAE = NH4+ excreted + Titratable acids excreted - HCO3- excreted
Three components of renal acid excretion:
| Component | Contribution | Details |
|---|---|---|
| Ammonium (NH4+) | ~60% | Made from glutamine in kidney cells; main way to excrete acid |
| Titratable Acids | ~40% | Mainly phosphate (HPO4²-) filtered at glomerulus; binds H+ in urine |
| Bicarbonate loss | Negative | Kidneys reabsorb all HCO3- normally; loss = acid gain |
How kidneys handle bicarbonate:
- Normally the kidney reabsorbs all filtered HCO3- (mainly in the proximal tubule)
- If blood is too acidic → kidneys make and secrete more H+ → regenerate new HCO3- → blood pH rises
- If blood is too alkaline → kidneys excrete HCO3- in urine
Kidney compensation takes hours to days but provides the most thorough correction.
Summary Table
| Mechanism | Speed | What It Does |
|---|---|---|
| Buffers (HCO3-, proteins, phosphate, Hb) | Seconds | Absorb H+ immediately, minimize pH change |
| Lungs | Minutes | Control CO2 levels by changing breathing rate |
| Kidneys | Hours to days | Excrete or retain acid/base; final fine-tuning |
Easy Memory Trick
"BBR" - Buffers soak, Breathing blows, Renal removes
Key Values to Remember
| Parameter | Normal Value |
|---|---|
| Arterial blood pH | 7.35 - 7.45 |
| Intracellular pH | 7.0 - 7.3 |
| PaCO2 | 35-45 mmHg |
| Serum HCO3- | 22-26 mEq/L |
| Daily acid load | ~1 mmol H+/kg/day |
Source: Comprehensive Clinical Nephrology, 7th Edition - Chapter 12: Acid-Base Homeostasis
Maintenance of ph of body short notes renal physiology easy words
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for complete, detailed short notes. Here they are:
Renal Physiology: Maintenance of pH - Short Notes (Easy Words)
Why the Kidney is Special
- Buffers and lungs only minimize or temporarily fix pH changes
- The kidney is the only organ that permanently removes acid from the body
- It is the slowest but most powerful controller of pH
- Normal blood pH = 7.35 to 7.45
- Daily acid load from diet and metabolism = ~1 mEq/kg/day (about 35-70 mEq total per day)
What the Kidney Must Do
The kidney has two main jobs to keep pH normal:
- Reabsorb (recover) almost all the bicarbonate (HCO3-) filtered at the glomerulus - so it is not lost in urine
- Regenerate new HCO3- to replace what is used up neutralizing daily acid production
Think of it this way: your blood uses HCO3- as a sponge to soak up acid every day. The kidney makes a fresh sponge each day and sends it back to the blood.
Net Acid Excretion (NAE) Formula
NAE = NH4+ + Titratable Acid - HCO3-
This is how we measure how much acid the kidney has excreted. Under normal conditions, NAE = 0 bicarbonate in urine (all reabsorbed).
Part 1 - Bicarbonate Reabsorption Along the Nephron
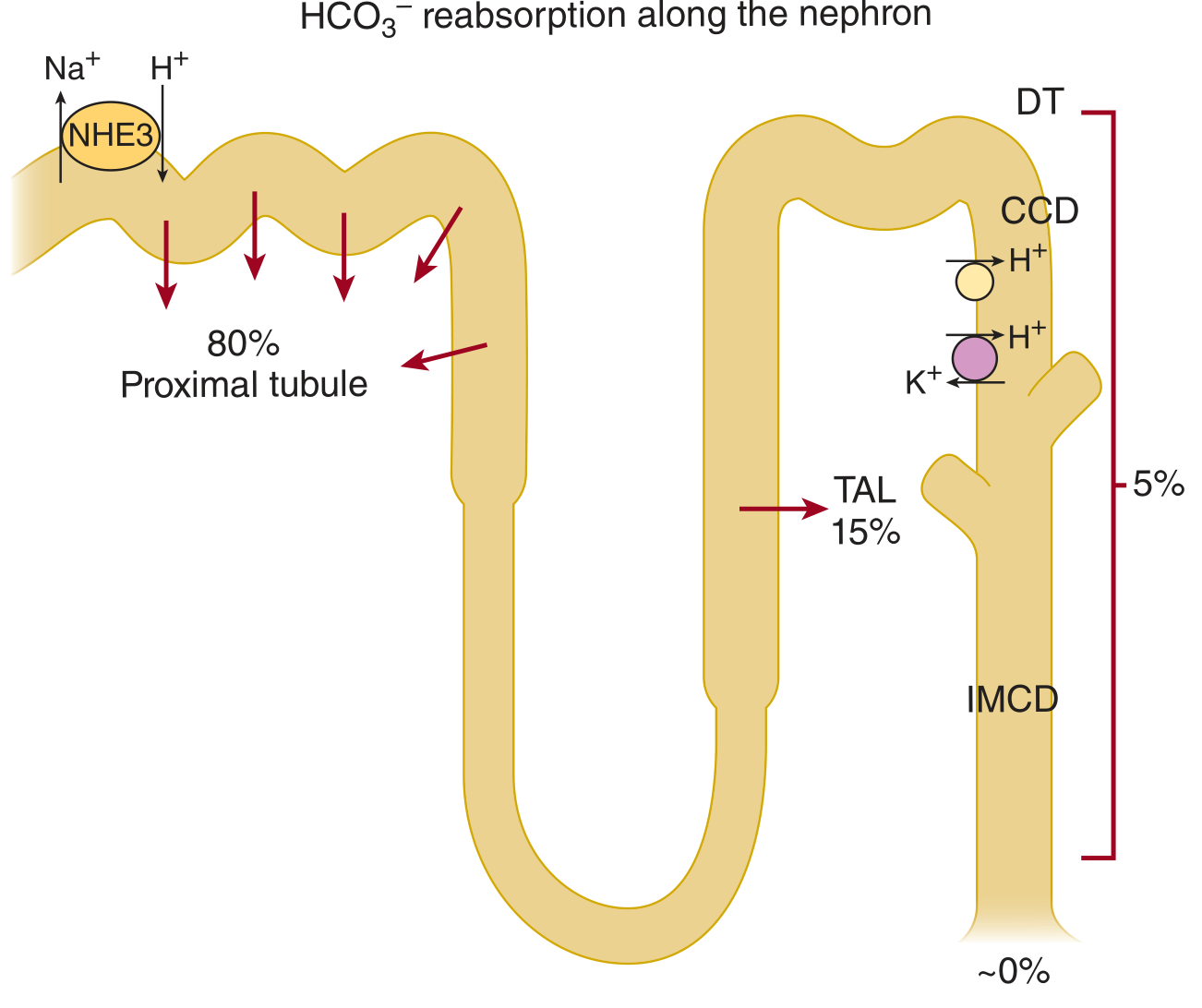
| Nephron Segment | % HCO3- Reabsorbed | Main Transporter |
|---|---|---|
| Proximal tubule | 80% | NHE3 (Na+/H+ exchanger) |
| Thick ascending limb (TAL) | 15% | NHE3 + H+-ATPase |
| Collecting duct (CCD + IMCD) | 5% | H+-ATPase, H+-K+-ATPase |
| Final urine | ~0% | None remains |
How Proximal Tubule Reabsorbs HCO3- (Simple Steps)
- Tubule cell pumps H+ into the lumen via the NHE3 exchanger (H+ out, Na+ in)
- In the lumen: H+ + HCO3- → H2CO3 (carbonic acid)
- Carbonic anhydrase IV (on brush border) breaks it down: H2CO3 → CO2 + H2O
- CO2 freely enters the cell
- Inside the cell: Carbonic anhydrase II reforms: CO2 + H2O → HCO3- + H+
- HCO3- exits to blood via NBC1 cotransporter (with Na+)
- The H+ goes back to step 1
Key point: Carbonic anhydrase (CA) is essential here. Block CA with acetazolamide → HCO3- is lost in urine → urine becomes alkaline.
Part 2 - Titratable Acid Excretion (~40% of NAE)
- Some weak acid buffers are filtered at the glomerulus (mainly phosphate - HPO4²-)
- As H+ is secreted into tubular fluid, it combines with these buffers:
H+ + HPO4²- → H2PO4- (excreted in urine)
- This H+ is now "trapped" in urine and cannot come back
- Called "titratable" because you can measure it by titrating urine back to blood pH with alkali
Other titratable buffers: creatinine, uric acid
Part 3 - Ammonium (NH4+) Excretion (~60% of NAE)
This is the most important and most flexible component - it increases hugely in acidosis.
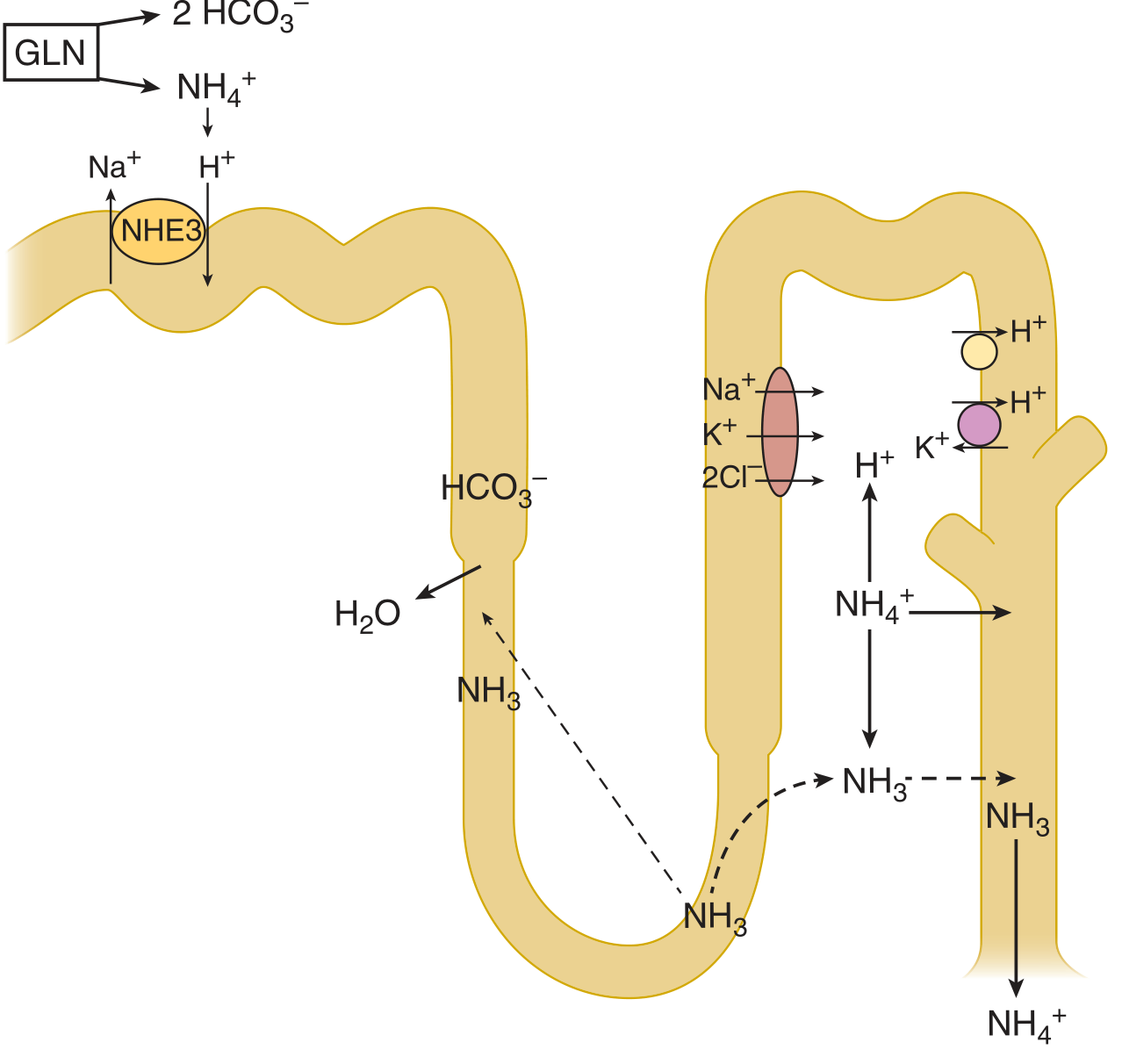
Simple Steps:
- Proximal tubule cells take up glutamine (amino acid from blood)
- Glutamine is broken down → makes 2 NH4+ + 2 HCO3- per molecule
- NH4+ is secreted into the tubular lumen (via NHE3, replacing H+)
- The new HCO3- goes back to the blood (this is the "new" bicarbonate)
- In the thick ascending limb, NH4+ is reabsorbed into the medullary interstitium
- NH3 (gas form) diffuses back into the collecting duct lumen
- In the collecting duct, H+ secreted by alpha-IC cells meets NH3:
NH3 + H+ → NH4+ (trapped in urine and excreted)
Key insight: For every NH4+ excreted, the kidney generates one "new" HCO3- to replenish the blood buffer. This is the kidney actually making new alkalinity.
NH4+ excretion is upregulated by:
- Acidosis
- Hypokalemia
NH4+ excretion is decreased by:
- Hyperkalemia
- Chronic kidney disease (major reason CKD causes metabolic acidosis)
Part 4 - The Collecting Duct: Fine-Tuning of pH
The collecting duct has two types of intercalated cells (IC cells):
| Cell Type | What It Does | Key Transporters |
|---|---|---|
| α-IC cell (type A) | Secretes H+ into urine (acid secretion) | Apical: H+-ATPase, H+-K+-ATPase; Basolateral: AE1 (Cl-/HCO3- exchanger) |
| β-IC cell (type B) | Secretes HCO3- into urine (when blood is too alkaline) | Apical: Pendrin (Cl-/HCO3- exchanger); Basolateral: H+-ATPase |
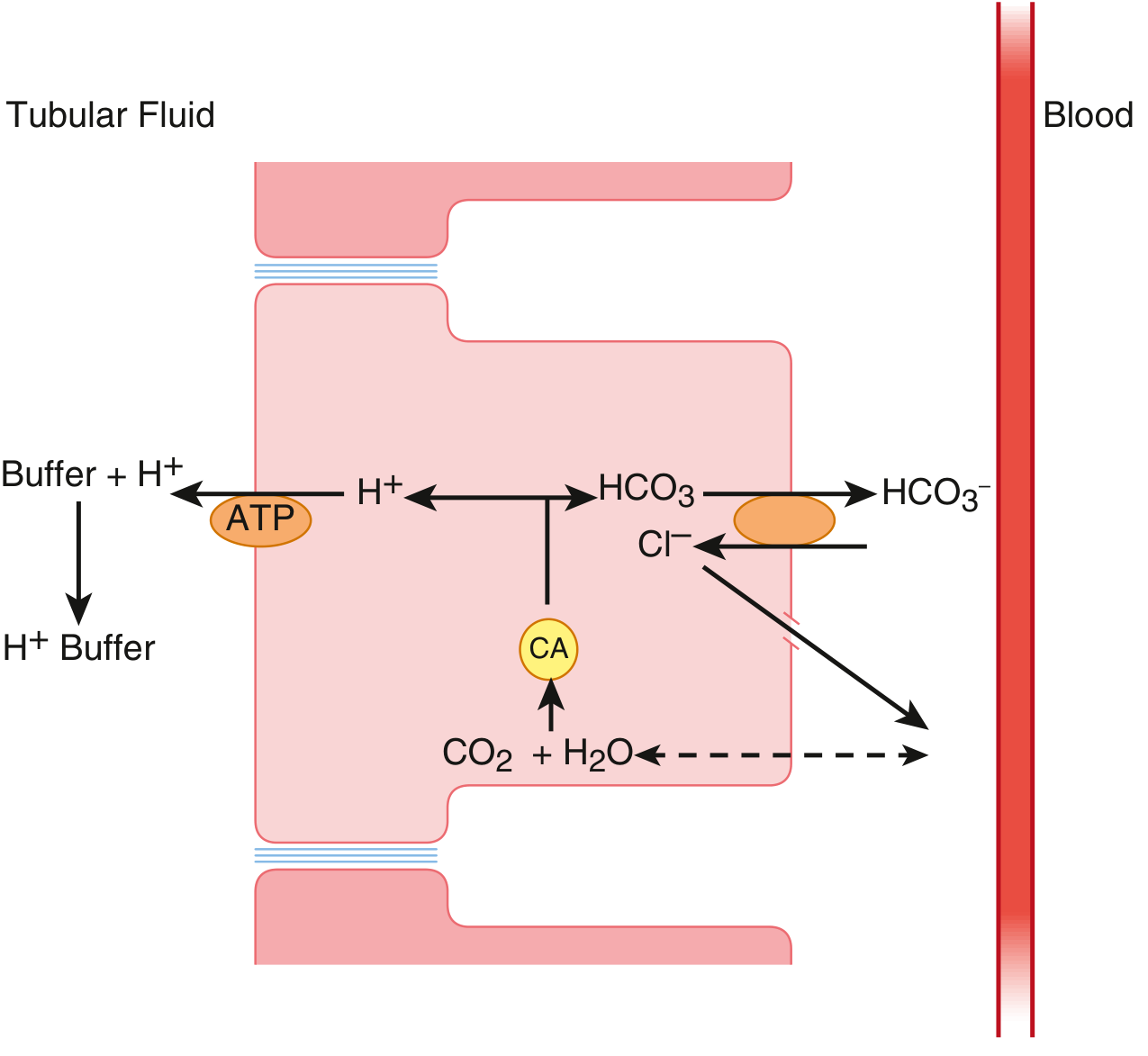
How α-IC Cell Works (in Acidosis):
- Inside cell: CO2 + H2O → H+ + HCO3- (via carbonic anhydrase II)
- H+ pumped into tubular lumen via H+-ATPase (ATP-powered proton pump)
- H+ titrates NH3 and phosphate in urine → trapped as NH4+ and H2PO4-
- HCO3- exits basolateral side to blood via AE1 exchanger (Cl-/HCO3-)
- Net result: acid removed from body, blood gets new HCO3-
Hormonal Control:
- Aldosterone stimulates Na+ absorption by principal cells → makes lumen more electrically negative → drives more H+ secretion by α-IC cells
- Chronic metabolic acidosis converts β-IC cells into α-IC cells → more acid-secreting cells
Summary: Kidney's 3 Tools to Control pH
| Mechanism | Where | Contribution | Key Enzyme/Transporter |
|---|---|---|---|
| HCO3- reabsorption | Proximal tubule mainly | Prevents HCO3- loss | NHE3 + Carbonic anhydrase |
| Titratable acid excretion | Collecting duct | ~40% of NAE | Phosphate buffer in urine |
| NH4+ excretion | Proximal tubule + Collecting duct | ~60% of NAE | Glutamine metabolism + H+-ATPase |
Key Numbers to Remember
| Parameter | Value |
|---|---|
| Normal urine pH | ~5 to 6 |
| Minimum urine pH | ~4.5 (max gradient = 3 pH units) |
| Daily NAE (Western diet) | 35-70 mEq/day |
| NH4+ contribution to NAE | ~60% |
| Titratable acid contribution | ~40% |
| HCO3- in normal urine | ~0% |
Easy Memory: "The 3 R's of Renal pH Control"
Reabsorb HCO3- (don't lose the buffer) Remove acid via phosphate (titratable acids) Regenerate new HCO3- via ammonium excretion
Sources: Comprehensive Clinical Nephrology 7th Ed.; Brenner and Rector's The Kidney; Goldman-Cecil Medicine; Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.