Pulsus paradoxas
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulsus paradoxus" mechanism clinical
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Pulsus Paradoxus
Definition
Pulsus paradoxus is an exaggerated fall in systolic blood pressure (>10-12 mmHg) during inspiration. Normally, inspiration causes a slight (~3-5 mmHg) decrease in systolic BP due to physiological intrathoracic pressure changes. When this drop exceeds 10-12 mmHg, it is defined as pulsus paradoxus.
- Harrison's Principles of Internal Medicine 22e defines it as a fall in systolic pressure >10 mmHg with inspiration
- Roberts and Hedges' Clinical Procedures in Emergency Medicine uses >12 mmHg as the threshold for abnormal
The name is "paradoxical" because the heart keeps beating, yet the radial pulse may disappear entirely on inspiration - a pulse that can be heard but not felt, which was the original paradox described by Kussmaul.
Pathophysiology / Mechanism
The diagram below illustrates the three parallel pathways triggered during inspiration that converge to reduce left ventricular output:
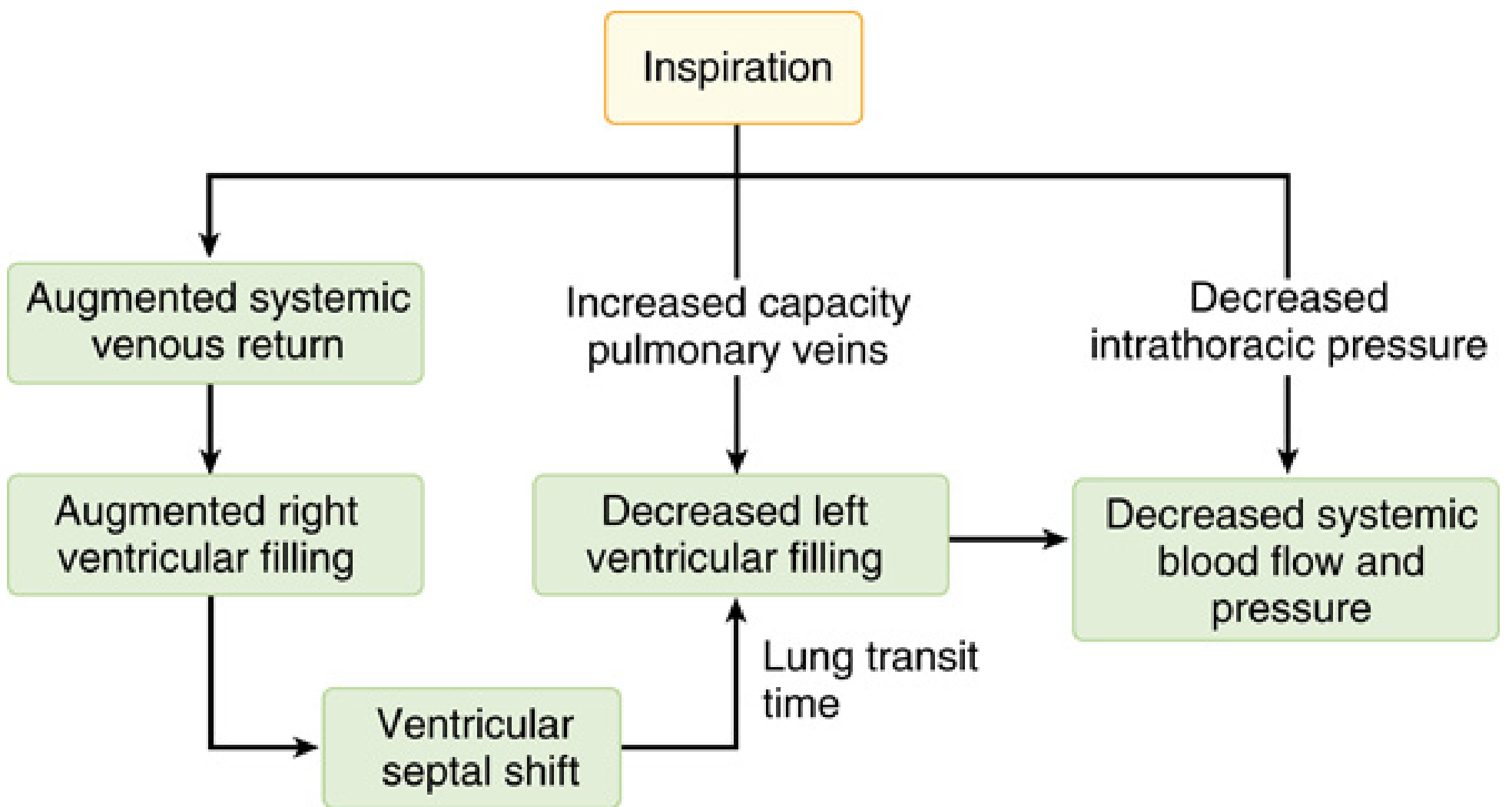
Three simultaneous mechanisms operate during inspiration:
-
Augmented right ventricular filling - Inspiration decreases intrathoracic pressure, increasing systemic venous return and RV preload. This causes the interventricular septum to shift leftward (ventricular septal shift), encroaching on the LV cavity and reducing LV filling.
-
Increased pulmonary venous capacitance - The expanding lungs "pool" blood in the pulmonary vasculature, reducing pulmonary venous return to the left atrium. Combined with lung transit time delays, LV preload drops.
-
Decreased intrathoracic pressure increases LV afterload - The LV must generate greater pressure against a more negative intrathoracic environment, increasing effective afterload.
All three mechanisms converge on decreased LV filling → decreased LV stroke volume → fall in systolic BP on inspiration.
In cardiac tamponade, the pericardial fluid prevents normal transmission of intrathoracic pressure changes to the cardiac chambers, making this fall in LV filling especially pronounced. This is the concept of ventricular interdependence operating within a fixed, fluid-constrained pericardial space.
- Miller's Anesthesia, 10e, Chapter 50
Causes
Cardiac causes:
- Cardiac tamponade - classic cause; typically >20 mmHg in moderate-severe tamponade
- Constrictive pericarditis (some cases)
- Cardiogenic shock
- Cardiac failure
Pulmonary / Respiratory causes:
- Severe asthma (exaggerated negative intrathoracic pressure swings)
- COPD / severe emphysema
- Tension pneumothorax
- Massive pulmonary embolism
Other:
- Hemorrhagic / hypovolemic shock
- Obesity (labored breathing)
Conditions Where Pulsus Paradoxus May Be ABSENT Despite Tamponade
This is a high-yield exam point. Pulsus paradoxus may be absent in tamponade when:
| Condition | Reason |
|---|---|
| Aortic insufficiency (AR) | LV has alternate filling route; LV pressure stays elevated |
| Atrial septal defect (ASD) | Right-to-left shunting equalizes RV/LV preloads |
| Positive pressure ventilation | Reverses intrathoracic pressure dynamics |
| Elevated LVEDP (LV hypertrophy, chronic HTN) | LV too stiff to show further volume-dependent pressure changes |
| Loculated / eccentric pericardial effusions | Pressure not transmitted uniformly to all chambers |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 16
Measurement Technique
The bedside BP cuff method is standard:
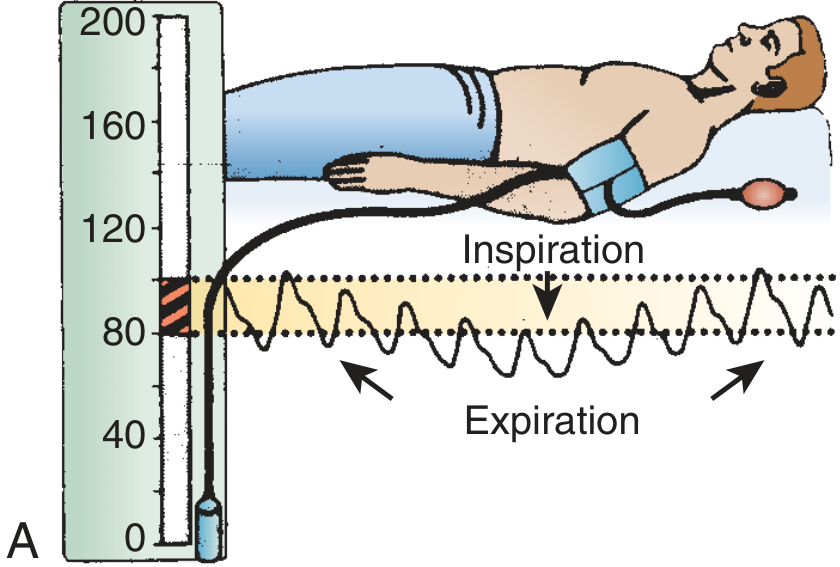
Step-by-step:
- Patient reclines at 30-45 degrees, breathing normally
- Inflate cuff above systolic pressure
- Deflate slowly until Korotkoff sounds are first heard only during expiration - record this pressure (Point A)
- Continue deflating until Korotkoff sounds are heard throughout the respiratory cycle - record this pressure (Point B)
- Pulsus paradoxus = A - B (in mmHg)
- A difference >12 mmHg = abnormal (>20-30 mmHg in significant tamponade)
Pitfalls in measurement:
- Tachycardia, atrial fibrillation, and tachypnea make it difficult to measure accurately
- In very narrow pulse pressure (advanced tamponade), the paradox may be "deceptively small" at only 5-15 mmHg
Alternative method: Pulse oximetry plethysmographic waveform - visually observe loss and reappearance of the waveform with respiration. Validated in ICU settings.
Clinical Significance
| Pulsus Paradoxus | Interpretation |
|---|---|
| <10 mmHg | Normal |
| 10-20 mmHg | Abnormal - consider tamponade, severe asthma |
| >20 mmHg | Moderate-severe tamponade |
| >25 mmHg | Both sensitive and specific for moderate-severe vs. mild tamponade (in hemodynamically stable patients with effusion) |
Echocardiographic data: an abnormal pulsus paradoxus has sensitivity 79%, specificity 40%, PPV 81%, NPV 40% for right ventricular diastolic collapse.
Practical caveat: In traumatic tamponade, pulsus paradoxus is present in only ~8.6% of patients and should not replace bedside ultrasound. In unstable patients, assessment for pulsus paradoxus should never delay definitive evaluation. - Roberts and Hedges, Chapter 16
Quick Comparison with Pulsus Alternans
| Feature | Pulsus Paradoxus | Pulsus Alternans |
|---|---|---|
| Variation | Respiratory-linked | Beat-to-beat (independent of respiration) |
| Mechanism | Ventricular interdependence + preload changes | Severe LV systolic dysfunction |
| Key association | Tamponade, severe asthma | Severe LV failure |
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapters 1 & 16
- Miller's Anesthesia, 10e, Chapter 50 (Pericardial Tamponade)
- Harrison's Principles of Internal Medicine, 22e, Chapter 246
- Fuster and Hurst's The Heart, 15th ed.
Pulsus alternas
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I have comprehensive data from multiple authoritative textbooks. Here is the full answer:
Pulsus Alternans
Definition
Pulsus alternans is a regular beat-to-beat alternation in the amplitude (strength) of the arterial pulse - alternating strong and weak beats - occurring at a regular heart rate and independent of the respiratory cycle.
On BP measurement: as the cuff is slowly deflated, every other Korotkoff sound is audible before all beats become audible. The difference in systolic BP between strong and weak beats can range from subtle (only detectable with intra-arterial monitoring) to marked (weak beats not palpable at all).
It is an ominous sign of severe left ventricular systolic dysfunction.
The Tracing
Below is an actual invasive aortic pressure tracing + LV outflow tract Doppler from a patient with severe LV systolic dysfunction, showing pulsus alternans. The asterisks (*) mark the reduced-amplitude beats:
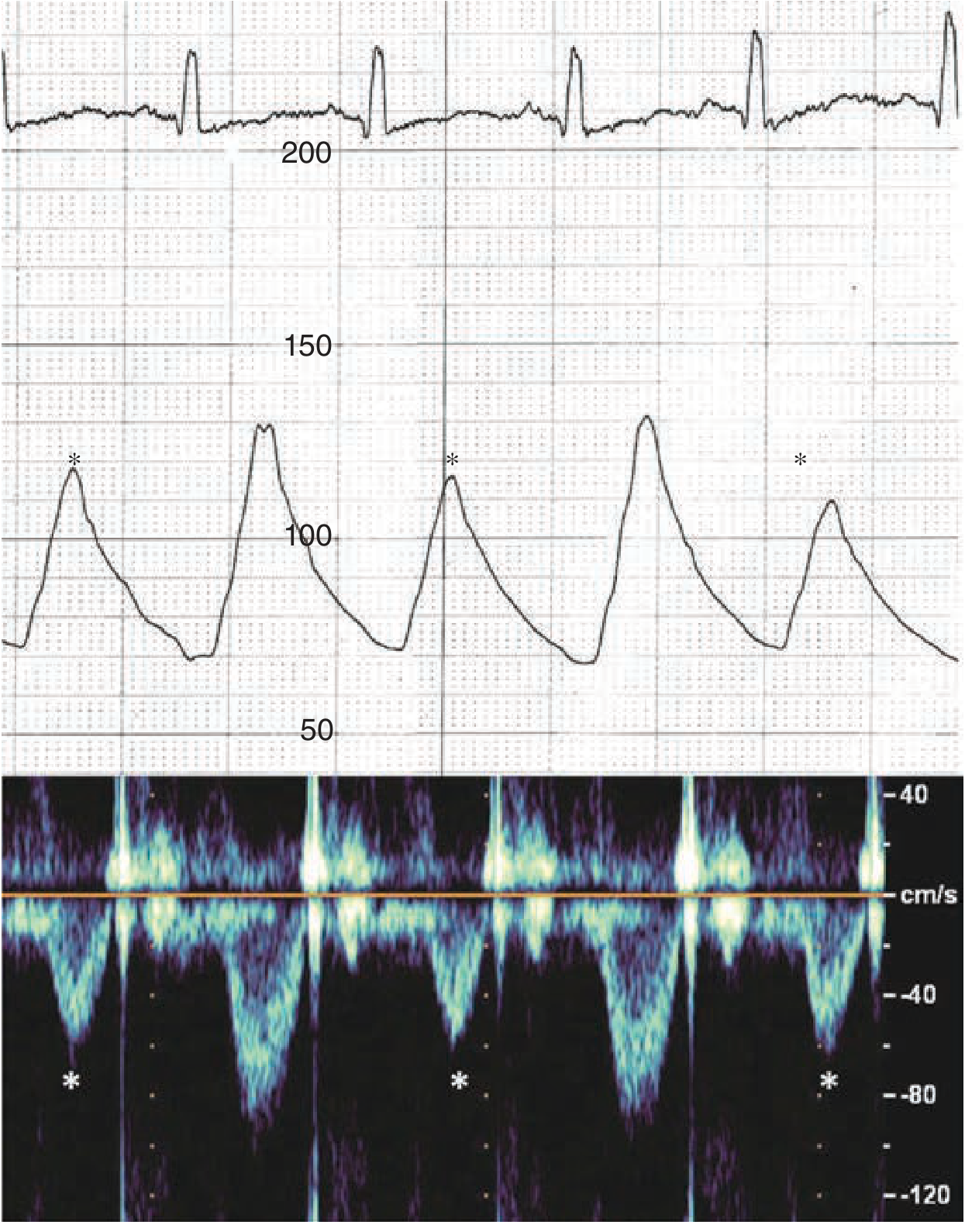
Note the clear alternating tall and short peaks in the pressure waveform (middle panel), and the corresponding alternating strong/weak Doppler signals (bottom panel) - confirming the beat-to-beat alternation in LV stroke volume.
Mechanism
Pulsus alternans is caused by cyclic changes in intracellular calcium and action potential duration in the failing myocardium:
- In severe heart failure, the sarcoplasmic reticulum (SR) cannot adequately handle calcium cycling
- After a strong beat, SR calcium is partially depleted - the next beat has less calcium available for release, producing a weaker contraction (smaller stroke volume)
- After a weak beat, calcium reaccumulates in the SR, leading to a stronger next beat
- This creates the repeating strong-weak-strong-weak alternation
This is fundamentally a cellular calcium cycling instability at the level of the cardiomyocyte, unlike pulsus paradoxus which is a hemodynamic/mechanical phenomenon.
- Harrison's Principles of Internal Medicine 22e: "thought to be due to cyclic changes in intracellular calcium and action potential duration"
Key Clinical Features
| Feature | Detail |
|---|---|
| Rhythm | Regular (sinus rhythm) |
| Respiratory relationship | None - NOT respirophasic |
| Cause | Severe LV systolic dysfunction |
| Amplitude variation | Beat-to-beat (every other beat is weak) |
| In severe cases | Weak beat may be completely impalpable (every other beat disappears) |
| ECG association | T-wave alternans (electrical alternans of repolarization) |
| Prognostic significance | T-wave alternans + pulsus alternans = increased risk for arrhythmic events |
Causes / Associated Conditions
- Severe left ventricular systolic dysfunction (primary cause) - any etiology:
- Dilated cardiomyopathy
- Ischemic cardiomyopathy / large MI
- Decompensated heart failure
- Tachycardia (can precipitate or worsen alternans in a failing ventricle)
How to Measure (Auscultation Method)
- Patient breathes calmly and quietly
- Inflate BP cuff above systolic pressure
- Deflate slowly - initially only alternating (every other) Korotkoff sounds will be heard
- Continue deflating until all beats are audible
- The difference between the pressure where alternating sounds are heard vs. where all sounds are heard = magnitude of pulsus alternans
Comparison with Pulsus Paradoxus
| Feature | Pulsus Alternans | Pulsus Paradoxus |
|---|---|---|
| Pattern | Strong-weak-strong-weak (beat-to-beat) | Falls on inspiration, rises on expiration |
| Rhythm | Regular, constant rate | Any rhythm |
| Respiratory link | None | Yes - respirophasic |
| Mechanism | Calcium cycling instability in cardiomyocytes | Ventricular interdependence + preload changes |
| Primary cause | Severe LV systolic dysfunction | Cardiac tamponade, severe asthma |
| Prognosis | Ominous - severe pump failure | Depends on cause |
Pulse Abnormalities Summary Table (Miller's Anesthesia, 10e)
| Condition | Pulse Abnormality |
|---|---|
| Aortic stenosis | Pulsus parvus (narrow pressure) + pulsus tardus (delayed upstroke) |
| Aortic regurgitation | Bisferiens pulse (double peak) + wide pulse pressure |
| Hypertrophic cardiomyopathy | Spike-and-dome pattern |
| LV systolic failure | Pulsus alternans |
| Cardiac tamponade | Pulsus paradoxus |
Sources:
- Harrison's Principles of Internal Medicine, 22e, Chapter 246
- Fuster and Hurst's The Heart, 15th ed., Chapters 2
- Miller's Anesthesia, 10e, Table 32.1
This is a shared conversation. Sign in to Orris to start your own chat.