Day care surgery seminar questions
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the material needed. Let me compile the comprehensive viva/short answer questions.
Day Care Surgery - PG Seminar: Short Answer / Viva Questions
(Sources: Bailey & Love's Short Practice of Surgery 28e; Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11e; Miller's Anesthesia 10e)
SECTION 1: Definition, Background & Concepts
Q1. Define day surgery. What is the etymological significance of the term "ambulatory surgery"?
Day surgery is the admission of selected patients to hospital for a planned surgical procedure with return home on the same day. The word ambulatory derives from the Latin ambulare ("to walk"), indicating that patients arrive under their own power and depart to their home environment after the procedure.
- Bailey & Love 28e, p. 320
Q2. What factors drove the expansion of day surgery since the 1980s?
Three main factors:
- Improved anaesthesia techniques (shorter-acting agents, regional blocks)
- Development of minimally invasive (laparoscopic/endoscopic) procedures
- Healthcare policy changes - particularly funding reforms and financial incentives for hospitals to shift elective procedures to outpatient settings Outpatient procedures grew from 19% to 60% of all US surgical volume between 1981 and 2011.
- Schwartz's 11e
Q3. What are the three main settings for ambulatory surgery?
- Hospital outpatient departments (HOPDs)
- Freestanding ambulatory surgery centres (ASCs)
- Physician's office-based surgical suites
- Schwartz's 11e
Q4. List at least five patient and hospital benefits of day surgery.
- Patient recovers in the comfort of home
- Less disruption to domestic/family life
- Reduced risk of hospital-acquired infection
- Greater patient satisfaction scores
- Frees inpatient beds for those who genuinely need them
- Lower cost than inpatient admission
- Activity can continue even during inpatient bed pressures
- Bailey & Love 28e, p. 320
SECTION 2: Patient Selection Criteria
Q5. What is the single most important principle governing patient selection for day surgery?
Selection is a dynamic process based on the interaction among: (a) the surgical procedure, (b) the patient's comorbidities and functional status, and (c) the anaesthetic technique, as well as social factors and the type of ambulatory facility. There should be no arbitrary cut-offs based on age, BMI, or ASA class alone.
- Current Surgical Therapy 14e, p. 1487; Bailey & Love 28e, p. 321
Q6. What ASA physical status classes are absolute medical exclusions to day surgery?
- ASA 4 or 5 - absolute exclusion
- Unstable ASA 3 or any poorly controlled comorbidity Stable ASA 3 patients may be considered case-by-case with optimisation.
- Bailey & Love 28e, p. 321
Q7. List the specific conditions that render a patient ineligible (ASA 4) for day surgery.
- Recent (<3 months) new-onset, unstable, or severe angina
- Recent MI or coronary stenting
- New-onset or decompensated heart failure
- Severe valve dysfunction
- High-grade AV block
- Cerebrovascular disease (TIA/CVA)
- Acute respiratory disease
- End-stage renal disease not on regular dialysis
- Current Surgical Therapy 14e, p. 1487
Q8. What are the surgical criteria that must be met before adding a patient to a day surgery pathway?
- Low risk of significant immediate postoperative complications (catastrophic bleeding, airway compromise)
- Patient able to eat, drink, or take oral nutrition postoperatively
- Postoperative pain manageable with oral analgesia +/- LA infiltration or peripheral nerve block
- Patient able to mobilise postoperatively (with or without aid)
- Bailey & Love 28e, p. 321
Q9. How should diabetes be managed in the context of day surgery?
- Well-controlled diabetes (HbA1c <69 mmol/mol / ~8.5%) - can be safely managed as a day case
- Poorly controlled diabetes - surgery should be delayed until control is optimised
- These patients have increased risk of cardiovascular complications and poor wound healing
- Schedule first on the operating list to minimise fasting duration
- Bailey & Love 28e, p. 322
Q10. How is obesity/OSA evaluated prior to day surgery? Which scoring tool is used?
The STOP-BANG questionnaire (Snoring, Tiredness, Observed apnoeas, Pressure, BMI, Age, Neck circumference, Gender) screens for undiagnosed OSA. A STOP-BANG score ≥5 is a risk factor making day surgery potentially unsuitable. Other red flags include:
- Poor functional capacity
- SpO2 <94% on room air Suitable obese patients should receive short-acting anaesthetic, avoid long-acting opiates, and allow extra time for anaesthetic recovery.
- Bailey & Love 28e, p. 322
Q11. Should age alone exclude a patient from day surgery?
No. There should be no arbitrary age cut-off. Older patients benefit from awake surgery or short-acting anaesthetics. Suitability should be judged on comorbidities and functional status, not age alone.
- Bailey & Love 28e, p. 321
Q12. What social factors must be confirmed before a patient proceeds to day surgery?
- A responsible adult available to escort the patient home
- A responsible adult to stay with the patient for 24 hours postoperatively
- Access to a phone (for emergencies)
- Appropriate home circumstances
- Ability to understand and follow written postoperative instructions
- Bailey & Love 28e, p. 324
SECTION 3: Common Day Case Procedures
Q13. Name common procedures from the BADS Directory of Procedures (DOP) and their recommended day case rates.
| Specialty | Procedure | Day Case Rate |
|---|---|---|
| General surgery | Laparoscopic cholecystectomy | 75% |
| ENT | Tonsillectomy | 90% |
| Breast | Simple mastectomy | 75% |
| Gynaecology | Vaginal hysterectomy | 60% |
| Orthopaedics | Arthroscopy (knee/shoulder) | 99% |
| Urology | Ureteroscopic calculus extraction | - |
The BADS DOP lists over 200 procedures now suitable as day cases.
- Bailey & Love 28e, p. 321
Q14. What was the traditional time limit for day surgery? Has it changed?
Traditionally, day surgery was limited to procedures lasting less than 1 hour. Currently, procedures lasting 3-4 hours are routinely performed as successful day cases owing to advances in anaesthesia and surgical technique.
- Bailey & Love 28e, p. 321
SECTION 4: Anaesthesia in Day Surgery
Q15. What anaesthetic principles are essential for day surgery?
- Meticulous attention to pain relief and prevention of PONV
- Multimodal analgesia approach with premedication
- Short-acting general anaesthetic agents (e.g., propofol/desflurane/sevoflurane)
- Day case spinals or regional anaesthesia techniques
- Avoidance of long-acting opioids (e.g., IV morphine) - can delay recovery through sedation or nausea
- Bailey & Love 28e, p. 323
Q16. What is "fast-track anaesthetic technique" in ambulatory surgery?
An approach minimising residual drug effects (from hypnotic-sedatives, NMBAs, opioids) to accelerate recovery and reduce 30-day readmission. Key principles:
- Minimal number of drug combinations (additive/synergistic effects)
- Prefer short-acting agents at lowest effective doses
- Superiority of TIVA vs. inhalational anaesthesia remains unclear
- Opioid-free anaesthesia is controversial - adjuncts (ketamine, dexmedetomidine, lidocaine, Mg infusion) may themselves impair recovery
- Current Surgical Therapy 14e, p. 1487
Q17. What are the ventilation targets during day surgery under GA?
- Lung-protective ventilation: tidal volume 6-8 mL/kg ideal body weight
- PEEP: 5-10 cm H2O
- ETCO2 target: ~40 mmHg (rather than traditional 30-35 mmHg) - improves tissue and organ perfusion
- Current Surgical Therapy 14e
Q18. What are the intraoperative fluid management targets in day surgery?
Goal is "zero" fluid balance. Recommend:
- Baseline: 3-5 mL/kg/h balanced crystalloid
- Blood loss replaced with balanced crystalloid at 1:1.5 ratio
- Goal-directed fluid therapy (guided by cardiac output monitoring) for high-risk patients with expected blood loss >1000 mL
- Current Surgical Therapy 14e
Q19. What is the approach to PONV prophylaxis in day surgery?
All patients: at least 2-3 antiemetics from different classes (preop or intraop)
High-risk patients (history of PONV, motion sickness, high opioid requirement): 3-4 antiemetics + TIVA
Options include:
- Scopolamine transdermal patch (1-3 h preop)
- Aprepitant 40 mg PO (1-3 h preop)
- Dexamethasone 8-10 mg IV at induction (also analgesic/anti-inflammatory)
- Ondansetron 4 mg IV or palonosetron 0.75 mg IV (end of surgery)
- Droperidol 0.625-1.25 mg IV (end of surgery)
PONV is the most significant cause of delayed discharge and unplanned hospital admission in day surgery.
- Current Surgical Therapy 14e, p. 1487
SECTION 5: List Planning & Perioperative Pathway
Q20. How should the operating list be planned to optimise day surgery?
- Procedures with longer recovery times (tonsillectomy, knee/hip replacement, complex lap. cholecystectomy) should be placed early on the list
- Exceptions: insulin-dependent diabetics and patients with learning difficulties should be first on the list (to minimise fasting time and waiting anxiety)
- Patients should be encouraged to walk to theatre
- Drains should be generally avoided; if used, clear removal plans must be documented at the time of surgery
- Bailey & Love 28e, p. 323
Q21. What is the role of preoperative assessment specific to day surgery?
In addition to standard preop assessment, day surgery-specific questions include:
- Can surgery be delayed until the medical condition is optimised, and then planned as a day case?
- Can social factors be addressed to make the patient a suitable day case? Anaesthetist should review notes and discuss suitability with the day surgery lead. Nurse-led assessment with anaesthetic review is the standard model.
- Bailey & Love 28e, p. 323
SECTION 6: Discharge Criteria
Q22. What are the standard discharge criteria after day surgery? (Table 22.5, Bailey & Love)
- Vital signs stable for at least 1 hour
- Correct orientation to time, place, and person (where applicable)
- Adequate pain control with oral analgesia supplied
- Patient understands how to use the supplied analgesia
- Ability to dress and walk where appropriate
- Minimal nausea, vomiting, or dizziness
- Has taken oral fluids
- Minimal bleeding or wound drainage
- Has passed urine (where appropriate)
- Has a responsible adult to take them home
- Written and verbal postoperative instructions given
- Knows when to return for follow-up (if applicable)
- Emergency contact number provided
- Bailey & Love 28e, p. 324
Q23. What is the PADSS and what does it assess?
PADSS = Post-Anaesthesia Discharge Scoring System. It was developed to assess home readiness in ambulatory surgery patients (beyond the standard Aldrete score used for PACU discharge). It assesses:
- Vital signs
- Ambulation and mental status
- Pain
- Nausea/vomiting
- Surgical bleeding
- Fluid intake/output
The current modified version separates pain and PONV as distinct criteria and has eliminated the requirement to void before discharge.
- Miller's Anesthesia 10e
Q24. Who bears ultimate responsibility for discharging a patient from the PACU/day surgery unit?
A supervising physician must accept responsibility for the discharge decision, even when the bedside decision is made by a PACU nurse using hospital-sanctioned scoring systems. The physician's name must be documented on the record. Discharge criteria must be approved by the department of anaesthesia and hospital medical staff.
- Miller's Anesthesia 10e
Q25. When is nurse-led discharge appropriate?
Nurse-led discharge is the standard expectation for day surgery unless an unexpected anaesthetic or surgical issue has occurred. Pre-agreed general criteria (Table 22.5) and any surgery-specific criteria must be met. Post-operative instructions must be given in both written and verbal form with an out-of-hours contact number (not an answerphone).
- Bailey & Love 28e, p. 324
Q26. Is there a time restriction before discharge after tonsillectomy?
Yes - patients must remain in hospital for at least 6 hours after tonsillectomy before discharge. This is one of the few procedure-specific time-based restrictions in day surgery.
- Bailey & Love 28e, p. 324
SECTION 7: Complications & Unplanned Admission
Q27. What is the most common cause of delayed discharge and unplanned hospital admission after day surgery?
Postoperative pain is the most significant cause. Studies of 10,000+ consecutive ambulatory surgical patients found that pain incidence and intensity increased with: higher BMI, longer duration of anaesthesia, and orthopaedic or urologic procedures.
PONV is the second most significant cause.
- Miller's Anesthesia 10e
Q28. What surgical factors increase PONV and pain risk in ambulatory surgery?
- Orthopaedic and urologic procedures (highest pain risk)
- Higher BMI
- Longer duration of anaesthesia
- Female sex, non-smoker, history of PONV/motion sickness (classic Apfel risk factors for PONV)
- Miller's Anesthesia 10e
Q29. What complications should be anticipated in a day surgery unit and may necessitate unplanned overnight admission?
- Uncontrolled pain
- Intractable PONV
- Intraoperative haemorrhage or unexpected findings requiring extended surgery
- Postoperative haemorrhage (especially tonsillectomy)
- Urinary retention
- Adverse anaesthetic events (prolonged sedation, laryngospasm)
- Cardiovascular instability
- Current Surgical Therapy 14e; Bailey & Love 28e
SECTION 8: High-Yield Viva Rapid-Fire Questions
| Question | Answer |
|---|---|
| Definition of day surgery | Planned surgery where the patient is admitted and discharged on the same day |
| The BADS DOP lists how many suitable procedures? | Over 200 |
| Maximum traditional duration of day surgery | <1 hour (now up to 3-4 hours acceptable) |
| ASA exclusion for day surgery | ASA 4/5 absolute; unstable ASA 3 relative |
| HbA1c cut-off for diabetic day surgery patient | <69 mmol/mol (~8.5%) |
| PONV prophylaxis: minimum antiemetics for all patients | 2-3 agents from different classes |
| Most common cause of delayed discharge | Postoperative pain |
| Discharge scoring system for day surgery | PADSS (Post-Anaesthesia Discharge Scoring System) |
| STOP-BANG score cut-off for OSA risk in day surgery | ≥5 |
| Minimum observation after tonsillectomy before discharge | 6 hours |
| What is NOT required before discharge (in modified PADSS)? | Ability to void/pass urine |
| Fluid balance target in day surgery | "Zero" fluid balance; 3-5 mL/kg/h balanced crystalloid |
| ETCO2 target in day surgery ventilation | ~40 mmHg |
| Tidal volume in lung-protective strategy | 6-8 mL/kg ideal body weight |
Sources: Bailey & Love's Short Practice of Surgery 28e (Ch. 22); Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11e (Ch. 52); Miller's Anesthesia 10e (Ch. 76)
Hydrocephalus
Asking for Preferences
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive material from Bailey & Love, Bradley & Daroff's Neurology, Adams & Victor's Neurology, and Grainger & Allison's Radiology. Let me compile the full topic notes.
Hydrocephalus - Comprehensive Topic Notes (PG Level)
Sources: Bailey & Love 28e; Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology 12e; Grainger & Allison's Diagnostic Radiology; Robbins & Kumar Pathology; Harriet Lane Handbook 23e; Miller's Anesthesia 10e
1. Definition
Hydrocephalus is an increase in CSF volume with consequent ventricular enlargement, often causing symptoms of raised intracranial pressure (ICP). More precisely, it refers to a pressure-dependent enlargement of the cerebral ventricles due to obstruction of CSF drainage (Bradley & Daroff's).
Note: "Hydrocephalus" literally means "water on the brain" and is a nonspecific term - it must be distinguished from ventriculomegaly due to cerebral atrophy ("hydrocephalus ex vacuo"), which does NOT benefit from intervention.
2. CSF Physiology (essential foundation)
| Parameter | Value |
|---|---|
| Total CSF volume | ~150 mL |
| Rate of production | ~20 mL/hour (500 mL/day) |
| Site of production | Choroid plexus of lateral ventricles (mainly); ependymal lining |
| Site of absorption | Arachnoid villi along the superior sagittal sinus; brain/cord parenchyma |
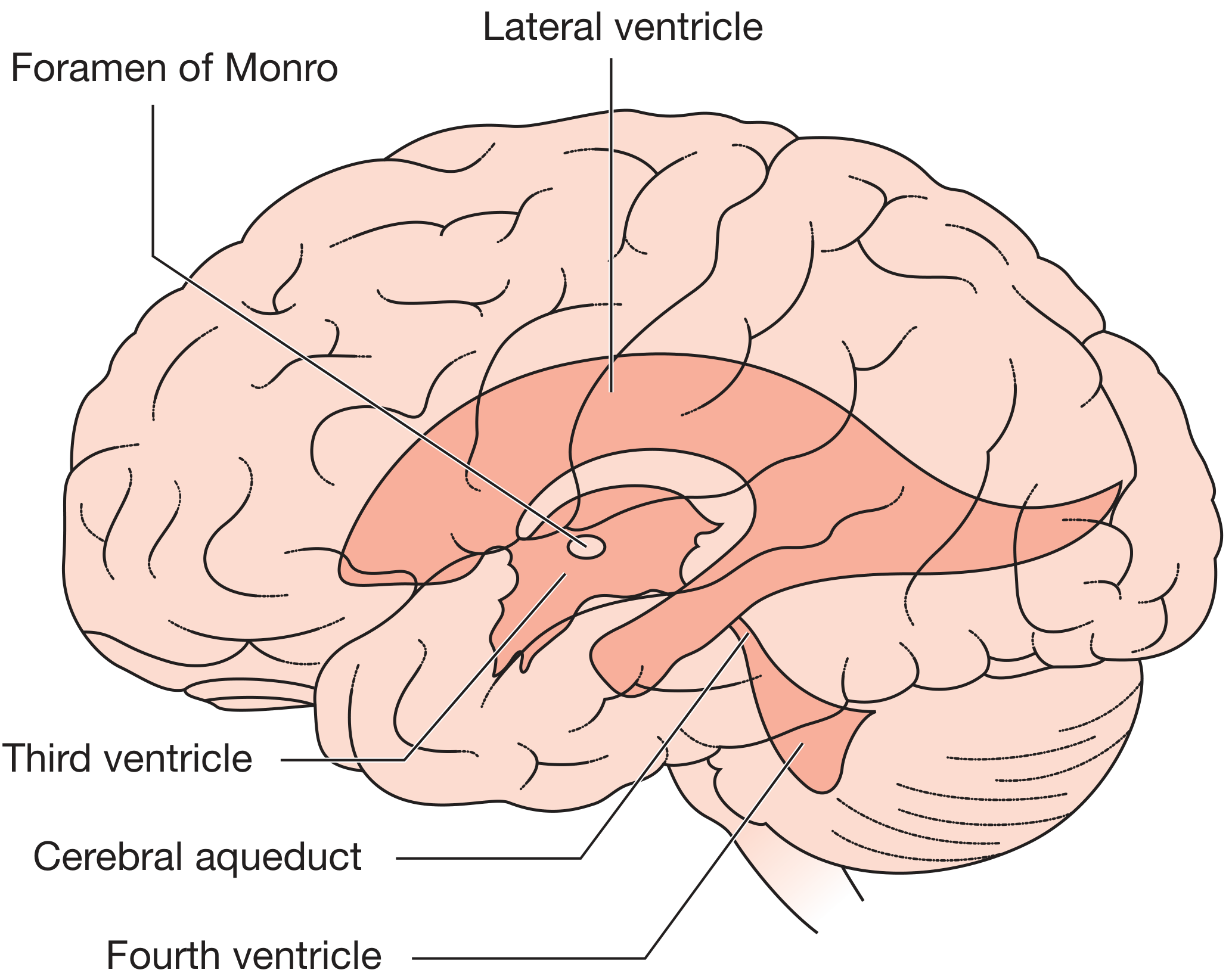
CSF Circulation Pathway:
Lateral ventricles → Foramen of Monro → Third ventricle → Cerebral aqueduct (of Sylvius) → Fourth ventricle → exits via Foramen of Magendie (midline) and Foramina of Luschka (lateral) → Subarachnoid space → Reabsorbed at arachnoid villi
3. Classification
3a. Obstructive (Non-Communicating) Hydrocephalus
- Obstruction lies within the ventricular system - CSF cannot exit the ventricles
- Ventricles proximal to the obstruction dilate; ventricles distal remain normal
- LP carries a risk of herniation (coning) - contraindicated until obstruction excluded
- Causes:
- Lesions within the ventricle (colloid cyst of 3rd ventricle, ependymoma, cysticercosis)
- Lesions in the ventricular wall
- Distant mass with pressure effect
- Aqueductal stenosis (most common cause in children)
- Posterior fossa tumours (cerebellum/brainstem)
- Chiari malformations
3b. Communicating (Extraventricular Obstructive) Hydrocephalus
- Obstruction at or beyond the subarachnoid space - ventricles communicate with each other but drainage is impaired
- Entire ventricular system dilates
- LP is safe and diagnostically useful (opening pressure, CSF analysis, therapeutic drainage)
- Causes:
- Post-haemorrhagic (SAH, IVH)
- Post-infective (meningitis - TB, bacterial, fungal)
- Raised CSF protein
- Leptomeningeal carcinomatosis
3c. Overproduction (rare)
- Choroid plexus papilloma / carcinoma
| Feature | Obstructive | Communicating |
|---|---|---|
| Site of block | Within ventricles | Subarachnoid space |
| LP safety | Contraindicated | Safe |
| Entire ventricular system dilated? | No (only proximal) | Yes |
| Common causes | Aqueductal stenosis, tumours | SAH, meningitis |
4. Aetiology by Age Group
Neonates / Infants (fontanelles open, <2 years)
- Intraventricular haemorrhage (IVH) - especially in premature infants <1500 g; 25% develop progressive ventricular enlargement; 5% require shunting
- Post-infective - in utero infection causing aqueductal scarring/closure
- Aqueductal stenosis/gliosis (congenital or acquired)
- Chiari II malformation (associated with myelomeningocele)
- Dandy-Walker malformation - cystic expansion of 4th ventricle, absent/hypoplastic vermis
- Congenital midline tumours
- Vein of Galen malformation
Older Children (fontanelles closed, >2-3 years)
- Posterior fossa tumours (most common) - medulloblastoma, ependymoma, astrocytoma
- Aqueductal stenosis
- Meningitis
Adults
- Colloid cyst of the third ventricle - ball-valve effect, intermittent/sudden obstruction, risk of sudden death
- Cerebellar haemorrhage or infarction - compresses brainstem, blocks aqueduct and 4th ventricle outflow
- SAH, bacterial/TB/fungal meningitis
- Tumours of basal cisterns
- Normal pressure hydrocephalus (NPH) - idiopathic, or following SAH, head injury, meningitis
5. Clinical Features
In Infants (sutures open)
The hallmark is progressive macrocephaly - head circumference crossing centiles on growth charts.
| Sign | Significance |
|---|---|
| Progressive macrocephaly (head circumference crossing centile) | Most reliable early sign |
| Frontal bossing | Frontal horns dilate first |
| Bulging, tense anterior fontanelle | Even with child upright and relaxed |
| Sutural diastasis | Sutures forced apart |
| Scalp vein engorgement | Raised venous pressure |
| "Sunset sign" / "Setting sun" phenomenon | Downward deviation of eyes due to pressure on superior colliculi - failure of upward gaze |
| Lateral rectus (VI nerve) palsies | False localising sign |
| Lower limb spasticity | Stretching of corticospinal tracts descending around ventricles |
| "Cracked-pot sound" / McEwen sign | Percussion of skull - suture separation |
| Irritability, poor feeding, lethargy | Non-specific raised ICP |
In Older Children (sutures closed)
- Early morning headache, nausea, vomiting (ICP highest on waking)
- Papilloedema
- Diplopia (VI nerve palsy - false localising)
- Visual blurring, ataxia
- Altered conscious level
- Wide-based ataxic gait (stretching of frontal-leg white-matter tracts)
- Deep tendon reflexes increased as spasticity develops
- Long-standing: endocrine dysfunction (short stature, menstrual irregularities, diabetes insipidus) from 3rd ventricle involvement
In Adults (acute)
- Headache, papilloedema, diplopia
- Mental status changes
- Sudden death (severe cases)
- Akinetic mutism (pressure on structures around 3rd ventricle - rare)
- Temporal lobe seizures
- CSF rhinorrhoea
- Endocrine dysfunction (amenorrhoea, polydipsia, polyuria, obesity) - 3rd ventricle dysfunction
6. Normal Pressure Hydrocephalus (NPH)
NPH deserves special emphasis as it is a treatable/reversible cause of dementia.
Classic Triad (Hakim-Adams Triad)
- Gait disturbance - earliest and most prominent feature
- Cognitive decline (frontal-type: apathy, dullness, impaired memory)
- Urinary incontinence (urgency → incontinence → "frontal lobe incontinence")
Gait in NPH
- Unsteady, slow, short steps - difficulty on stairs/curbs
- May superficially resemble Parkinsonism (short steps, stooped posture) but:
- No shuffling or festination
- No rigidity, no resting tremor
- No bradykinesia
- No Babinski signs
- Unexplained falls (often backward)
Aetiology
- Idiopathic (most common)
- Secondary: SAH, head injury, meningitis, tumour
Pathophysiology
- CSF pressure at LP is normal on random measurement
- But: reduced brain compliance causes transient ICP spikes that drive ventricular enlargement
- Ventricular enlargement began at a time of higher pressure; compensatory mechanisms later normalise the measured pressure
Prevalence
- ~0.2% in ages 70-79; ~5.9% in those >80
Diagnosis
- Clinical triad + ventriculomegaly on imaging
- Lumbar infusion/drainage studies - demonstrate altered compliance and/or clinical improvement with CSF removal (30-50 mL tap test)
- Must be distinguished from ventriculomegaly from cortical atrophy
Treatment
- Ventriculoperitoneal (VP) shunt - treatment of choice
- Gait responds best; cognitive and urinary symptoms respond less predictably
7. Investigations
Imaging
CT head (non-contrast):
- First-line for emergency assessment
- Shows ventricular enlargement, periventricular lucency (transependymal oedema)
- Signs of raised ICP (sulcal effacement, loss of basal cisterns)
- Classically in chronic hydrocephalus: erosion of dorsum sellae, copper-beaten skull (less reliable)
MRI brain (preferred where available):
- Superior to CT for posterior fossa, aqueduct, brainstem, Chiari malformations
- Identifies site of obstruction (sagittal T2 best for aqueduct)
- Periventricular interstitial oedema (transependymal flow) on T2/FLAIR
- Identifies underlying cause (tumour, haemorrhage, infection)
- ETV patency: large T2 hypointense flow voids through the ventriculostomy
Specific radiological features of non-communicating hydrocephalus:
- Dilatation of temporal horns disproportionate to lateral ventricular dilatation
- Enlargement of anterior/posterior recesses of 3rd ventricle
- Inferior convexity of the floor of the 3rd ventricle
- Transependymal (periventricular) oedema
- Small/obliterated sulci, fissures, and basal cisterns
Aqueductal stenosis on MRI:
- Lateral + 3rd ventricles dilated; 4th ventricle normal
- Focal narrowing at superior colliculi or intercollicular sulcus on sagittal T2
- Aqueduct dilated proximal to stenosis
Shunt malfunction on imaging:
- Ventricular dilatation (compare with baseline)
- Fluid tracking along shunt tubing
- Plain shunt series (skull to abdomen): assess tubing continuity, kinks, disconnection
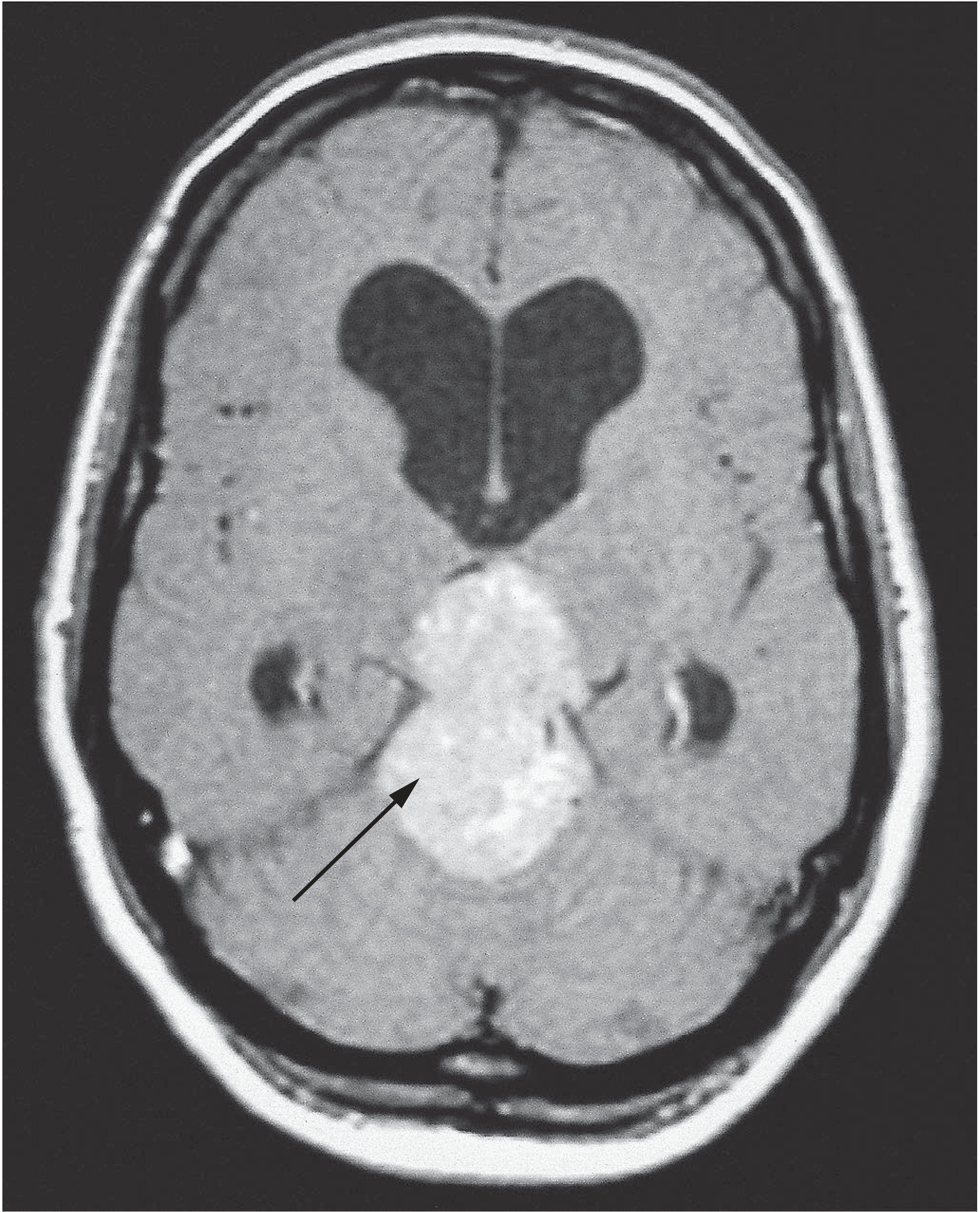
Below: MRI showing a pineal region tumour (arrow) causing obstructive hydrocephalus with gross lateral ventricular dilatation:
CSF Analysis (Lumbar Puncture)
- Only safe in communicating hydrocephalus (LP contraindicated in obstructive/non-communicating hydrocephalus - risk of tonsillar herniation)
- Derives opening pressure
- CSF contents: protein, cells, glucose, culture (TB, bacterial, fungal causes)
- Therapeutic drainage (10-30 mL) can provide temporary relief
8. Treatment
Emergency / Acute
- External ventricular drain (EVD) - immediate CSF diversion
- Management of acute raised ICP (see ICP chapter)
Medical (temporary / adjunctive)
- Acetazolamide (carbonic anhydrase inhibitor) + furosemide - reduce CSF production rate
- Used for slowly progressive hydrocephalus or as a bridge to surgery
Surgical
A. Ventriculoperitoneal (VP) Shunt - the mainstay of surgical treatment
- Most commonly used CSF diversion procedure
- Catheter from lateral ventricle → one-way pressure-sensitive valve → peritoneal cavity
- Programmable valves allow external adjustment of drainage pressure
Shunt Complications:
| Complication | Notes |
|---|---|
| Obstruction/malfunction | Most common; clogging by choroid plexus or glial tissue, kinking, disconnection, migration of proximal/distal tip |
| Infection | Incidence 1-5% (higher in infants); presents as ventriculitis, meningitis; organisms: Staph. epidermidis, Staph. aureus |
| Overdrainage / Slit ventricle syndrome | Chronic headaches without ventricular dilatation; poorly compliant, stiff ventricles |
| Abdominal pseudocyst | Loculated CSF in peritoneum |
| Peritoneal complications | Ascites, perforated viscus (rare) |
| Shunt revision | Required as child grows; recurrent revision is common |
Note: Shunt malfunction in a known VP shunt patient presenting with signs of raised ICP is an emergency - requires urgent neurosurgical review and shunt tap/CT.
B. Ventriculoatrial (VA) Shunt
- CSF drained into the right atrium
- Used when peritoneal cavity not suitable
- Higher risk of cardiac complications (arrhythmia, endocarditis)
C. Endoscopic Third Ventriculostomy (ETV)
- A surgical defect (fenestration) is made in the floor of the third ventricle, allowing CSF to drain into the suprasellar cistern, bypassing the obstruction
- Best suited for non-communicating hydrocephalus with aqueductal obstruction
- Avoids the long-term complications of an indwelling shunt
- ETV patency confirmed on MRI by T2 hypointense flow voids through the fenestration
- Less effective in infants <6 months and post-infective hydrocephalus
D. Surgical removal of obstructing lesion
- Tumours (colloid cyst, posterior fossa tumours) - definitive treatment restores CSF flow
9. Special Scenarios
Colloid Cyst of the Third Ventricle
- Benign mucin-filled cyst at the foramen of Monro
- Acts as a ball valve - intermittently blocks CSF flow
- Presents with positional headaches, sudden loss of consciousness, or sudden death
- Treatment: surgical resection (endoscopic or open)
Dandy-Walker Malformation
- Cystic dilation of the 4th ventricle, aplasia/hypoplasia of the cerebellar vermis, enlarged posterior fossa
- Associated with hydrocephalus in ~80%
Chiari II Malformation
- Associated with myelomeningocele
- Posterior fossa structures herniate through foramen magnum
- Can cause hydrocephalus by obstructing 4th ventricle outlets within the spinal canal
- In shunted patients: enlarged or normal-sized 4th ventricle suggests shunt malfunction or isolated 4th ventricle
- Occipital headaches at night = suspect shunt malfunction + risk of brainstem compression
IVH in Premature Infants
- Germinal matrix haemorrhage - risk highest in <1500 g infants
- 25% develop progressive ventricular enlargement; 5% require VP shunting
- Ventricular size followed by bedside cranial ultrasound through the open fontanelle
10. Key Facts Summary Table
| Feature | Key Point |
|---|---|
| CSF volume | 150 mL total; produced at 20 mL/h |
| Most common cause in children | Aqueductal stenosis (congenital/post-infective) |
| Most common cause of adult acute obstructive hydrocephalus | Posterior fossa tumour, colloid cyst, cerebellar haemorrhage |
| Hallmark sign in infants | Progressive macrocephaly (HC crossing centiles) |
| Sunset sign | Downward gaze deviation - pressure on superior colliculi |
| McEwen sign / "Cracked-pot sound" | Percussion of skull in infant hydrocephalus |
| NPH triad | Gait disturbance → Cognitive decline → Urinary incontinence |
| LP in non-communicating hydrocephalus | Contraindicated (risk of tonsillar herniation) |
| Treatment of choice for hydrocephalus | VP shunt |
| Most common shunt complication | Obstruction/malfunction |
| Shunt infection rate | 1-5% |
| Alternative to VP shunt for aqueductal stenosis | Endoscopic Third Ventriculostomy (ETV) |
| Temp. medical Rx to reduce CSF production | Acetazolamide + furosemide |
| NPH treatment | VP shunt (gait responds best) |
| Dandy-Walker triad | 4th ventricle cyst, cerebellar vermis hypoplasia, enlarged posterior fossa |
Sources: Bailey & Love's Short Practice of Surgery 28e (Ch. 48); Bradley & Daroff's Neurology in Clinical Practice (Ch. 88); Adams & Victor's Principles of Neurology 12e (Ch. 30); Grainger & Allison's Diagnostic Radiology; Harriet Lane Handbook 23e
Brain stem death
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive, high-quality material from multiple authoritative sources. Let me compile the full topic notes.
Brain Stem Death - Comprehensive Topic Notes (PG Level)
Sources: PC Dikshit Forensic Medicine & Toxicology; Plum & Posner's Diagnosis and Treatment of Stupor and Coma; Harrison's Principles of Internal Medicine 22e; Miller's Anesthesia 10e; Essentials of Forensic Medicine & Toxicology 36e (2026)
1. Historical Background
- 1959 - Mollaret and Goulon first described "coma dépassé" (irreversible coma), marking the conceptual birth of brain death
- 1968 - The Harvard Ad Hoc Committee published the first widely accepted criteria for brain death, then called "irreversible coma"
- 1976 - The Conference of Medical Royal Colleges and Faculties of the United Kingdom issued guidelines on brain stem death (regularly updated; used throughout NHS)
- USA - The Uniform Determination of Death Act (UDDA) established that brain death = death of the person
- India - The Transplantation of Human Organs and Tissues Act (THOTA), 1994 (amended 2011) governs brain death certification and organ donation
"The concept of brain death is not simply a convenience invented to satisfy the demands of transplant surgeons." - Dikshit
2. Concepts of Death
| Type | Definition |
|---|---|
| Somatic / Clinical death | Triad of Bichat: irreversible failure of circulation + respiration + enervation (CNS function) |
| Molecular death | Death of individual organs/tissues after cessation of circulation. CNS: irreversible damage within 4 minutes of blood supply cessation |
| Brain stem death | Accepted as synonymous with death. Irreversible loss of all brainstem function - the person can never breathe spontaneously or regain consciousness |
| Apparent death / Suspended animation | Mimics death under special conditions (drowning, hypothermia) - reversible |
| Persistent Vegetative State (PVS) | Severe brain damage NOT involving the brainstem. Patient breathes spontaneously, opens/closes eyes, swallows, grimaces - but no behavioural evidence of awareness |
Key distinction: BSD patients are irrefutably dead. Switching off the ventilator "does not kill the patient but discontinues ventilating a corpse." PVS patients raise the moral dilemma of "allowing someone to die."
3. Why Brain Stem Death = Death
The brainstem:
- Controls respiration (medullary respiratory centres)
- Controls circulation (cardiovascular centres)
- Maintains consciousness (reticular activating system, ARAS)
- Mediates all cranial nerve reflexes
If the brainstem is irreversibly dead → the individual can never breathe spontaneously, maintain independent circulation, or regain consciousness. All other organ function maintained by machine is simply preserving a biological shell.
"All death is brain death. Even if all other organs were artificial, the individual would still be alive. Conversely, when the brain is dead, sustaining other organs is simply preserving a dead body." - Plum & Posner
4. Most Common Causes of Brain Death
(Plum & Posner, Table 10.3)
- Traumatic brain injury (most common overall)
- Aneurysmal subarachnoid haemorrhage
- Intracerebral haemorrhage
- Ischaemic stroke with cerebral oedema and herniation
- Hypoxic-ischaemic encephalopathy (cardiac arrest)
- Fulminant hepatic necrosis with cerebral oedema and raised ICP
5. Prerequisites / Preconditions Before Testing
Before any brainstem death tests are performed, ALL of the following must be satisfied:
5a. The Three Preconditions (UK / Dikshit)
- The patient must be in deep coma
- The patient must be maintained on a mechanical ventilator
- The cause of the coma must be established and irreversible (known structural or metabolic cause)
5b. The Three Exclusions - Conditions That Must Be Ruled Out
These are reversible causes of brainstem depression that can mimic brain death:
- Drug effects - therapeutic drugs (sedatives, anaesthetics, neuromuscular blockers) or overdose (alcohol, opioids, benzodiazepines)
- Hypothermia - core body temperature must be above 35°C (UK) / above 36.5°C (AAN/US). Must warm patient before testing
- Severe metabolic or endocrine disturbances - e.g. severe hypoglycaemia, hyperglycaemic coma, electrolyte disturbances, uraemia, hepatic encephalopathy
Note: Diabetes insipidus is a common complication of severe brain injury. It may appear hours or days after other signs of brain death and is not a diagnostic criterion.
5c. Additional Prerequisites (AAN guidelines, Plum & Posner)
- Systolic BP must be maintained >90 mmHg (dopamine infusion if needed)
- Pre-test arterial blood gases: PaO2 >200 mmHg, PaCO2 ≥40 mmHg
- Euvolemia or positive fluid balance for at least 6 hours before testing
- Cervical spine injury excluded before oculocephalic testing (if trauma suspected)
6. Who Performs the Tests
| Rule | Detail |
|---|---|
| Number of doctors | Two medical practitioners independently |
| Qualifications | Experts in the field; at least one must be of consultant status. Junior doctors are NOT permitted |
| Excluded | Under no circumstances may transplant surgeons perform brain death tests (prevents conflict of interest) |
| Frequency | Each doctor performs the tests twice (two separate sets) |
| India (THOTA Section 5) | A panel of 4 doctors: (1) treating physician, (2) neurologist/neurosurgeon, (3) intensivist/anaesthetist, (4) hospital medical administrator |
7. The Brainstem Death Tests
The diagnosis tests the cranial nerves that pass through the brainstem. All responses must be absent:
| Test | Cranial Nerve Tested | How Performed | Expected Response (normal) | Result in BSD |
|---|---|---|---|---|
| Pupillary light reflex | CN II (afferent), CN III (efferent) | Bright light in each eye | Pupils constrict | Fixed, non-reactive pupils - mid-position (4-6 mm) |
| Corneal reflex | CN V (afferent), CN VII (efferent) | Cotton wisp or gauze to cornea | Blink | Absent |
| Vestibulo-ocular reflex (caloric) | CN VIII (afferent), CN III, IV, VI (efferent) | 20-50 mL ice-cold water into each ear (tympanic membrane confirmed clear); observe for 1 min each side, 5-min interval | Eyes deviate toward cold-water side (nystagmus to opposite side) | No eye movement |
| Oculocephalic reflex ("Doll's eye") | CN VIII / brainstem | Rapidly rotate head side to side (ONLY if C-spine injury excluded) | Eyes move opposite to head rotation | Eyes move with head (absent reflex) |
| Motor response (grimace) | CN V (afferent), CN VII (efferent) | Painful stimulus to supraorbital nerve / temporomandibular joint | Grimacing | No motor response within cranial nerve distribution |
| Gag reflex | CN IX (afferent), CN X (efferent) | Posterior pharynx stimulation | Gagging | Absent |
| Cough reflex | CN X | Suction catheter passed down the trachea | Coughing | Absent |
| Apnoea test | Medullary respiratory centres | See below | Breathing | No respiratory effort |
Key notes on Pupils
- Harvard criteria (1968) required dilated AND fixed pupils
- Current standard: mid-position fixed pupils are more reliable - initially after brain death, agonal catecholamine release dilates pupils, but as catecholamines clear, pupils return to mid-position
- Exclude prior use of mydriatics (atropine), miotic drugs
- Neuromuscular blockers do NOT affect pupil size (nicotinic receptors not present in iris)
8. The Apnoea Test - in Detail
The single most important test - confirms irreversible destruction of medullary respiratory centres.
Rationale
- PaCO2 must rise high enough to maximally stimulate the medullary respiratory centres before declaring them non-functional
- In deep coma, the CO2 threshold for respiratory stimulation may be elevated (up to 50-55 mmHg)
- Rate of rise of PaCO2 during apnoea: ~3 mmHg/min (UK: 2-3 mmHg/min; Harrison's: 2-3 mmHg/min)
Procedure (Apnoeic Oxygenation)
- Pre-oxygenate with 100% oxygen for 10-20 minutes
- Pre-test ABG: confirm PaO2 >200 mmHg, PaCO2 ≥40 mmHg
- Disconnect the ventilator
- Deliver O2 via tracheal catheter at 6 L/min (maintains oxygenation via apnoeic diffusion for ≥1 hour)
- Observe for any chest/abdominal respiratory movements for 8-10 minutes
- At 8 minutes: draw ABG
- Reconnect ventilator
Interpretation
| Result | Meaning |
|---|---|
| No respiratory effort AND PaCO2 ≥60 mmHg (or ≥20 mmHg above baseline) | Positive apnoea test - brainstem respiratory centres non-functional |
| Any respiratory effort seen | Test negative - not brain dead; retest later |
When to stop early
- Cardiovascular instability / hypotension (SBP <90 mmHg) during test
- Severe hypoxia (SpO2 falls critically)
- Arrhythmia
Special situation: ECMO patients
- Traditional apnoea testing cannot be performed on ECMO - ancillary testing required
9. Spinal Reflex Activity - a Critical Pitfall
After brain death, the spinal cord remains functional. The following may be observed and should not preclude diagnosis of brain death:
- Deep tendon reflexes may be present
- Plantar responses: flexor, absent, or toe undulations (NOT Babinski - extensor plantar NOT expected in brain death)
- "Lazarus sign" - arms rise and cross over the chest, or body slowly rises to a sitting position - spinally mediated, not a sign of brain function
- Stepping movements
- Body movements synchronous with ventilator
These spinally mediated movements are generated by the spinal cord below the level of the brainstem and do not represent residual brain function.
10. Interval Between the Two Examinations
(AAN guidelines, Plum & Posner - Table 10.2)
| Age | Minimum interval |
|---|---|
| Term newborn to 2 months | 48 hours |
| >2 months to 1 year | 24 hours |
| >1 year to <18 years | 12 hours |
| ≥18 years (adults) | Optional (6-hour observation acceptable) |
- For anoxic brain injury (cardiac arrest, diffuse insult): minimum 24-hour observation before final diagnosis
- For identified structural injury: shorter evaluation periods acceptable
- For cases with possible drug exposure: 6-hour period of observation (AAN)
11. Confirmatory (Ancillary) Tests
These are optional in adults but mandatory in neonates/young infants. Used when:
- Clinical examination is incomplete (facial trauma, perforated tympanic membrane precluding caloric testing)
- Chronic hypercapnia complicates apnoea testing
- ECMO patients
| Test | What It Shows |
|---|---|
| EEG (electroencephalogram) | Isoelectric (flat) EEG - confirms absence of cortical electrical activity |
| Cerebral angiography (4-vessel) | Absence of intracranial blood flow - gold standard confirmatory test |
| Radionuclide brain scan (HMPAO scan) | No cerebral perfusion ("hollow skull" or "empty light bulb" sign) |
| Transcranial Doppler (TCD) | Absent or reverberant flow; systolic spikes only |
| CT angiography | Absent intracranial enhancement |
| Auditory/Visual Evoked Potentials | Absent responses |
Note: A normal EEG does not exclude brain death in primary brainstem lesions (brainstem may be dead while cortex temporarily shows electrical activity).
12. Certification of Death
- Once both doctors have performed the tests twice and all are negative → patient is pronounced dead
- A death certificate is issued at this point
- The time of death is recorded as the time the first set of tests confirmed brainstem death (not the time the ventilator is switched off)
- After certification, a decision regarding organ donation may be raised and consent obtained from the family
13. Legal Framework
United Kingdom
- UK Human Tissue Act 1961: If a person in writing or orally (in presence of 2+ witnesses) during life requested organ donation, organs may be used after death
- Brain stem death guidelines issued by Conference of Medical Royal Colleges (1976, updated regularly)
India - THOTA 1994 (amended 2011)
Full name: Transplantation of Human Organs and Tissues Act, 1994
Key definitions under THOTA:
- Human organ: Heart, kidneys, liver, lungs, pancreas + other government-specified organs
- Tissue: Cornea, bone, skin, blood vessels
- Near relative: Spouse, parents, siblings, children, grandparents, grandchildren
- Brain stem death: Irreversible loss of brain function while maintaining cardiac function (for deceased donation)
- Registered Medical Practitioner (RMP): Doctor recognised to certify brain death
Brain death certification panel (Section 5): 4 doctors:
- Treating physician (in charge of the patient)
- Neurologist or neurosurgeon
- Intensivist or anaesthetist
- Hospital medical administrator (or nominee)
Key provisions:
- Section 3: Prohibition of organ removal without authority
- Section 4: Living donor transplantation conditions (near relatives without committee; non-relatives need authorisation committee)
- Section 9: Prohibition of buying/selling human organs - up to 10 years imprisonment + fine up to ₹1 crore
- Section 13: Deceased donation requires lifetime consent OR next-of-kin consent
- Section 15: NOTTO/SOTTO for fair organ allocation
- "Required request" policy - hospitals must ask about organ donation in brain death cases
USA
- Uniform Determination of Death Act (UDDA): Brain death = legal death of the person
- AAN guidelines (reviewed 2010) govern clinical diagnosis
14. Brain Death and Organ Donation
- Most transplanted organs in the US/UK come from Donation after Brain Death (DBD) donors
- Donation after Circulatory Death (DCD): organs retrieved after planned withdrawal of life support and cardiac arrest - obligatory warm ischaemia period
- Brain-dead donors have significant physiological alterations that must be actively managed:
- Haemodynamic instability (loss of sympathetic tone, diabetes insipidus)
- Endocrine changes (DI, hypothyroidism, adrenal failure)
- Neurogenic pulmonary oedema
- Coagulopathy
- Goal-directed donor management improves number of transplantable organs per donor
- Organ viability after brain death (approximate cold ischaemia tolerance):
- Cornea: viable up to 24 hours
- Heart: most sensitive - very short ischaemia tolerance
- Kidney: most tolerant - can be preserved for hours
15. Brain Death vs. Persistent Vegetative State - Key Comparisons
| Feature | Brain Stem Death | Persistent Vegetative State |
|---|---|---|
| Brainstem function | Completely absent | Intact |
| Spontaneous breathing | Absent | Present |
| Eye opening | Absent | Present (sleep-wake cycles) |
| Cranial nerve reflexes | All absent | Present |
| Legal status | Dead | Alive |
| Consciousness | Permanently absent | No behavioural evidence of awareness |
| Ventilator dependence | Yes (for breathing) | No (breathes spontaneously) |
| Ethical dilemma | None (already dead) | "Allowing someone to die" |
16. Summary Table - Brainstem Reflexes Tested
| Reflex | Stimulus | Brainstem Level | Cranial Nerves |
|---|---|---|---|
| Pupillary light | Bright light | Midbrain (CN III nucleus) | II → III |
| Corneal | Touch cornea | Pons | V → VII |
| Vestibulo-ocular (caloric) | Cold water in ear | Pons (MLF) | VIII → III/IV/VI |
| Oculocephalic (Doll's eye) | Head rotation | Pons (MLF) | VIII → III/VI |
| Grimace to pain | Supraorbital pressure | Pons | V → VII |
| Gag | Posterior pharynx | Medulla | IX → X |
| Cough | Tracheal suction | Medulla | X → X |
| Apnoea | Hypercapnia (PaCO2 ≥60) | Medulla oblongata | - |
17. Quick-Reference Key Facts
| Point | Answer |
|---|---|
| Year BSD concept first described | 1959 (Mollaret & Goulon) |
| Harvard criteria year | 1968 |
| UK Royal Colleges guidelines | 1976 |
| India's law on brain death | THOTA 1994 |
| Number of doctors for BSD tests (India) | 4 |
| Minimum temperature for testing | >35°C (UK); >36.5°C (AAN) |
| BSD tests performed how many times? | Twice by each of 2 doctors |
| Can a transplant surgeon perform BSD tests? | No - absolutely prohibited |
| PaCO2 threshold for apnoea test | ≥60 mmHg (or ≥20 mmHg above baseline) |
| Rate of PaCO2 rise during apnoea | ~3 mmHg/min |
| Pre-oxygenation before apnoea test | 100% O2 for 10-20 min |
| O2 flow via tracheal catheter during apnoea | 6 L/min |
| "Lazarus sign" | Spinal reflex - NOT a sign of brain function |
| Gold standard confirmatory test | 4-vessel cerebral angiography (absent intracranial flow) |
| EEG in BSD | Isoelectric/flat (optional confirmatory) |
| Time of death is recorded as | Time of first positive test set (not ventilator withdrawal) |
| Interval between tests in adults | Optional (6-hour observation acceptable) |
| Interval in term newborns - 2 months | 48 hours |
Sources: PC Dikshit Textbook of Forensic Medicine & Toxicology; Plum & Posner's Diagnosis and Treatment of Stupor and Coma; Harrison's Principles of Internal Medicine 22e; Miller's Anesthesia 10e; Essentials of Forensic Medicine & Toxicology 36e (2026)
This is a shared conversation. Sign in to Orris to start your own chat.