Explain baroreceptor for physiology 1st year mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have everything needed to write a thorough, exam-oriented answer for 1st year MBBS. Let me compile the comprehensive response.
Baroreceptors - Complete Guide for 1st Year MBBS
(Sources: Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition)
1. Definition
Baroreceptors (also called pressoreceptors) are spray-type mechanoreceptive nerve endings located in the walls of large arteries. They are stretch-sensitive - when arterial pressure rises, the vessel wall stretches and the receptors fire. They form the afferent arm of the baroreceptor reflex, the body's most important rapid mechanism for short-term blood pressure control.
2. Location
There are two major sites:
| Location | Details |
|---|---|
| Carotid Sinus | Wall of each internal carotid artery, just above the carotid bifurcation (the widened portion). Most important baroreceptor zone. |
| Aortic Arch | Wall of the aortic arch. Functional similar to carotid but operates ~30 mmHg higher. |
A few baroreceptors also lie in the walls of almost every large artery of the thoracic and neck regions, but the above two are the main ones.
Anatomical diagram from Guyton & Hall (Fig. 18.5):
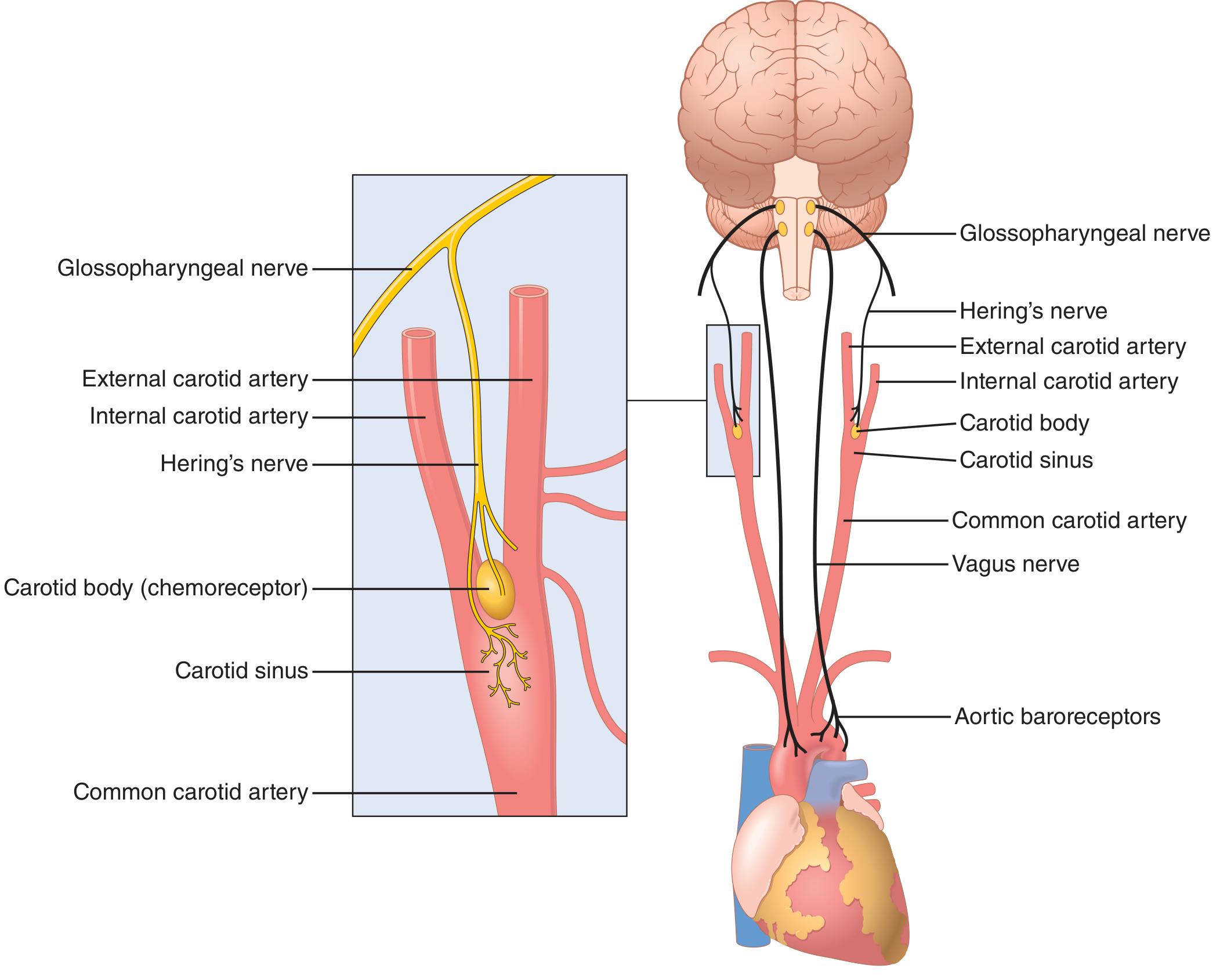
3. Innervation (Afferent Pathway)
| Source | Nerve | Destination |
|---|---|---|
| Carotid sinus baroreceptors | Hering's nerve → Glossopharyngeal nerve (CN IX) | Nucleus Tractus Solitarius (NTS) in medulla |
| Aortic arch baroreceptors | Vagus nerve (CN X) | Nucleus Tractus Solitarius (NTS) in medulla |
The Nucleus Tractus Solitarius (NTS) is the first relay station in the medulla. It processes baroreceptor input and coordinates the efferent response through cardiovascular centers.
4. Mechanism of Action (Receptor Properties)
Baroreceptors are mechanoreceptors - a rise in arterial pressure stretches the vessel wall, deforming the nerve endings and generating a receptor potential (depolarization). This increases action potential frequency in the afferent nerve.
Key properties (high-yield for exams):
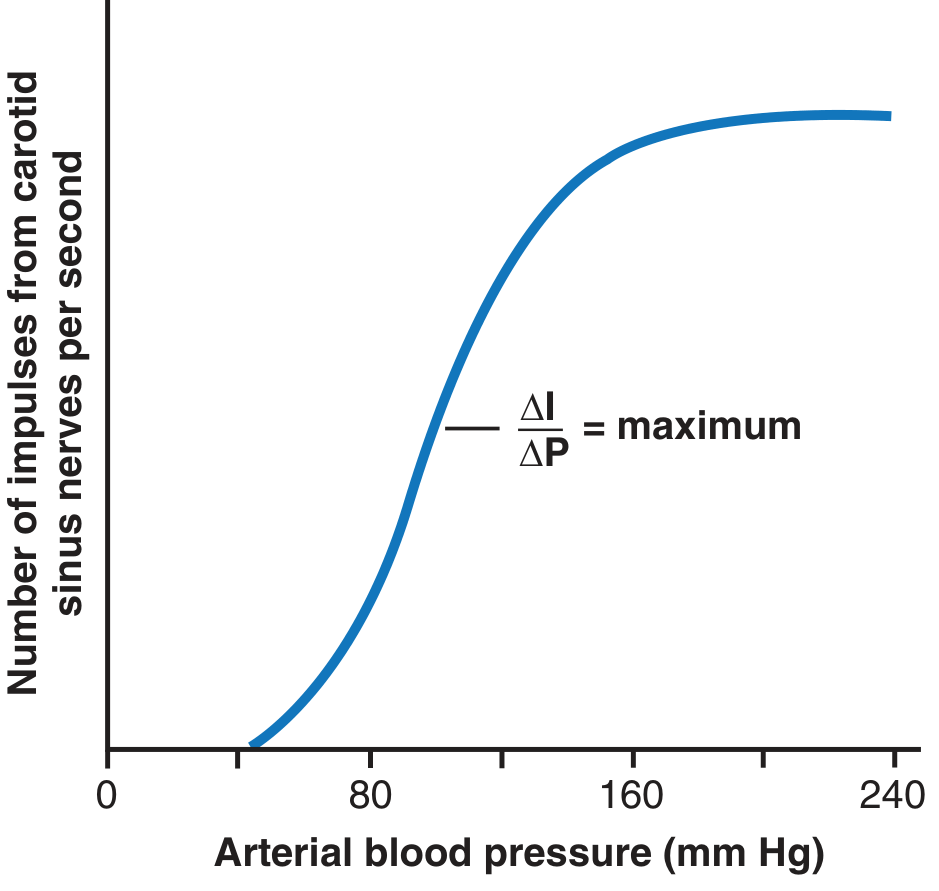
- Threshold: Carotid sinus receptors begin firing at ~60 mmHg; no firing below 50-60 mmHg
- Maximum response: Firing saturates around 180 mmHg
- Most sensitive: Around 100 mmHg (normal mean arterial pressure) - the slope ΔI/ΔP is steepest here
Firing rate vs. arterial pressure graph (Guyton & Hall, Fig. 18.6):
- Dynamic sensitivity: Baroreceptors respond more to rapidly changing pressure than to a steady pressure. A rapidly rising pressure produces ~twice the firing compared to the same pressure held steady. This makes them ideal for detecting sudden BP fluctuations.
- Pulse pressure sensitivity: Firing increases during systole and decreases during diastole - so they also respond to pulse pressure.
- Carotid vs. Aortic:
- Carotid sinus: responds to both increases AND decreases
- Aortic arch: primarily responds to increases in arterial pressure
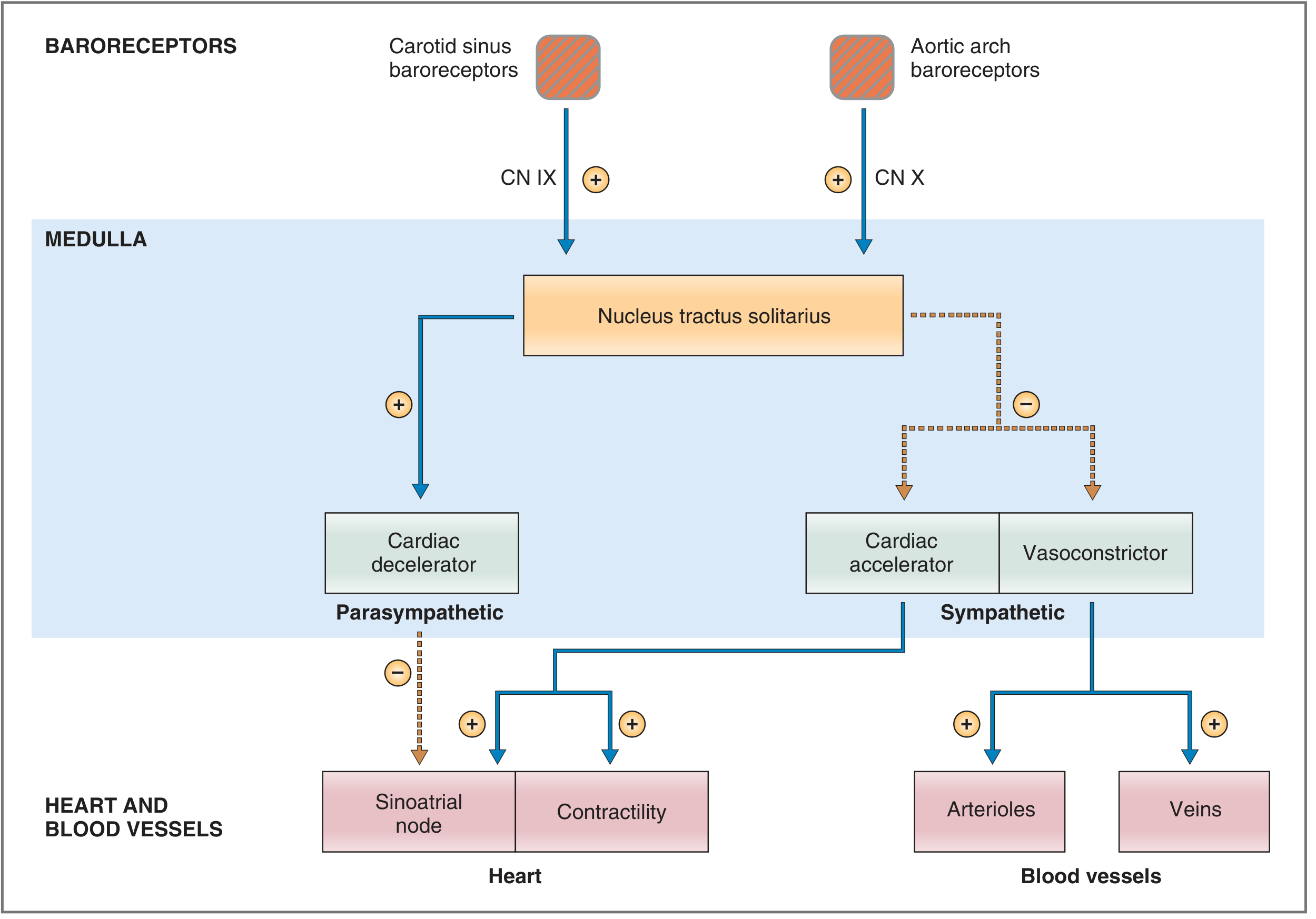
5. Central Processing
Brain stem cardiovascular centers (in the reticular formation of the medulla and lower pons):
- Vasoconstrictor center (C1) - upper medulla/lower pons; sympathetic outflow to arterioles and venules
- Cardiac accelerator center - sympathetic; increases SA node firing rate (HR), AV conduction, and contractility
- Cardiac decelerator center - parasympathetic (vagus nerve); decreases SA node firing rate (HR)
The NTS coordinates these centers' outputs based on incoming baroreceptor signals.
6. The Baroreceptor Reflex (Complete Reflex Arc)
This is the full feedback loop (most important topic for exams):
Reflex arc diagram from Costanzo (Fig. 4.31):
Response to INCREASED Arterial Pressure (e.g., after giving a vasopressor):
- ↑ BP → ↑ stretch on carotid sinus/aortic arch baroreceptors
- ↑ Firing rate in CN IX and CN X afferents → NTS activated
- NTS directs:
- ↑ Parasympathetic (vagal) outflow to SA node → ↓ Heart rate
- ↓ Sympathetic outflow to heart → ↓ Heart rate + ↓ Contractility → ↓ Cardiac output
- ↓ Sympathetic outflow to arterioles → Vasodilation → ↓ Total Peripheral Resistance (TPR)
- ↓ Sympathetic outflow to veins → Venodilation → ↑ Unstressed volume → ↓ Venous return → ↓ CO
- Net result: ↓ CO and ↓ TPR → BP returns toward normal
Response to DECREASED Arterial Pressure (e.g., hemorrhage):
Flow diagram from Costanzo:
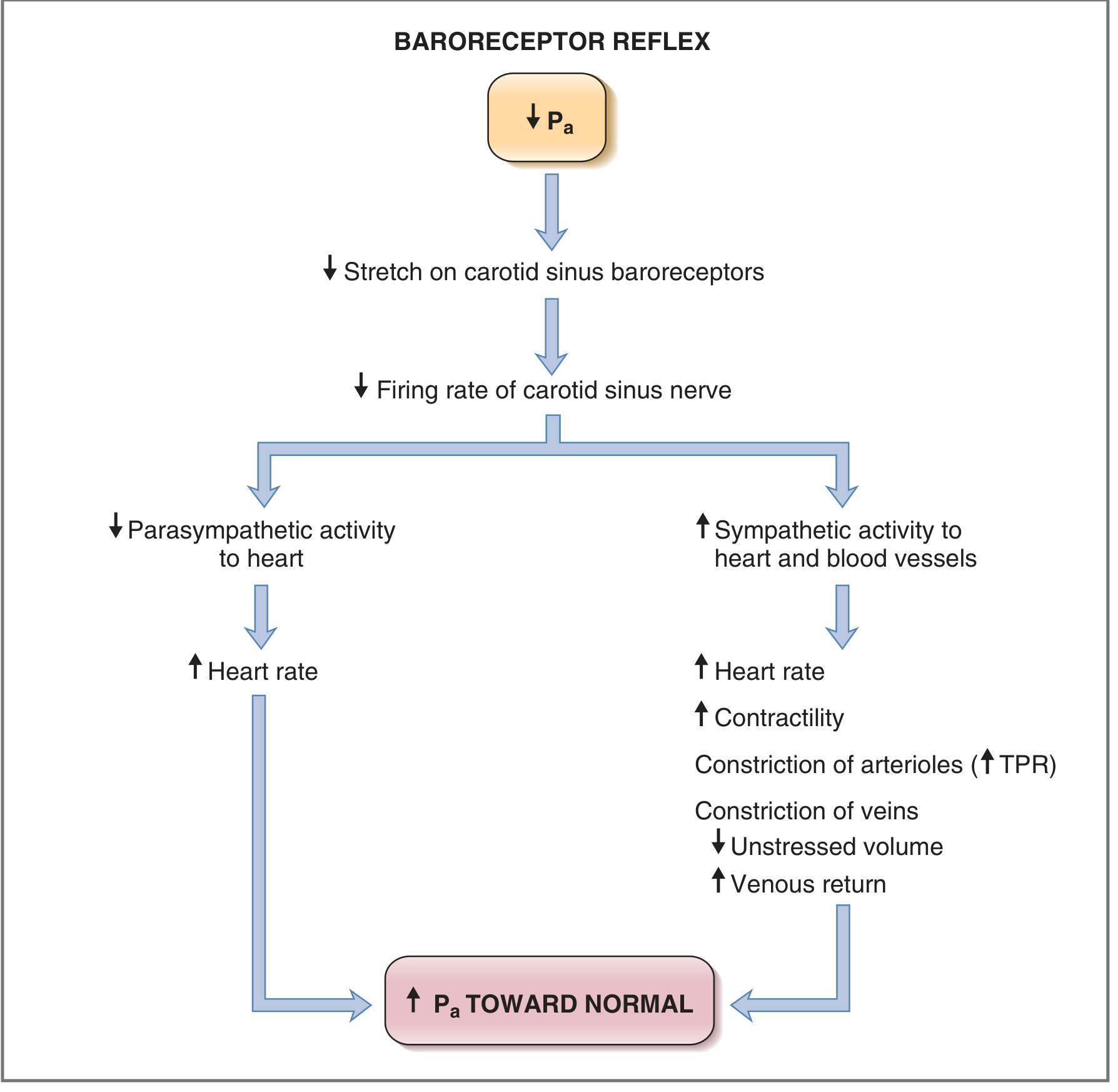
- ↓ BP → ↓ stretch on baroreceptors
- ↓ Firing rate in afferents → NTS less activated
- NTS directs:
- ↓ Parasympathetic outflow to SA node → ↑ Heart rate
- ↑ Sympathetic outflow to heart → ↑ Heart rate + ↑ Contractility → ↑ Cardiac output
- ↑ Sympathetic outflow to arterioles → Vasoconstriction → ↑ TPR
- ↑ Sympathetic outflow to veins → Venoconstriction → ↑ Venous return → ↑ CO
- Net result: ↑ CO and ↑ TPR → BP rises back toward normal
7. Summary Table: Baroreceptor Response
| Parameter | ↑ BP (Hypertension response) | ↓ BP (Hypotension response) |
|---|---|---|
| Baroreceptor firing | ↑ | ↓ |
| Parasympathetic tone | ↑ | ↓ |
| Sympathetic tone | ↓ | ↑ |
| Heart rate | ↓ | ↑ |
| Contractility | ↓ | ↑ |
| Cardiac output | ↓ | ↑ |
| TPR (arterioles) | ↓ (vasodilation) | ↑ (vasoconstriction) |
| Venous tone | ↓ (venodilation) | ↑ (venoconstriction) |
| Net BP effect | Falls toward normal | Rises toward normal |
8. Important Clinical & Physiological Applications
A. Orthostatic Hypotension Prevention
When you stand up from lying down, gravity pools blood in the legs, reducing venous return and BP. Baroreceptors sense this drop and immediately trigger sympathetic activation - raising HR, CO, and TPR to maintain cerebral perfusion. Failure of this reflex causes orthostatic (postural) hypotension and fainting.
B. Pressure Buffer Function
Because the reflex always opposes pressure changes (up or down), baroreceptors are called a pressure buffer system and the afferent nerves are called buffer nerves. When baroreceptors are denervated experimentally, blood pressure becomes extremely labile - swinging widely throughout the day.
C. Chronic Hypertension and "Resetting"
In chronic hypertension, baroreceptors reset to the new (elevated) pressure level. They no longer treat 160 mmHg as too high - the set point shifts. This is why the baroreceptor reflex maintains, rather than corrects, chronic hypertension. The mechanism is either decreased baroreceptor sensitivity or a changed set point in the NTS.
D. Valsalva Maneuver (Test of Baroreceptor Reflex)
Expiring forcefully against a closed glottis (as in coughing, straining at defecation, or heavy lifting):
- ↑ Intrathoracic pressure → ↓ Venous return → ↓ CO → ↓ BP
- Baroreceptor reflex is triggered → ↑ HR + vasoconstriction
- On release: BP overshoots upward → baroreceptors cause reflex bradycardia
- A normal 4-phase Valsalva response confirms intact baroreceptor reflex. Used clinically to assess autonomic function.
E. Carotid Sinus Hypersensitivity
External pressure on the carotid sinus (e.g., tight collar, neck massage) can cause exaggerated baroreceptor firing → sudden bradycardia and hypotension → syncope (fainting). Explains why pressing on the neck can cause fainting.
9. Limitations of the Baroreceptor Reflex
- Effective only for short-term BP control - the reflex adapts/resets within 1-3 days; it cannot regulate long-term BP (kidneys handle that)
- Loses effectiveness below ~50 mmHg - no receptor firing at very low pressures, so no reflex correction during severe shock
- Does not control long-term mean arterial pressure - only buffers acute changes
Quick Recall (Exam Summary)
| Feature | Detail |
|---|---|
| Type | Mechanoreceptor (stretch receptor), spray-type nerve ending |
| Locations | Carotid sinus (CN IX), Aortic arch (CN X) |
| Afferent nerves | Hering's nerve → CN IX (carotid); CN X (aortic) |
| Central relay | Nucleus Tractus Solitarius (NTS), medulla |
| Efferent | Sympathetic + Parasympathetic nervous system |
| Function | Short-term (acute) blood pressure regulation |
| Threshold | No firing <50-60 mmHg; maximum ~180 mmHg |
| Most sensitive at | ~100 mmHg (normal MAP) |
| Adaptation | Resets in 1-3 days → not for long-term BP |
| Also called | Pressoreceptors; buffer nerves (afferents) |
- Guyton and Hall Textbook of Medical Physiology, pp. 227-228
- Costanzo Physiology 7th Edition, pp. 169-172
Make its consize form for easy learning and good marks scoring
Baroreceptors - Concise Notes for MBBS Exams
What & Where
- Stretch receptors (spray-type nerve endings) in artery walls
- Detect changes in blood pressure by sensing vessel wall stretch
- Two main locations:
| Location | Nerve | CN |
|---|---|---|
| Carotid sinus (above carotid bifurcation) | Hering's nerve | CN IX (Glossopharyngeal) |
| Aortic arch | Vagus nerve | CN X |
Both send signals → Nucleus Tractus Solitarius (NTS), medulla
Key Properties (High-Yield)
- Fire between 60-180 mmHg; no firing below 50 mmHg
- Most sensitive at ~100 mmHg (normal MAP) - best buffer zone
- Respond MORE to rapidly changing pressure than steady pressure
- Carotid sinus → responds to both ↑ and ↓ BP
- Aortic arch → mainly responds to ↑ BP only
The Reflex (Core Concept)
ONE RULE: High BP → baroreceptors fire more → BP brought DOWN. Low BP → baroreceptors fire less → BP brought UP.
↑ BP → Reflex to LOWER it
↑ BP → ↑ baroreceptor firing → NTS activated
→ ↑ Parasympathetic + ↓ Sympathetic
→ ↓ HR, ↓ Contractility, Vasodilation
→ ↓ CO + ↓ TPR → BP normalizes
↓ BP → Reflex to RAISE it
↓ BP → ↓ baroreceptor firing → NTS less active
→ ↓ Parasympathetic + ↑ Sympathetic
→ ↑ HR, ↑ Contractility, Vasoconstriction, Venoconstriction
→ ↑ CO + ↑ TPR → BP normalizes
Master Summary Table
| BP Change | Baroreceptor Firing | Para | Sympa | HR | CO | TPR |
|---|---|---|---|---|---|---|
| ↑ BP | ↑ | ↑ | ↓ | ↓ | ↓ | ↓ |
| ↓ BP | ↓ | ↓ | ↑ | ↑ | ↑ | ↑ |
Memory trick: Think of baroreceptors as a see-saw - when BP goes up, everything that raises BP goes down, and vice versa.
Medullary Centers (Efferent Side)
| Center | Type | Effect |
|---|---|---|
| Vasoconstrictor (C1) | Sympathetic | Constricts arterioles + venules |
| Cardiac Accelerator | Sympathetic | ↑ HR, ↑ contractility |
| Cardiac Decelerator | Parasympathetic (vagus) | ↓ HR |
Clinical Points (Exam Favorites)
| Scenario | Mechanism | Result |
|---|---|---|
| Standing up | BP falls → reflex activates | ↑ HR + vasoconstriction prevents fainting |
| Orthostatic hypotension | Reflex fails on standing | Dizziness/syncope |
| Carotid sinus pressure (tight collar, massage) | Exaggerated baroreceptor firing | Bradycardia + hypotension → syncope |
| Chronic hypertension | Baroreceptors reset to new high level | Reflex now maintains high BP instead of correcting it |
| Hemorrhage/shock | ↓ BP → reflex raises HR + vasoconstriction | Compensatory response |
| Valsalva maneuver | Straining → ↓ venous return → ↓ BP → reflex ↑ HR; on release → BP overshoots → reflex bradycardia | Clinical test of baroreceptor integrity |
Limitations (Short Answer Favorite)
- Controls acute/short-term BP only - NOT long-term
- Resets within 1-3 days - adapts to new pressure level
- Fails below 50 mmHg (severe shock)
- Long-term BP = kidneys (pressure natriuresis)
One-Line Definitions for Viva
- Baroreceptors = stretch receptors in carotid sinus + aortic arch that detect BP changes
- Hering's nerve = afferent nerve from carotid sinus → CN IX
- Buffer nerves = another name for baroreceptor afferent nerves (they buffer BP changes)
- NTS = first brainstem relay for baroreceptor signals
- Resetting = adaptation of baroreceptors to chronic hypertension
Rapid Recall Box
LOCATION → Carotid sinus (CN IX) + Aortic arch (CN X)
RELAY → NTS, medulla
RANGE → 60 - 180 mmHg; best at 100 mmHg
FUNCTION → Short-term (acute) BP control
LIMITS → Resets in 1-3 days; fails <50 mmHg
ALSO CALLED → Pressoreceptors / Buffer nerves
For theory exam
Baroreceptors — Theory Exam Answer
(Structured for 5/10 mark questions | MBBS 1st Year)
Introduction
Baroreceptors are mechanoreceptors (stretch receptors) present in the walls of large arteries. They detect changes in arterial blood pressure and initiate the baroreceptor reflex — the most important neural mechanism for short-term regulation of arterial blood pressure.
Location and Innervation
Baroreceptors are found in two main sites:
1. Carotid Sinus
- Located in the wall of the internal carotid artery, just above the carotid bifurcation
- Afferent nerve: Hering's nerve → Glossopharyngeal nerve (CN IX)
2. Aortic Arch
- Located in the wall of the aortic arch
- Afferent nerve: Vagus nerve (CN X)
Both sets of afferents terminate in the Nucleus Tractus Solitarius (NTS) in the medulla oblongata.
A few baroreceptors are also present in the walls of other large thoracic and cervical arteries, but the above two are physiologically most significant.
Structure
Baroreceptors are spray-type nerve endings lying in the tunica adventitia of the arterial wall. They are not specialized end-organs but free nerve terminals that deform when the vessel wall stretches.
Stimulus and Response Properties
Baroreceptors are stimulated by stretch of the vessel wall, which occurs when arterial pressure rises.
| Property | Detail |
|---|---|
| Type of receptor | Mechanoreceptor |
| Adequate stimulus | Stretch of arterial wall (due to ↑ BP) |
| Threshold | ~60 mmHg (no firing below 50 mmHg) |
| Maximum response | ~180 mmHg |
| Most sensitive zone | Around 100 mmHg (normal MAP) — steepest part of the curve |
| Dynamic sensitivity | Respond more to rapidly changing pressure than steady pressure |
The relationship between firing rate and arterial pressure follows a sigmoid (S-shaped) curve — the steepest (most sensitive) portion corresponds to the normal operating range of blood pressure (~100 mmHg), making the reflex maximally effective under normal physiological conditions.
Afferent Pathway
Carotid sinus baroreceptors
↓
Hering's nerve → CN IX (Glossopharyngeal)
↓
Nucleus Tractus Solitarius (NTS), Medulla
Aortic arch baroreceptors
↓
Vagus nerve (CN X)
↓
Nucleus Tractus Solitarius (NTS), Medulla
Central Integration — Brain Stem Centers
The NTS processes baroreceptor input and modulates three medullary cardiovascular centers:
| Center | Autonomic Type | Action |
|---|---|---|
| Vasoconstrictor center (C1) | Sympathetic | Controls arteriolar and venous tone |
| Cardiac accelerator center | Sympathetic | ↑ HR and ↑ contractility |
| Cardiac decelerator center | Parasympathetic (Vagus) | ↓ HR |
The Baroreceptor Reflex
Response to RISE in Arterial Pressure
Example: Sudden injection of a vasopressor drug
- ↑ Arterial pressure → ↑ stretch on carotid sinus and aortic arch
- ↑ Firing rate in CN IX and CN X afferents
- NTS activated → coordinates efferent response:
- ↑ Parasympathetic outflow to SA node → ↓ Heart rate
- ↓ Sympathetic outflow to heart → ↓ Heart rate + ↓ Contractility → ↓ Cardiac output
- ↓ Sympathetic outflow to arterioles → Vasodilation → ↓ Total Peripheral Resistance (TPR)
- ↓ Sympathetic outflow to veins → Venodilation → ↓ Venous return → further ↓ CO
- ↓ Cardiac output + ↓ TPR → Arterial pressure returns toward normal
(Since: Mean Arterial Pressure = Cardiac Output × TPR)
Response to FALL in Arterial Pressure
Example: Acute hemorrhage
- ↓ Arterial pressure → ↓ stretch on baroreceptors
- ↓ Firing rate in afferents
- NTS less activated → coordinates opposite response:
- ↓ Parasympathetic outflow → ↑ Heart rate
- ↑ Sympathetic outflow to heart → ↑ Heart rate + ↑ Contractility → ↑ Cardiac output
- ↑ Sympathetic outflow to arterioles → Vasoconstriction → ↑ TPR
- ↑ Sympathetic outflow to veins → Venoconstriction → ↑ Venous return → ↑ CO (Frank-Starling)
- ↑ Cardiac output + ↑ TPR → Arterial pressure rises back toward normal
Summary Comparison Table
| Parameter | ↑ BP Response | ↓ BP Response |
|---|---|---|
| Baroreceptor firing | ↑ | ↓ |
| Parasympathetic | ↑ | ↓ |
| Sympathetic | ↓ | ↑ |
| Heart rate | ↓ | ↑ |
| Contractility | ↓ | ↑ |
| Cardiac output | ↓ | ↑ |
| TPR | ↓ | ↑ |
| Venous return | ↓ | ↑ |
| Net BP change | ↓ toward normal | ↑ toward normal |
Physiological Significance
1. Pressure Buffer Function
The baroreceptor system acts as a pressure buffer — opposing any sudden rise or fall in BP. The afferent nerves are therefore also called buffer nerves. Without them, BP fluctuates wildly throughout the day.
2. Postural Regulation
On standing, BP tends to fall due to venous pooling in the legs. The baroreceptor reflex immediately increases sympathetic tone, preventing cerebral hypoperfusion.
3. Response to Hemorrhage
Acute blood loss reduces BP → baroreceptor reflex raises HR and causes vasoconstriction to compensate. This is the immediate hemodynamic response to blood loss.
Applied Physiology
| Condition | Mechanism | Effect |
|---|---|---|
| Carotid sinus hypersensitivity | Exaggerated baroreceptor firing with neck pressure | Sudden bradycardia + hypotension → syncope |
| Orthostatic hypotension | Impaired baroreceptor reflex on standing | Dizziness, fainting on rising |
| Chronic hypertension | Baroreceptors reset to new elevated set point | Reflex maintains high BP instead of correcting it |
| Valsalva maneuver | Straining → ↓ venous return → ↓ BP → reflex ↑ HR; on release, BP overshoots → reflex bradycardia | Clinical test of baroreceptor reflex integrity |
Limitations
- Controls only acute (short-term) blood pressure changes
- Resets within 1-3 days of sustained pressure change — cannot regulate long-term BP
- Ineffective below 50 mmHg (baroreceptors stop firing in severe shock)
- Long-term blood pressure regulation is handled by the kidneys (pressure natriuresis)
Conclusion
Baroreceptors form the afferent limb of a powerful negative feedback reflex that maintains arterial blood pressure within the normal range on a moment-to-moment basis. By sensing vessel wall stretch and modulating both sympathetic and parasympathetic output via medullary centers, they provide rapid and effective short-term blood pressure homeostasis. Their limitation is an inability to reset the long-term pressure set point, which is the domain of renal mechanisms.
Exam tip: For a 10-mark question, write all sections above. For a 5-mark question, write: Introduction + Location + The Reflex (both responses as flow diagrams) + Significance + Limitations. Diagrams of the reflex arc and sigmoid firing curve always fetch extra marks.
This is a shared conversation. Sign in to Orris to start your own chat.