PCOD SIGN AND SYMPTOMS
Reading File
Finding Sources
Searching PubMed
"polycystic ovary syndrome" signs symptoms diagnosis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I have comprehensive information now. Let me compile the full answer.
PCOD / PCOS - Signs and Symptoms
PCOD (Polycystic Ovarian Disease) and PCOS (Polycystic Ovary Syndrome) refer to the same condition - the most common endocrine disorder in women of reproductive age, affecting 5-10% of women worldwide. It was first described by Stein and Leventhal in 1935.
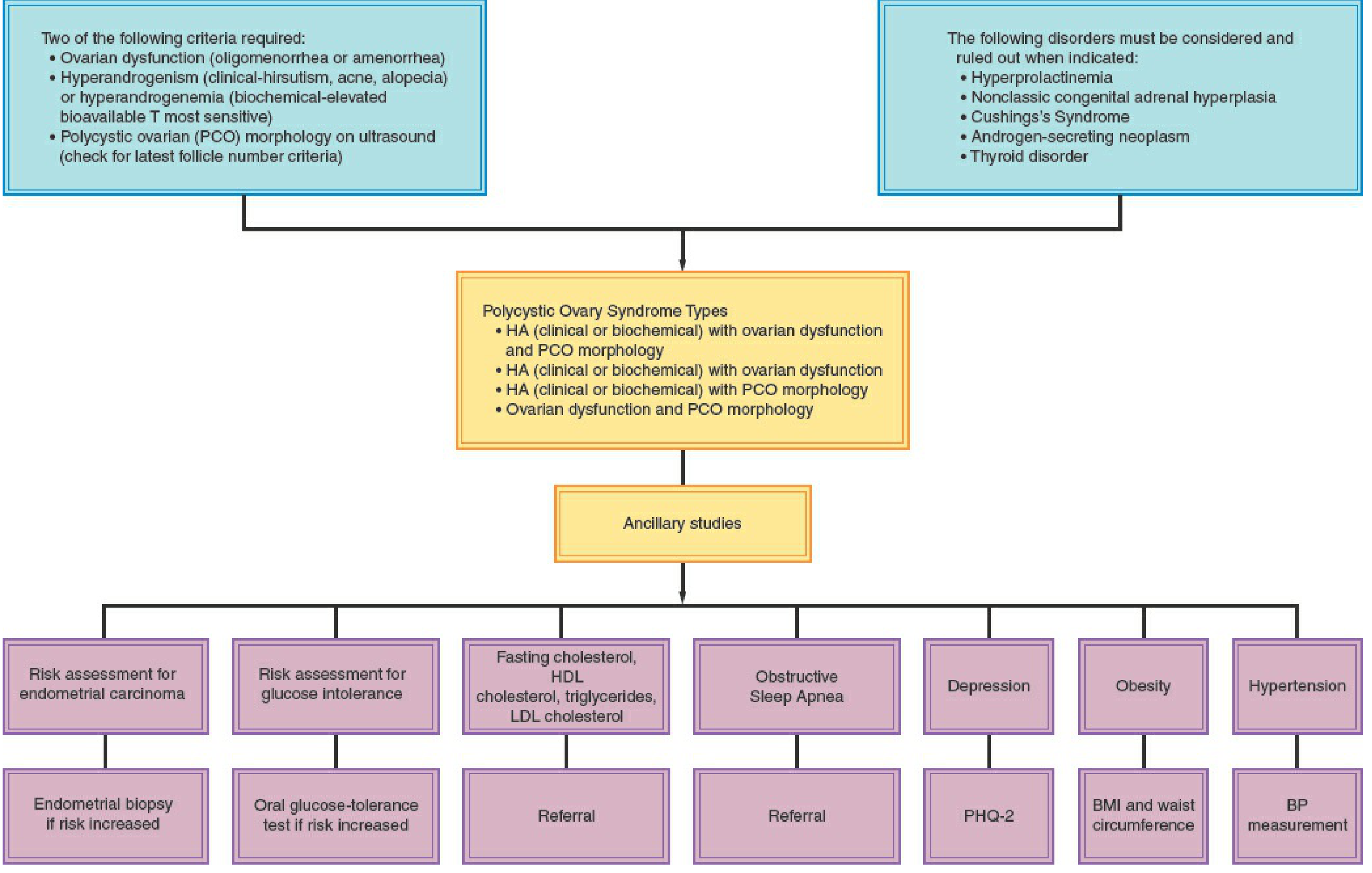
Diagnostic Criteria (Rotterdam 2003 - 2 of 3 required)
| Criterion | Description |
|---|---|
| 1. Menstrual dysfunction | Oligomenorrhea or amenorrhea |
| 2. Hyperandrogenism (HA) | Clinical (hirsutism, acne, alopecia) or biochemical (elevated androgens) |
| 3. Polycystic ovary (PCO) morphology | Ultrasound: ≥20 follicles (2-9 mm) in either ovary and/or ovarian volume >10 mL |
Diagnosis of exclusion - other causes must be ruled out first.
Signs and Symptoms by Category
1. Menstrual Irregularities
- Oligomenorrhea - infrequent periods (cycles >35 days)
- Amenorrhea - absent periods (primary or secondary)
- Irregular/unpredictable menstrual cycles
- Anovulation/oligo-ovulation - some women may have regular cycles but still not ovulate (21% of hyperandrogenic women with regular cycles are anovulatory)
- Onset typically at menarche - abnormal menses from puberty is the classic pattern
2. Hyperandrogenic Signs (Clinical)
- Hirsutism - excess body/facial hair in male distribution; occurs in ~70% of PCOS patients in the US (only 10-20% in Asian populations due to differences in 5α-reductase activity)
- Acne - especially persistent adult acne
- Male-pattern alopecia - diffuse scalp hair thinning, especially at crown
- Clitoromegaly (rare, more with virilization)
3. Metabolic Features
- Obesity - present in >50% of PCOS patients; characteristically central/android distribution (abdominal fat deposition, higher waist-to-hip ratio)
- Insulin resistance (IR) - very common; leads to hyperinsulinemia, which worsens androgen production
- Impaired glucose tolerance / Type 2 diabetes - significantly increased risk
- Dyslipidemia - elevated total cholesterol, triglycerides, LDL; low HDL (the most characteristic alteration is decreased HDL2α)
- Acanthosis nigricans - velvety, dark skin patches (neck, axilla, groin) - marker of insulin resistance
4. Reproductive / Fertility Consequences
- Anovulatory infertility - PCOS is the most common cause of anovulatory infertility in developed countries
- Recurrent early miscarriage - increased risk
- Pregnancy complications - gestational diabetes, gestational hypertension, preeclampsia, preterm birth
5. Cardiovascular & Long-term Risks
- Hypertension - incidence increases with age, reaching 40% by perimenopause
- Increased atherosclerosis risk
- ~7-fold increased risk of myocardial infarction
- Obstructive sleep apnea - underrecognized association
- Impaired fibrinolysis - elevated plasminogen activator inhibitor (PAI) levels
6. Psychological Features
- Depression
- Anxiety
- Body image concerns
7. Pelvic / Sonographic Findings
- Enlarged ovaries - 2-5x normal size on ultrasound
- String of pearls / necklace sign - multiple small follicles arranged peripherally
- Increased ovarian stroma
- Thickened ovarian cortex on gross pathology (white, fibrotic)
PCOS Diagnostic Algorithm
Key Laboratory Findings
| Finding | Direction |
|---|---|
| LH : FSH ratio | Elevated (classically >2:1 or >3:1) |
| Total & free testosterone | Elevated (usually ≤2x upper normal) |
| Androstenedione | Elevated |
| DHEA-S | May be elevated (adrenal contribution) |
| Fasting insulin | Elevated |
| Fasting glucose / OGTT | Abnormal (screen for T2DM) |
| LH | Elevated in ~2/3 of cases |
| HDL cholesterol | Low |
| Triglycerides | Elevated |
| AMH (Anti-Mullerian Hormone) | Elevated - useful marker |
Four PCOS Phenotypes (Rotterdam)
- HA + Ovarian dysfunction + PCO morphology (classic, most severe)
- HA + Ovarian dysfunction (without PCO morphology)
- HA + PCO morphology (with regular cycles)
- Ovarian dysfunction + PCO morphology (without HA)
Conditions to Rule Out
Before diagnosing PCOS, exclude:
- Hyperprolactinemia
- Non-classic congenital adrenal hyperplasia (measure basal follicular-phase 17-OHP)
- Cushing's syndrome
- Androgen-secreting neoplasm (ovarian or adrenal)
- Thyroid disease (hypo/hyperthyroidism)
- Hypergonadotropic or hypogonadotropic disorders
Sources: Berek & Novak's Gynecology, p. 1919-1923 | Goldman-Cecil Medicine, p. 2551 | Harrison's Principles of Internal Medicine 22E, p. 3179 | Fitzpatrick's Dermatology | Swanson's Family Medicine Review
Lipoma detail explanation
Reading File
Finding Sources
Searching PubMed
"lipoma" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, multi-source information. Here is the full detailed explanation:
Lipoma - Detailed Explanation
Definition
A lipoma is a benign tumor composed of mature white adipocytes (fat cells). It is the most common soft tissue tumor in adults and the most common benign mesenchymal neoplasm overall. Most are cured by simple excision.
Epidemiology
- Affects adults predominantly, with peak incidence in the 5th to 7th decades of life
- No sex predilection (affects males and females equally)
- Multiple lipomas are uncommon; solitary lesions are the rule
- Rare in children
- Prevalence: affects approximately 1% of the general population
Classification / Types
| Type | Features |
|---|---|
| Conventional / Subcutaneous | Most common; small (<5 cm), encapsulated, painless |
| Intramuscular | Larger, ill-defined, infiltrative; higher recurrence (~20%) |
| Intermuscular | Between muscle groups; usually painless |
| Parosteal | Arises on bone surface; may stimulate periosteal reaction |
| Angiolipoma | Contains blood vessels with fibrin thrombi; often painful, often multiple |
| Fibrolipoma | Abundant fibrous tissue within lesion |
| Chondrolipoma | Contains cartilage |
| Osteolipoma | Contains bone (post-trauma or ischemia) |
| Myolipoma | Contains smooth muscle |
| Myxolipoma | Extensive myxoid change |
| Adenolipoma | Contains sweat ducts/glands (purely dermal) |
| Lipoma arborescens | Villous lipomatous proliferation of synovial membrane |
Etiology & Pathogenesis
Lipomas are cytogenetically heterogeneous. Key genetic abnormalities include:
- 12q13-15 aberrations - includes the HMGA2 gene (at 12q14.3), which plays a key role in pathogenesis; various HMGA2 fusion genes have been reported
- 6p21-23 rearrangements
- 13q deletions
These genetic changes result in aberrant adipocyte differentiation and uncontrolled proliferation of mature fat cells.
Clinical Features
Common Presentation
- Painless, slowly growing subcutaneous mass
- Soft, fluctuant, compressible on palpation
- Mobile - slides under the fingers ("slipping sign")
- Well-defined margins
- Doughy or rubbery consistency
- Overlying skin is normal in color and texture
Typical Locations
- Trunk (back, shoulders)
- Neck
- Proximal extremities (upper arms, thighs)
- Less common: hands, feet (thenar eminence in the hand)
- Involvement of hands and feet is uncommon
Size
- Superficial (subcutaneous): usually <5 cm
- Deep-seated (intramuscular/intermuscular): can be considerably larger
When Lipomas Are Painful
Pain is not typical but occurs when:
- Nerve compression in restricted spaces (carpal tunnel, tarsal tunnel, cubital tunnel)
- Angiolipoma subtype (painful by nature)
- Very large lesions compressing adjacent structures
Histopathology
Gross appearance:
- Yellow, lobulated, soft fatty tissue
- Well-circumscribed with a thin fibrous capsule
- Multiple white/yellow lobules separated by fine septa
Microscopy:
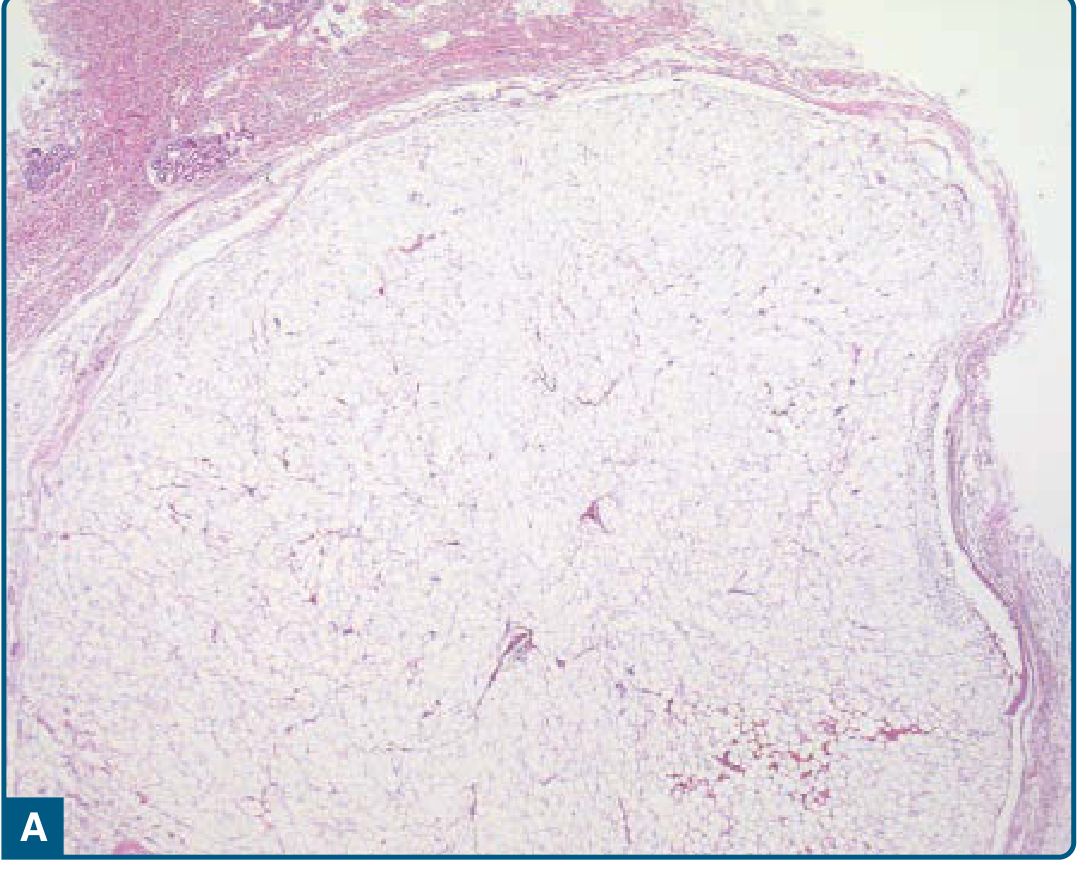
- Composed of mature adipocytes with only slight variation in size/shape
- No nuclear atypia
- Thin, hypocellular fibrous septa containing thin-walled capillaries
- Lobulated architecture
- Immunohistochemistry: Tumor cells are negative for p16, MDM2, and CDK4 (important to distinguish from atypical lipomatous tumor/liposarcoma)
- May show posttraumatic changes: fat necrosis, inflammation, histiocytes
Syndromes Associated with Multiple Lipomas
| Syndrome | Associated Features |
|---|---|
| Gardner syndrome | Familial adenomatous polyposis, desmoid fibromatosis, osteomas, cysts |
| Bannayan-Riley-Ruvalcaba syndrome | Macrocephaly, lymphangiomas, hamartomas, intestinal polyposis, lentigines |
| Cowden syndrome | Hamartomas, trichilemmomas, oral papillomas, palmoplantar keratoses |
| Goldenhar-Gorlin syndrome | Intracranial lipomas, hydrocephalus, oculoauriculovertebral dysplasia |
| Madelung disease (Symmetric lipomatosis) | Neck/shoulder/upper limb lipomas; middle-aged Mediterranean men; peripheral neuropathy |
| MERRF syndrome | Symmetric lipomas, myoclonus epilepsy, ragged-red fibers |
| CLOVE syndrome | Congenital lipomatous overgrowth, vascular malformations, epidermal nevi |
Imaging
X-Ray
- Large lipomas appear as areas of relative radiolucency compared to surrounding soft tissue
- Small lesions invisible on X-ray
- Foci of calcification or ossification visible in ~11% of cases
Ultrasound
- Elliptical, often well-defined mass
- Long axis and internal septations oriented parallel to skin surface
- Variable reflectivity (often more reflective than surrounding fat)
- Compressible on light probe pressure
- May or may not appear encapsulated
CT Scan
- Mass of density similar to subcutaneous fat (negative Hounsfield units, approximately -65 to -120 HU)
- Rarely needed for superficial lesions
- More useful for deep/retroperitoneal lesions
MRI (Gold Standard for Deep Lesions)
- Isointense to subcutaneous fat on both T1 and T2 weighted images
- Low signal on STIR (fat suppression sequences null the signal)
- Signal suppressed on T2 fat-saturation sequences
- Fine thin septa (<2 mm) may be visible - this distinguishes lipoma from atypical lipomatous tumor (which has thick or nodular enhancing septa)
- Fine septa show little or no gadolinium enhancement
Differential Diagnosis
| Lesion | Distinguishing Features |
|---|---|
| Liposarcoma (well-differentiated/atypical lipomatous tumor) | Thick/nodular enhancing septa on MRI; MDM2/CDK4 positive on IHC; atypical cells and lipoblasts on histology |
| Angiolipoma | Painful, often multiple; increased vasculature with fibrin thrombi on histology |
| Epidermoid/sebaceous cyst | Firmer, attached to skin, has a punctum |
| Lipodermoid | Subconjunctival location |
| Hibernoma | Composed of brown fat; younger patients; more vascular on imaging |
| Nodular fasciitis | Young adults, upper extremities; not purely fat; MYH9-USP6 fusion |
| Fibroma / desmoid | Firm, fibrotic; no fat signal on MRI |
Treatment
Conservative (Observation)
- Asymptomatic small lipomas do not require treatment
- Monitoring is acceptable if the diagnosis is clinically certain
Surgical Excision (Definitive)
- Indications: symptomatic (pain, nerve compression), large, rapidly growing, cosmetically bothersome, or uncertain diagnosis
- Technique:
- Incise skin over the lesion
- Squeeze the surrounding tissue to make it bulge forward
- Blunt or sharp dissection along the cleavage plane (enucleation)
- For large/multilocular lesions: meticulous hemostasis, close dead space or insert suction drain
- Local or general anesthesia depending on size/location
- Cure rate: near 100% for conventional subcutaneous lipomas
- Recurrence: Rare for conventional lipomas; up to 20% for intramuscular lipomas
Liposuction
- Suitable for soft, subcutaneous lipomas in cosmetically sensitive areas
- Higher recurrence rate than open excision
Steroid Injection (Triamcinolone)
- Causes local fat atrophy; can reduce size of small lipomas
- Not curative, but useful in selected patients who decline surgery
Prognosis
- Classical subcutaneous lipomas: entirely benign, recur only rarely after excision
- Intramuscular lipomas: higher local recurrence rate (up to 20%)
- Malignant transformation (lipoma → liposarcoma): an exceedingly rare phenomenon
- No risk of metastasis
Key Distinguishing Points: Lipoma vs Liposarcoma
| Feature | Lipoma | Liposarcoma |
|---|---|---|
| Nature | Benign | Malignant |
| Size | Usually <5 cm (superficial) | Often large, deep |
| Location | Subcutaneous, superficial | Deep soft tissues, retroperitoneum |
| MRI septa | Thin (<2 mm), no enhancement | Thick, nodular, enhancing |
| IHC | p16-, MDM2-, CDK4- | MDM2+, CDK4+ (well-differentiated) |
| Recurrence | Rare (<2%) | Common |
| Metastasis | Never | Yes (except well-differentiated) |
Sources: Fitzpatrick's Dermatology, 9e, p. 2202-2203 | Robbins & Kumar Basic Pathology, p. 151 | Grainger & Allison's Diagnostic Radiology, p. 1707-1729 | Sabiston Textbook of Surgery | Pye's Surgical Handicraft, 22e | Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.