Superficial tendon reflex and deep tendon reflex
Superficial (Cutaneous) Tendon Reflexes vs. Deep Tendon Reflexes
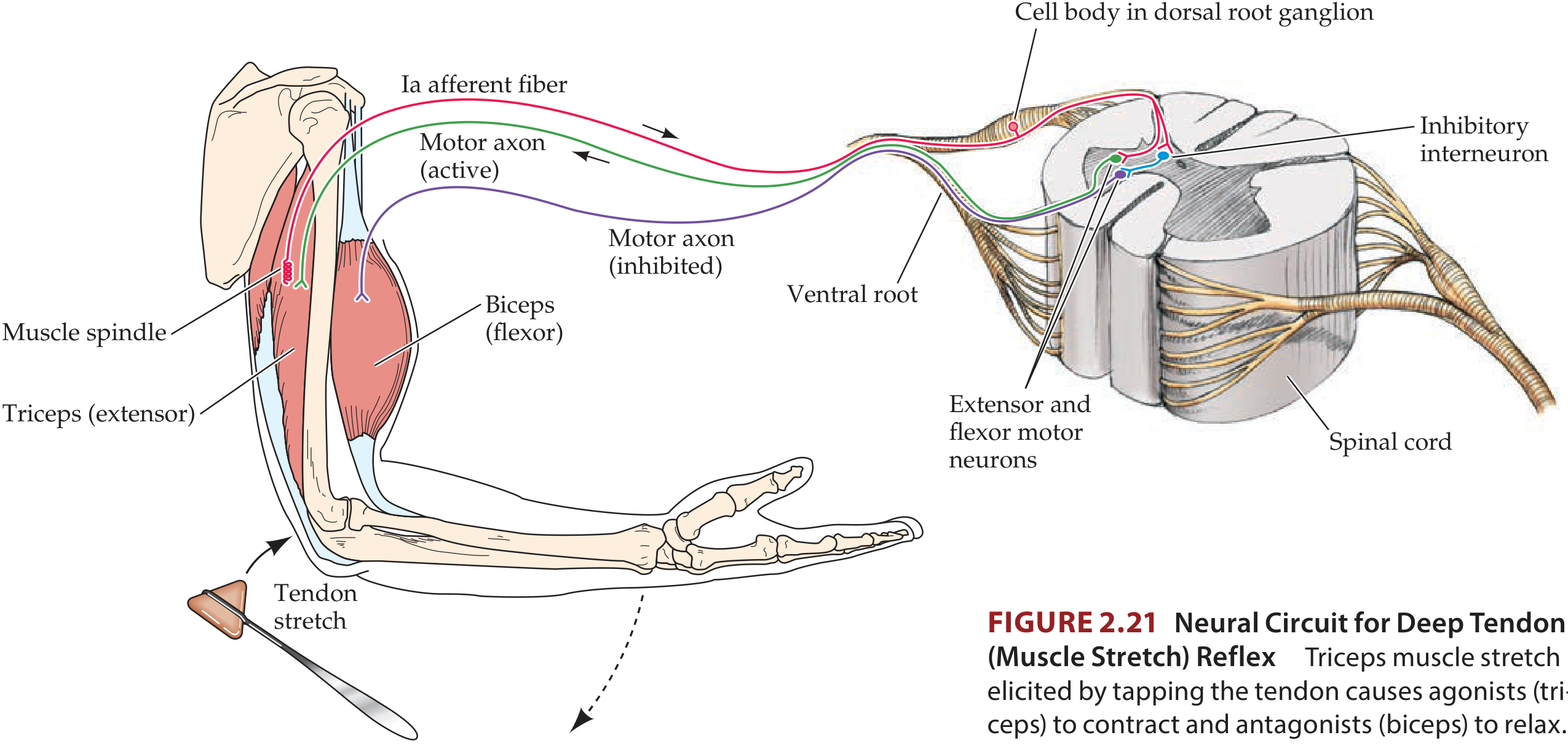
Deep Tendon Reflexes (DTRs) / Stretch Reflexes
Definition & Mechanism
Components of the Reflex Arc
- Receptor - Muscle spindle (detects stretch)
- Afferent limb - Group Ia (primary) and Group II (secondary) sensory fibers via dorsal root
- Integration center - Spinal cord gray matter (anterior horn)
- Efferent limb - Alpha motor neuron via ventral root
- Effector - Extrafusal skeletal muscle fibers (contraction)
Dynamic vs. Static Components
- Dynamic stretch reflex: Brief, powerful contraction in response to sudden stretch - elicited by the velocity component from primary (Ia) endings. Over within a fraction of a second.
- Static stretch reflex: Weaker but prolonged contraction proportional to maintained muscle length, elicited by both primary and secondary endings. Functions to maintain muscle length against gravity. - Guyton & Hall, p.679
Modulation by Higher Centers
Common DTRs and Their Spinal Levels
| Reflex | Tendon Tapped | Spinal Level | Response |
|---|---|---|---|
| Biceps jerk | Biceps tendon | C5, C6 | Elbow flexion |
| Triceps jerk | Above olecranon | C7 | Elbow extension |
| Knee jerk (patellar) | Ligamentum patellae | L2, L3, L4 | Leg extension |
| Ankle jerk | Tendo Achilles (dorsiflexed foot) | S1, S2 | Plantar flexion |
Clonus
Golgi Tendon Reflex (inverse myotatic reflex)
Superficial (Cutaneous) Reflexes
Definition & Mechanism
Key Superficial Reflexes and Spinal Levels
| Reflex | How Elicited | Normal Response | Spinal Level |
|---|---|---|---|
| Plantar reflex | Scratch inner/outer border of sole with a pin | Flexion (curling) of great toe | S1 |
| Abdominal reflexes | Stroke abdominal wall parallel to costal margins/iliac crests | Umbilicus moves toward the stroked side | T7-T11 |
| Cremasteric reflex | Scratch skin at upper inner thigh | Testis drawn upward (cremaster contracts) | T12 / L1-L2 |
The Plantar Reflex and Babinski's Sign
- Normal response: Great toe flexes (plantar flexion)
- Babinski's sign (abnormal): Great toe extends (dorsiflexes) with fanning of other toes - indicates pyramidal tract (UMN) lesion. Also physiologically normal in infants whose tracts are not yet myelinated. - S Das, p.279
Abdominal Reflexes
Key Clinical Differences: UMN vs. LMN Lesions
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Deep tendon reflexes | Exaggerated (hyperreflexia) | Diminished/absent (hyporeflexia) |
| Superficial reflexes | Diminished/absent | Variable |
| Plantar reflex | Extensor (Babinski +) | Normal flexor |
| Clonus | May be present | Absent |
| Tone | Spastic (increased) | Flaccid (decreased) |
| Fasciculations | Absent | Present |
"In lesions of the pyramidal system, all deep or tendon reflexes are exaggerated, sometimes so much that a clonus can be elicited; the superficial or skin reflexes are diminished or absent (e.g. abdominal reflexes) or altered as in plantar reflex (Babinski's sign)." - S Das, A Manual on Clinical Surgery, 13th Ed.
Why Testing Both Matters
- Sensory neurons (Ia afferent integrity)
- LMN/anterior horn cells
- Descending UMN modulatory pathways
Create a clinical summary table comparing UMN vs LMN findings
UMN vs. LMN: Clinical Summary Table
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness pattern | Groups of muscles; never individual muscles | Individual muscles may be affected |
| Muscle tone | Increased - spasticity (acute phase: may be decreased) | Decreased - flaccidity |
| Deep tendon reflexes | Increased (hyperreflexia) - clonus possible (acute phase: may be decreased) | Decreased/absent (hyporeflexia/areflexia) |
| Superficial (cutaneous) reflexes | Diminished or absent (e.g. abdominal reflexes) | Variable - usually preserved if arc is intact |
| Plantar reflex | Extensor - upgoing (Babinski sign) (expected normally in infants up to 1-2 years) | Flexor - downgoing (normal response) |
| Muscle atrophy | Absent (mild disuse atrophy only, up to ~30%) | Pronounced - up to 70% of total bulk |
| Fasciculations | Absent | Present (spontaneous motor unit firing) |
| Clonus | May be present (ankle, patellar) | Absent |
| Hoffmann's sign | May be present | Absent |
| Additional pathological reflexes | Babinski, Hoffmann, posturing present | Absent |
| Nerve conduction studies | Normal | Abnormal (reduced conduction velocity/amplitude) |
| EMG | No denervation potentials | Fibrillations, positive sharp waves, fasciculation potentials |
| Gait | Spastic gait (scissor/circumduction) | Steppage gait (foot drop), waddling gait |
| Affected level | Cerebral cortex, internal capsule, brainstem, corticospinal tract (before anterior horn) | Anterior horn cells, nerve roots, peripheral nerve, NMJ, muscle |
| Common causes | Stroke, MS, spinal cord compression, brain tumors, cerebral palsy | Polio, GBS, peripheral neuropathy, motor neuron disease (anterior horn), radiculopathy |
Important Caveats
Anatomical Localization Aid
CEREBRAL CORTEX / INTERNAL CAPSULE
↓ (corticospinal tract)
BRAINSTEM
↓
SPINAL CORD (before anterior horn) ← UMN lesions above this
↓
ANTERIOR HORN CELLS ← LMN lesions start here
↓
NERVE ROOT / PERIPHERAL NERVE
↓
NEUROMUSCULAR JUNCTION
↓
MUSCLE
Give me a detailed description of tracts of spinal cord including ascending descending pyramidal and extrapyramidal tract
Spinal Cord Tracts - Detailed Description
OVERVIEW
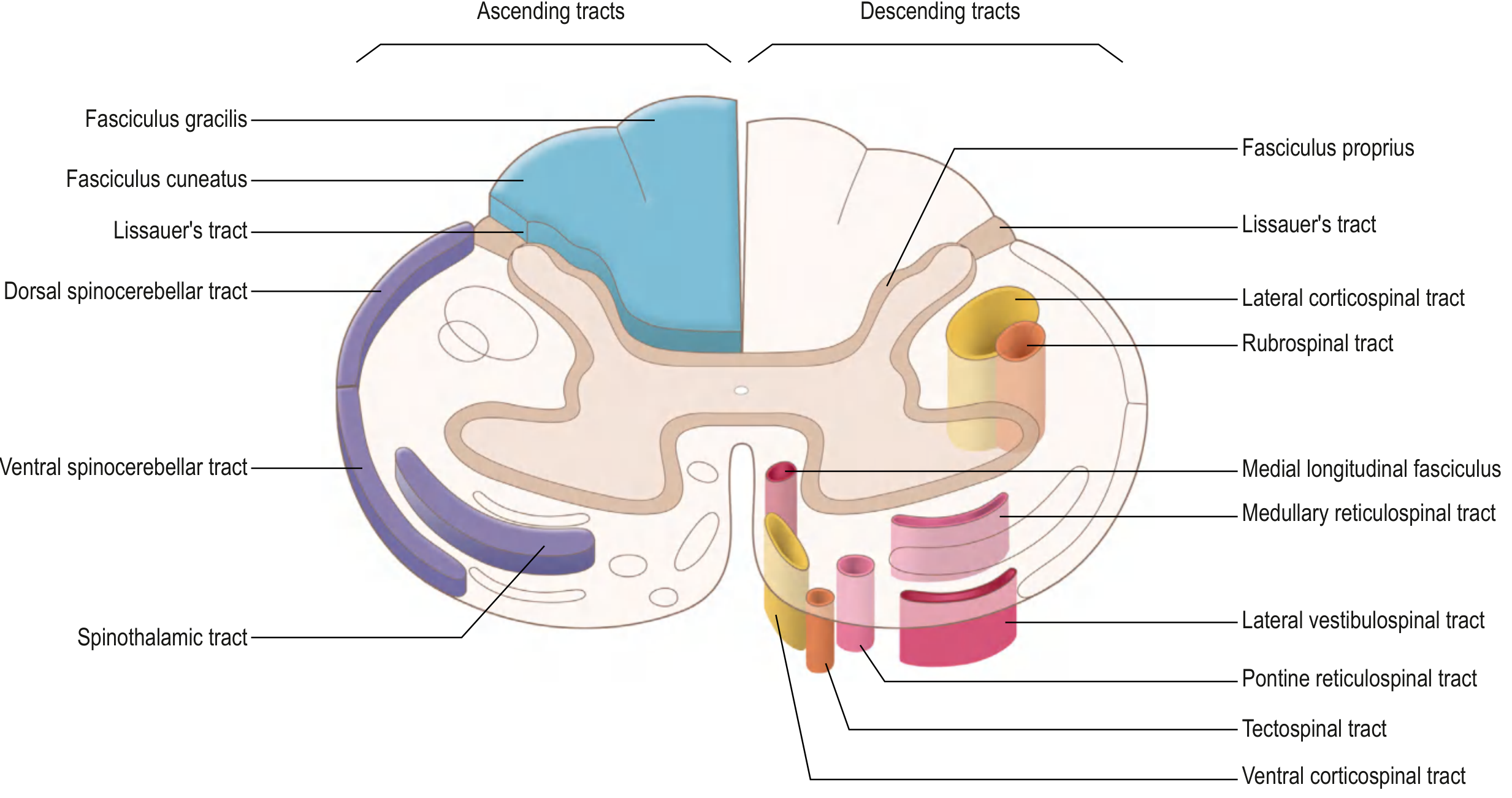
- Posterior (dorsal) funiculus - mainly ascending sensory tracts
- Lateral funiculus - both ascending and descending tracts
- Anterior (ventral) funiculus - mainly descending motor tracts
ASCENDING TRACTS (Sensory)
1. Posterior Column - Medial Lemniscal Pathway
- Fasciculus Gracilis (medial): carries input from lower limb and lower trunk (below T6). Fibers from S, L, lower T segments.
- Fasciculus Cuneatus (lateral): carries input from upper limb, upper trunk, and neck (above T6). Fibers from upper T, C segments.
- 1st order neuron: Cell body in dorsal root ganglion → enters posterior horn → ascends ipsilaterally in posterior column → synapses in nucleus gracilis / nucleus cuneatus in the caudal medulla
- 2nd order neuron: Axons cross as internal arcuate fibers → form the medial lemniscus (contralateral medulla) → ascend to VPL nucleus of thalamus
- 3rd order neuron: VPL thalamus → through posterior limb of internal capsule → primary somatosensory cortex (postcentral gyrus)
2. Anterolateral System (Spinothalamic Tract)
a) Spinothalamic Tract (main)
- 1st order neuron: Cell body in dorsal root ganglion → enters posterior horn → ascends/descends 1-2 segments in Lissauer's tract → synapses in laminae I and V of posterior horn
- 2nd order neuron: Axon crosses obliquely over 2-3 spinal segments through the anterior white commissure → joins the contralateral anterolateral column → ascends to VPL nucleus of thalamus
- 3rd order neuron: VPL thalamus → posterior limb of internal capsule → primary somatosensory cortex
b) Spinoreticular Tract
- Carries the emotional/affective components of pain
- 2nd order axons project to the reticular formation in the brainstem (not the thalamus)
c) Spinomesencephalic Tract
- Projects to periaqueductal gray (PAG) and superior colliculi
- Involved in central pain modulation (endogenous analgesia)
3. Spinocerebellar Tracts (Subconscious Proprioception)
| Tract | Origin | Decussation | Location | Carries |
|---|---|---|---|---|
| Dorsal spinocerebellar | Clarke's nucleus (T1-L2) | None - ipsilateral | Lateral funiculus (posterior) | Unconscious proprioception from trunk and ipsilateral lower limb |
| Ventral spinocerebellar | Spinal border cells (lumbosacral) | Crosses twice (net ipsilateral) | Lateral funiculus (anterior) | Proprioception from lower limb |
| Cuneocerebellar | External arcuate nucleus (medulla) | None - ipsilateral | - | Proprioception from upper limb (above T6) |
DESCENDING TRACTS (Motor)
PYRAMIDAL TRACT (Corticospinal Tract)
Origin
- ~30% from primary motor cortex (precentral gyrus, area 4)
- ~30% from premotor and supplementary motor areas (area 6)
- ~40% from somatosensory cortex (parietal lobe, areas 1, 2, 3)
Course
Primary Motor Cortex (precentral gyrus)
↓
Corona Radiata
↓
Posterior limb of Internal Capsule
(between caudate nucleus and putamen)
↓
Crus Cerebri (midbrain)
↓
Anterior Pons (small scattered bundles)
↓
Medullary Pyramids (forms the "pyramid" bulge)
↓
Pyramidal Decussation (cervicomedullary junction)
↙ (85-90% cross) ↘ (10-15% stay)
Lateral Corticospinal Anterior Corticospinal
Tract (contralateral Tract (ipsilateral
lateral funiculus) anterior funiculus)
↓ ↓
Interneurons and LMNs Crosses later in
(lateral anterior horn) cervical/upper thoracic cord
↓ (controls bilateral axial muscles)
Skeletal muscle
(distal limb movements)
Key Features
- Controls fine, discrete, distal limb movements (especially fingers and hands)
- Terminates on interneurons of intermediate zones AND directly on anterior horn LMNs
- Has somatotopic organization throughout its course (leg medial, arm lateral in the cord)
- Damage → UMN signs (spasticity, hyperreflexia, Babinski sign)
EXTRAPYRAMIDAL TRACTS
LATERAL MOTOR SYSTEM
1. Rubrospinal Tract
| Feature | Detail |
|---|---|
| Origin | Red nucleus (magnocellular division), midbrain tegmentum |
| Decussation | Ventral tegmental decussation - immediately crosses in midbrain |
| Location in cord | Lateral funiculus (just anterior to lateral corticospinal tract) |
| Termination | Cervical cord only (in humans) - interneurons of anterior horn |
| Function | Controls movement of contralateral upper limbs; facilitates flexors, inhibits extensors |
MEDIAL MOTOR SYSTEM
2. Anterior Corticospinal Tract
| Feature | Detail |
|---|---|
| Origin | Primary motor cortex (uncrossed fibers from pyramidal decussation) |
| Location | Anterior funiculus, near anterior median fissure |
| Termination | Upper thoracic levels; crosses within the cord to synapse bilaterally |
| Function | Bilateral control of axial (postural) muscles |
3. Vestibulospinal Tract
| Feature | Detail |
|---|---|
| Origin (medial) | Medial vestibular nucleus → projects bilaterally to thoracic levels |
| Origin (lateral) | Lateral vestibular nucleus → descends ipsilaterally down entire cord |
| Location | Anterior funiculus |
| Input | Receives from inner ear (vestibular organ) and cerebellum |
| Function | Facilitates extensor/antigravity muscles, inhibits flexors - essential for maintaining balance and upright posture; mediates righting reflexes |
4. Reticulospinal Tracts
| Feature | Detail |
|---|---|
| Pontine reticulospinal | From pontine reticular formation → descends ipsilaterally → facilitates extensors |
| Medullary reticulospinal | From medullary reticular formation → descends bilaterally → inhibits extensors |
| Location | Anterior and lateral funiculi |
| Function | Regulates voluntary movement, reflex activity, muscle tone, and autonomic outflow |
5. Tectospinal Tract
| Feature | Detail |
|---|---|
| Origin | Superior colliculus (dorsal midbrain) |
| Decussation | Dorsal tegmental decussation |
| Location | Anterior funiculus, near median fissure |
| Termination | Cervical cord only |
| Function | Reflex postural movements of head and neck in response to visual stimuli |
Summary Comparison Table
| Tract | Type | Column | Origin | Decussation | Modality/Function |
|---|---|---|---|---|---|
| Fasciculus gracilis | Ascending | Posterior | DRG (below T6) | Medulla | Fine touch, vibration, proprioception (lower limb) |
| Fasciculus cuneatus | Ascending | Posterior | DRG (above T6) | Medulla | Fine touch, vibration, proprioception (upper limb) |
| Spinothalamic | Ascending | Anterolateral | Posterior horn | Spinal cord (anterior commissure) | Pain, temperature, crude touch |
| Dorsal spinocerebellar | Ascending | Lateral (post.) | Clarke's nucleus | None (ipsilateral) | Unconscious proprioception (lower limb) |
| Ventral spinocerebellar | Ascending | Lateral (ant.) | Spinal border cells | Twice (net ipsilateral) | Unconscious proprioception (lower limb) |
| Lateral corticospinal | Descending (Pyramidal) | Lateral | Motor cortex | Pyramidal decussation (medulla) | Voluntary fine movement (contralateral distal limbs) |
| Anterior corticospinal | Descending (Pyramidal) | Anterior | Motor cortex | Within cord (bilateral) | Axial/postural movements |
| Rubrospinal | Descending (Extrapyramidal) | Lateral | Red nucleus | Midbrain (ventral tegmental) | Flexor facilitation, distal limb control |
| Vestibulospinal | Descending (Extrapyramidal) | Anterior | Vestibular nuclei | None (ipsilateral) | Extensor facilitation, balance |
| Reticulospinal | Descending (Extrapyramidal) | Anterior/Lateral | Pontine/medullary RF | Ipsilateral | Tone, autonomic, voluntary movement modulation |
| Tectospinal | Descending (Extrapyramidal) | Anterior | Superior colliculus | Midbrain (dorsal tegmental) | Head/neck reflexes to visual stimuli |
Clinical Correlations
| Lesion | Tracts Affected | Clinical Picture |
|---|---|---|
| Brown-Séquard syndrome (hemisection) | Ipsilateral: posterior column + lateral CST; Contralateral: spinothalamic | Ipsilateral: fine touch/proprioception loss + UMN signs; Contralateral: pain/temperature loss |
| Central cord syndrome (syringomyelia) | Crossing spinothalamic fibers at affected levels | "Cape-like" suspended loss of pain and temperature; spares posterior column |
| Posterior column lesion (tabes dorsalis, B12 deficiency) | Fasciculus gracilis/cuneatus | Loss of vibration, proprioception; sensory ataxia, positive Romberg |
| Anterior cord syndrome | Bilateral spinothalamic + anterior CST | Loss of pain/temperature + motor paralysis below lesion; posterior column spared |
| ALS | Lateral CST + anterior horn cells | Combined UMN + LMN signs |
Generate a study guide on spinal cord tracts (DOCX or PDF)
ls /home/daytona/workspace/ 2>/dev/null && ls /home/daytona/skills/docx/scripts/…
mkdir -p /home/daytona/workspace/spinal-cord-study-guide && node -e "require('do…
~/spinal-cord-study-guide/generate.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageNumber, Header, Footer, TabStopType, TabStopPosition,
PageBreak, UnderlineType
} = require('docx');
const fs = require('fs');
// ── Colour palette ──────────────────────────────────────────────────────────
const BLUE_DARK = "1A3A5C"; // headings
const BLUE_MID = "2E6DA4"; // sub-headings / accent
const BLUE_LIGHT = "D9E8F5"; // table header shading
const GREEN_DARK = "1B5E20"; // ascending tract headers
const GREEN_LIGHT= "E8F5E9"; // ascending shading
const RED_DARK = "B71C1C"; // descending tract headers
const RED_LIGHT = "FFEBEE"; // descending shading
const GREY_LIGHT = "F5F5F5"; // alternating table rows
const WHITE = "FFFFFF";
// ── Helper: bold coloured text run ─────────────────────────────────────────
const h = (text, color = BLUE_DARK, size = 24) =>
new TextRun({ text, bold: true, color, size });
const t = (text, opts = {}) =>
new TextRun({ text, size: opts.size || 20, color: opts.color || "000000",
bold: opts.bold || false, italics: opts.italics || false });
// ── Helper: heading paragraph ───────────────────────────────────────────────
function heading1(text) {
return new Paragraph({
heading: HeadingLevel.HEADING_1,
spacing: { before: 300, after: 120 },
children: [new TextRun({ text, bold: true, color: BLUE_DARK, size: 32, font: "Calibri" })]
});
}
function heading2(text, color = BLUE_MID) {
return new Paragraph({
heading: HeadingLevel.HEADING_2,
spacing: { before: 240, after: 80 },
children: [new TextRun({ text, bold: true, color, size: 26, font: "Calibri" })]
});
}
function heading3(text, color = "2C3E50") {
return new Paragraph({
heading: HeadingLevel.HEADING_3,
spacing: { before: 160, after: 60 },
children: [new TextRun({ text, bold: true, color, size: 22, font: "Calibri" })]
});
}
function para(text, opts = {}) {
return new Paragraph({
spacing: { before: 60, after: 60 },
alignment: opts.align || AlignmentType.LEFT,
children: [new TextRun({ text, size: opts.size || 20, color: opts.color || "000000",
bold: opts.bold || false, italics: opts.italics || false, font: "Calibri" })]
});
}
function bullet(text, level = 0) {
return new Paragraph({
bullet: { level },
spacing: { before: 40, after: 40 },
children: [new TextRun({ text, size: 20, font: "Calibri" })]
});
}
function spacer() {
return new Paragraph({ spacing: { before: 60, after: 60 }, children: [new TextRun({ text: "" })] });
}
function pageBreak() {
return new Paragraph({ children: [new PageBreak()] });
}
function note(text) {
return new Paragraph({
spacing: { before: 80, after: 80 },
indent: { left: 360 },
children: [
new TextRun({ text: "⚠ Clinical Note: ", bold: true, color: RED_DARK, size: 20, font: "Calibri" }),
new TextRun({ text, size: 20, italics: true, color: "4A4A4A", font: "Calibri" })
]
});
}
// ── Helper: shaded cell ─────────────────────────────────────────────────────
function cell(text, opts = {}) {
return new TableCell({
width: opts.width ? { size: opts.width, type: WidthType.PERCENTAGE } : undefined,
verticalAlign: VerticalAlign.CENTER,
shading: opts.shade ? { fill: opts.shade, type: ShadingType.SOLID } : undefined,
children: [new Paragraph({
alignment: AlignmentType.LEFT,
spacing: { before: 60, after: 60 },
children: [new TextRun({
text,
bold: opts.bold || false,
size: opts.size || 18,
color: opts.color || "000000",
font: "Calibri"
})]
})]
});
}
// ── Helper: table with header row ────────────────────────────────────────────
function makeTable(headers, rows, headerShade = BLUE_LIGHT) {
const headerRow = new TableRow({
tableHeader: true,
children: headers.map(h => cell(h, { bold: true, shade: headerShade, color: "1A3A5C", size: 19 }))
});
const dataRows = rows.map((row, ri) =>
new TableRow({
children: row.map(cellText => cell(cellText, { shade: ri % 2 === 0 ? WHITE : GREY_LIGHT }))
})
);
return new Table({
width: { size: 100, type: WidthType.PERCENTAGE },
borders: {
top: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
bottom: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
left: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
right: { style: BorderStyle.SINGLE, size: 4, color: BLUE_MID },
insideH:{ style: BorderStyle.SINGLE, size: 1, color: "CCCCCC" },
insideV:{ style: BorderStyle.SINGLE, size: 1, color: "CCCCCC" },
},
rows: [headerRow, ...dataRows]
});
}
// ═══════════════════════════════════════════════════════════════════════════
// DOCUMENT CONTENT
// ═══════════════════════════════════════════════════════════════════════════
const children = [
// ── TITLE PAGE ─────────────────────────────────────────────────────────
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 600, after: 200 },
children: [new TextRun({ text: "SPINAL CORD TRACTS", bold: true, size: 52, color: BLUE_DARK, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 120 },
children: [new TextRun({ text: "Comprehensive Study Guide", size: 32, color: BLUE_MID, font: "Calibri", italics: true })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 80 },
children: [new TextRun({ text: "Ascending • Descending • Pyramidal • Extrapyramidal", size: 24, color: "555555", font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 200, after: 0 },
children: [new TextRun({ text: "Sources: Gray's Anatomy for Students | Guyton & Hall Medical Physiology |", size: 18, color: "888888", font: "Calibri", italics: true })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 0, after: 0 },
children: [new TextRun({ text: "Neuroanatomy through Clinical Cases 3e | Adams & Victor's Principles of Neurology", size: 18, color: "888888", font: "Calibri", italics: true })]
}),
pageBreak(),
// ── SECTION 1: OVERVIEW ────────────────────────────────────────────────
heading1("1. Overview of Spinal Cord White Matter"),
para("The spinal cord white matter is divided into three funiculi (columns), each containing specific ascending and descending tracts:"),
spacer(),
makeTable(
["Funiculus (Column)", "Location", "Main Tracts"],
[
["Posterior (Dorsal)", "Between posterior horns", "Fasciculus gracilis, Fasciculus cuneatus"],
["Lateral", "Between anterior and posterior horns", "Lateral corticospinal, Rubrospinal, Spinothalamic, Spinocerebellar"],
["Anterior (Ventral)", "Between anterior horns", "Anterior corticospinal, Vestibulospinal, Reticulospinal, Tectospinal"],
]
),
spacer(),
para("General Rules:", { bold: true }),
bullet("Ascending tracts carry sensory information from periphery → brain"),
bullet("Descending tracts carry motor commands from brain → spinal cord"),
bullet("Most tracts decussate (cross midline) at some point — lesion side vs. symptom side depends on where"),
bullet("Sensory pathways use a 3-neuron chain: 1st order → 2nd order → 3rd order neuron"),
pageBreak(),
// ── SECTION 2: ASCENDING TRACTS ────────────────────────────────────────
heading1("2. Ascending (Sensory) Tracts"),
para("Sensory information travels via a 3-neuron relay: (1) Dorsal root ganglion → (2) Thalamus → (3) Somatosensory cortex."),
spacer(),
// 2A – Posterior Column
heading2("2A. Posterior Column – Medial Lemniscal Pathway", GREEN_DARK),
makeTable(
["Feature", "Details"],
[
["Location", "Posterior funiculus"],
["Modalities", "Fine/discriminative touch, vibration, 2-point discrimination, conscious proprioception, stereognosis"],
["Sub-divisions", "Fasciculus Gracilis (medial) — lower limb & trunk below T6\nFasciculus Cuneatus (lateral) — upper limb & trunk above T6"],
["1st Order Neuron", "Cell body in dorsal root ganglion → enters posterior horn → ascends IPSILATERALLY → nucleus gracilis / cuneatus (caudal medulla)"],
["2nd Order Neuron", "Crosses as internal arcuate fibers → forms medial lemniscus (contralateral) → ascends to VPL nucleus of thalamus"],
["3rd Order Neuron", "VPL thalamus → posterior limb of internal capsule → primary somatosensory cortex (postcentral gyrus, areas 1, 2, 3)"],
["Decussation Site", "Medulla (nucleus gracilis / cuneatus level)"],
["Lesion Effect", "IPSILATERAL loss of fine touch, vibration, proprioception BELOW the lesion level"],
],
GREEN_LIGHT
),
spacer(),
note("In posterior column lesions (e.g., tabes dorsalis, B12 deficiency, MS): sensory ataxia, positive Romberg's sign, loss of vibration and joint position sense."),
spacer(),
// 2B – Spinothalamic
heading2("2B. Anterolateral System — Spinothalamic Tract", GREEN_DARK),
makeTable(
["Feature", "Details"],
[
["Location", "Anterolateral column (lateral and anterior funiculi)"],
["Modalities", "Pain, temperature, crude touch, pressure"],
["1st Order Neuron", "DRG cell body → posterior horn → ascends/descends 1-2 segments in Lissauer's tract → synapses in laminae I and V"],
["2nd Order Neuron", "Crosses OBLIQUELY over 2-3 segments via anterior white commissure → joins contralateral anterolateral tract → VPL thalamus"],
["3rd Order Neuron", "VPL thalamus → posterior limb of internal capsule → primary somatosensory cortex"],
["Decussation Site", "Spinal cord (anterior white commissure) — 2-3 segments above entry level"],
["Lesion Effect", "CONTRALATERAL loss of pain and temperature, 1-2 levels below the lesion"],
],
GREEN_LIGHT
),
spacer(),
note("Central cord lesion (syringomyelia) destroys crossing fibers at affected levels → cape-like / suspended loss of pain and temperature bilaterally, sparing posterior column (dissociated sensory loss)."),
spacer(),
// 2B2 – Spinoreticular / spinomesencephalic
heading3("Spinoreticular and Spinomesencephalic Tracts"),
bullet("Spinoreticular tract: carries emotional/affective aspects of pain → reticular formation in brainstem (not thalamus)"),
bullet("Spinomesencephalic tract: projects to periaqueductal gray (PAG) → central pain modulation / endogenous analgesia"),
spacer(),
// 2C – Spinocerebellar
heading2("2C. Spinocerebellar Tracts (Subconscious Proprioception)", GREEN_DARK),
para("These tracts carry unconscious proprioceptive information from muscles, joints, and tendons to the cerebellum (NOT to conscious cortical awareness)."),
spacer(),
makeTable(
["Tract", "Origin", "Decussation", "Column", "Peduncle", "Function"],
[
["Dorsal (posterior) spinocerebellar", "Clarke's nucleus (T1–L2)", "None — ipsilateral", "Lateral (posterior)", "Inferior cerebellar", "Unconscious proprioception: trunk + ipsilateral lower limb"],
["Ventral (anterior) spinocerebellar", "Spinal border cells (lumbosacral)", "Crosses twice (net ipsilateral)", "Lateral (anterior)", "Superior cerebellar", "Proprioception from lower limb during locomotion"],
["Cuneocerebellar", "External arcuate nucleus (medulla)", "None — ipsilateral", "—", "Inferior cerebellar", "Proprioception from upper limb & neck (above T6)"],
],
GREEN_LIGHT
),
spacer(),
note("Spinocerebellar tract lesions (e.g., Friedreich's ataxia) produce cerebellar ataxia, nystagmus, dysarthria, and loss of coordination without loss of conscious proprioception."),
pageBreak(),
// ── SECTION 3: DESCENDING TRACTS ───────────────────────────────────────
heading1("3. Descending (Motor) Tracts"),
para("Divided into two major systems based on location and function:"),
bullet("Lateral motor system: controls distal limb movements (fine, skilled)"),
bullet("Medial motor system: controls axial/proximal muscles (posture, balance, automatic movement)"),
spacer(),
// 3A – Pyramidal
heading2("3A. PYRAMIDAL TRACT (Corticospinal Tract)", RED_DARK),
para("The direct voluntary motor pathway from cortex to spinal cord. The most clinically important descending tract."),
spacer(),
heading3("Origin"),
bullet("~30% from primary motor cortex (precentral gyrus, area 4) — including giant Betz cells"),
bullet("~30% from premotor and supplementary motor areas (area 6)"),
bullet("~40% from somatosensory cortex (areas 1, 2, 3)"),
bullet("Total fibers per tract: >1 million; Betz cell fibers: only ~34,000 (3%) — conduct at ~70 m/sec"),
spacer(),
heading3("Course"),
makeTable(
["Level", "Structure", "Notes"],
[
["Cortex", "Primary motor cortex", "Betz cells (60 μm), somatotopic map (homunculus)"],
["Cerebral hemisphere", "Corona radiata → posterior limb of internal capsule", "Leg (posterior), arm (middle), face (anterior) arrangement"],
["Midbrain", "Crus cerebri (basis pedunculi)", "Middle 3/5 of crus cerebri"],
["Pons", "Scattered bundles in basis pontis", "Separated by transverse pontocerebellar fibers"],
["Medulla", "Medullary pyramid", "Forms visible bulge = 'pyramid'"],
["Cervicomedullary junction", "Pyramidal decussation", "85-90% cross → Lateral corticospinal tract; 10-15% stay → Anterior corticospinal tract"],
["Spinal cord (lateral)", "Lateral corticospinal tract (lateral funiculus)", "Controls contralateral distal limbs — most important"],
["Spinal cord (anterior)", "Anterior corticospinal tract (anterior funiculus)", "Crosses later in cervical cord; controls bilateral axial muscles"],
["Termination", "Anterior horn interneurons (mainly) + some direct α-motor neurons", "Direct LMN synapses more prominent in humans than animals"],
],
RED_LIGHT
),
spacer(),
heading3("Somatotopic Organisation in the Lateral Corticospinal Tract"),
para("Leg fibers are most lateral (near cord surface); arm fibers are medial. This explains why central tumors/MS plaques may affect legs first."),
spacer(),
note("Damage to the pyramidal tract above the decussation → contralateral spastic hemiplegia (UMN signs: hyperreflexia, Babinski, spasticity). Damage below the decussation → ipsilateral UMN signs."),
spacer(),
// 3B – Extrapyramidal
heading2("3B. EXTRAPYRAMIDAL TRACTS", RED_DARK),
para("All descending motor tracts other than the corticospinal tract. They travel outside the medullary pyramids. They modulate posture, tone, balance, and automatic movements via indirect pathways through the basal ganglia, cerebellum, and brainstem nuclei."),
spacer(),
// Rubrospinal
heading3("i. Rubrospinal Tract [Lateral Motor System]"),
makeTable(
["Feature", "Details"],
[
["Origin", "Red nucleus — magnocellular division, midbrain tegmentum"],
["Decussation", "Ventral tegmental decussation — immediately crosses in midbrain"],
["Location in cord", "Lateral funiculus — just anterior to lateral corticospinal tract"],
["Termination", "Cervical cord only (in humans) — interneurons of lateral anterior horn"],
["Input", "Receives from motor cortex (corticorubral tract) and cerebellum"],
["Function", "Controls contralateral upper limb movement; facilitates flexors, inhibits extensors"],
["Clinical relevance", "Partially compensates when corticospinal tract is damaged (wrist/hand movement may persist)"],
],
RED_LIGHT
),
spacer(),
// Anterior corticospinal
heading3("ii. Anterior Corticospinal Tract [Medial Motor System]"),
makeTable(
["Feature", "Details"],
[
["Origin", "Motor cortex — uncrossed fibers from pyramidal decussation"],
["Location in cord", "Anterior funiculus, near anterior median fissure"],
["Decussation", "Crosses within cervical/upper thoracic cord"],
["Termination", "Upper thoracic levels — bilateral, medial anterior horn"],
["Function", "Bilateral control of axial/postural muscles"],
],
RED_LIGHT
),
spacer(),
// Vestibulospinal
heading3("iii. Vestibulospinal Tract [Medial Motor System]"),
makeTable(
["Feature", "Details"],
[
["Origin (medial)", "Medial vestibular nucleus → bilateral, to thoracic cord"],
["Origin (lateral)", "Lateral vestibular nucleus (Deiter's nucleus) → ipsilateral, entire cord"],
["Location in cord", "Anterior funiculus"],
["Input", "Inner ear (vestibular organ) + cerebellum"],
["Function", "FACILITATES extensors/antigravity muscles; INHIBITS flexors — maintains balance and upright posture; mediates righting reflexes"],
["Example", "Tripping → vestibulospinal reflex extends limbs to prevent fall"],
],
RED_LIGHT
),
spacer(),
// Reticulospinal
heading3("iv. Reticulospinal Tracts [Medial Motor System]"),
makeTable(
["Feature", "Pontine Reticulospinal", "Medullary Reticulospinal"],
[
["Origin", "Pontine reticular formation", "Medullary reticular formation"],
["Laterality", "Ipsilateral", "Bilateral"],
["Location", "Anterior funiculus", "Anterior/lateral funiculus"],
["Effect on extensors", "FACILITATES extensors", "INHIBITS extensors"],
["Function", "Muscle tone, voluntary movement, gait", "Modulates tone, autonomic outflow, reflexes"],
],
RED_LIGHT
),
spacer(),
note("Reticulospinal tracts are the final common pathway for basal ganglia and cerebellar influences on spinal motor neurons."),
spacer(),
// Tectospinal
heading3("v. Tectospinal Tract [Medial Motor System]"),
makeTable(
["Feature", "Details"],
[
["Origin", "Superior colliculus — dorsal midbrain"],
["Decussation", "Dorsal tegmental decussation — crosses in midbrain"],
["Location in cord", "Anterior funiculus, near anterior median fissure"],
["Termination", "Cervical cord only — interneurons in anterior horn"],
["Function", "Reflex postural movements of head and neck in response to VISUAL and auditory stimuli"],
],
RED_LIGHT
),
pageBreak(),
// ── SECTION 4: MASTER COMPARISON TABLE ─────────────────────────────────
heading1("4. Master Summary Table — All Spinal Cord Tracts"),
spacer(),
makeTable(
["Tract", "Type", "Column", "Origin", "Decussation", "Modality / Function"],
[
["Fasciculus gracilis", "Ascending", "Posterior", "DRG (below T6)", "Medulla", "Fine touch, vibration, proprioception (lower limb/trunk)"],
["Fasciculus cuneatus", "Ascending", "Posterior", "DRG (above T6)", "Medulla", "Fine touch, vibration, proprioception (upper limb/neck)"],
["Spinothalamic", "Ascending", "Anterolateral", "Posterior horn (I, V)", "Spinal cord (ant. commissure)", "Pain, temperature, crude touch"],
["Spinoreticular", "Ascending", "Anterolateral", "Posterior horn", "Spinal cord", "Emotional/affective pain component"],
["Spinomesencephalic", "Ascending", "Anterolateral", "Posterior horn", "Spinal cord", "Endogenous pain modulation (PAG)"],
["Dorsal spinocerebellar", "Ascending", "Lateral (post.)", "Clarke's nucleus (T1-L2)", "None (ipsilateral)", "Unconscious proprioception — lower limb"],
["Ventral spinocerebellar", "Ascending", "Lateral (ant.)", "Spinal border cells", "Twice (net ipsilateral)", "Unconscious proprioception — lower limb"],
["Lateral corticospinal", "Descending (Pyramidal)", "Lateral", "Motor cortex", "Pyramidal decussation (medulla)", "Voluntary fine movement — contralateral distal limbs"],
["Anterior corticospinal", "Descending (Pyramidal)", "Anterior", "Motor cortex", "Within cord (bilateral)", "Bilateral axial/postural movements"],
["Rubrospinal", "Descending (Extrapyramidal)", "Lateral", "Red nucleus (midbrain)", "Ventral tegmental decussation", "Flexor facilitation — contralateral upper limb"],
["Vestibulospinal (lateral)", "Descending (Extrapyramidal)", "Anterior", "Lateral vestibular nucleus", "None (ipsilateral)", "Extensor facilitation — balance, posture"],
["Reticulospinal (pontine)", "Descending (Extrapyramidal)", "Anterior", "Pontine RF", "Ipsilateral", "Facilitates extensors; modulates tone"],
["Reticulospinal (medullary)", "Descending (Extrapyramidal)", "Ant./Lateral", "Medullary RF", "Bilateral", "Inhibits extensors; autonomic outflow"],
["Tectospinal", "Descending (Extrapyramidal)", "Anterior", "Superior colliculus", "Dorsal tegmental decussation", "Head/neck reflexes to visual stimuli"],
]
),
pageBreak(),
// ── SECTION 5: CLINICAL SYNDROMES ──────────────────────────────────────
heading1("5. Clinical Cord Syndromes"),
spacer(),
makeTable(
["Syndrome", "Tracts Affected", "Ipsilateral Findings", "Contralateral Findings", "Cause"],
[
[
"Brown-Séquard\n(Cord Hemisection)",
"Posterior column + lateral CST (ipsilateral)\nSpingothalamic (contralateral)",
"Loss of fine touch, vibration, proprioception\nUMN motor weakness below lesion",
"Loss of pain and temperature (1-2 levels below lesion)",
"Stab wound, MS, tumor, radiation"
],
[
"Central Cord Syndrome\n(Syringomyelia)",
"Crossing spinothalamic fibers at affected levels",
"Cape-like loss of pain and temperature\nPosterior column intact (spared)",
"Same — bilateral symmetric loss",
"Syrinx, hyperextension injury, tumor"
],
[
"Anterior Cord Syndrome",
"Bilateral spinothalamic +\nanterior corticospinal tract",
"Motor paralysis + loss of pain/temp below lesion",
"Same — bilateral",
"Anterior spinal artery infarction, disc herniation"
],
[
"Posterior Column Syndrome\n(Dorsal Column Syndrome)",
"Fasciculus gracilis and/or cuneatus",
"Loss of vibration, proprioception, fine touch\nSensory ataxia, Romberg+",
"None (no contralateral deficit)",
"Tabes dorsalis, B12 deficiency, MS, Friedreich's ataxia"
],
[
"Complete Cord Transection",
"All tracts",
"Spinal shock initially → then spastic paraplegia/quadriplegia",
"Bilateral total loss below lesion",
"Trauma, tumour"
],
[
"Subacute Combined\nDegeneration (B12 def.)",
"Posterior columns + lateral\ncorticospinal tracts",
"Sensory ataxia + UMN signs (combined)",
"Bilateral involvement",
"B12 deficiency (pernicious anaemia)"
],
]
),
pageBreak(),
// ── SECTION 6: UMN vs LMN ──────────────────────────────────────────────
heading1("6. UMN vs LMN — Quick Reference"),
spacer(),
makeTable(
["Feature", "UMN Lesion", "LMN Lesion"],
[
["Weakness pattern", "Groups of muscles", "Individual muscles possible"],
["Muscle tone", "Increased (spasticity)\n[Acute: may be decreased]", "Decreased (flaccidity)"],
["Deep tendon reflexes", "Increased (hyperreflexia)\nClonus possible", "Decreased / absent"],
["Superficial reflexes", "Diminished or absent", "Variable"],
["Plantar reflex", "Extensor — Babinski sign", "Flexor (normal)"],
["Atrophy", "Mild (disuse only)", "Pronounced (up to 70%)"],
["Fasciculations", "Absent", "Present"],
["EMG", "No denervation potentials", "Fibrillations, positive sharp waves"],
["Level of lesion", "Cortex → anterior horn (exclusive)", "Anterior horn → muscle"],
]
),
spacer(),
note("Acute UMN lesion (spinal shock): initially flaccid with absent reflexes — spasticity develops over hours to months."),
pageBreak(),
// ── SECTION 7: MEMORY AIDS ─────────────────────────────────────────────
heading1("7. Memory Aids & Mnemonics"),
spacer(),
heading2("Decussation Sites"),
makeTable(
["Tract", "Where it Crosses", "Mnemonic Clue"],
[
["Posterior column (DCML)", "Medulla (nucleus gracilis/cuneatus)", "Crosses HIGH — medulla"],
["Spinothalamic", "Spinal cord (anterior commissure, 2-3 levels up)", "Crosses LOW — within cord"],
["Lateral corticospinal", "Pyramidal decussation (cervicomedullary)", "Crosses at the PYRAMID"],
["Rubrospinal", "Ventral tegmental decussation (midbrain)", "Crosses in MIDBRAIN"],
["Tectospinal", "Dorsal tegmental decussation (midbrain)", "Crosses in MIDBRAIN"],
]
),
spacer(),
heading2("Which Modalities Are Lost in Brown-Séquard?"),
para("SAME side as lesion: Motor (UMN) + fine touch + vibration + proprioception"),
para("OPPOSITE side to lesion: Pain + temperature (1-2 levels below)"),
para("Memory: IPSILATERAL motor and fine sensation; CONTRALATERAL pain and temperature"),
spacer(),
heading2("Posterior Column Sensory Modalities — PPVS"),
bullet("P — Proprioception (conscious joint position sense)"),
bullet("P — Pressure (deep)"),
bullet("V — Vibration"),
bullet("S — Stereognosis / fine discriminative touch"),
spacer(),
heading2("Spinocerebellar Tracts — DOVE"),
bullet("D — Dorsal spinocerebellar (from Clarke's nucleus, T1-L2, lower limb)"),
bullet("O — (goes up ipsilateral, no cross)"),
bullet("V — Ventral spinocerebellar (crosses twice — net ipsilateral)"),
bullet("E — Enters cerebellum via inferior and superior peduncles respectively"),
spacer(),
heading2("Lateral vs. Medial Motor Systems"),
para("LATERAL system (CST + rubrospinal) = LIMBS (distal, fine, skilled movement)"),
para("MEDIAL system (vestibulospinal + reticulospinal + tectospinal + anterior CST) = MIDDLE of body (axial, posture, balance)"),
pageBreak(),
// ── SECTION 8: QUICK-REVIEW Q&A ────────────────────────────────────────
heading1("8. Quick-Review Questions"),
spacer(),
makeTable(
["#", "Question", "Answer"],
[
["1", "Which tract carries conscious proprioception?", "Posterior column (fasciculus gracilis / cuneatus)"],
["2", "Where does the spinothalamic tract decussate?", "Within the spinal cord, 2-3 segments above entry, via anterior white commissure"],
["3", "What is the 3rd-order neuron relay station for all sensory tracts?", "VPL nucleus of the thalamus (for body); VPM for face"],
["4", "What percentage of CST fibers cross at the pyramidal decussation?", "~85-90% (form lateral CST); ~10-15% remain ipsilateral (anterior CST)"],
["5", "What cells of origin give the fastest conducting CST fibers?", "Betz cells (giant pyramidal neurons, ~60 μm, conduct at ~70 m/sec)"],
["6", "Which tract facilitates extensor muscles for balance?", "Vestibulospinal tract (especially lateral vestibulospinal)"],
["7", "What is the function of the spinomesencephalic tract?", "Central pain modulation via periaqueductal gray (PAG)"],
["8", "In Brown-Séquard: which side loses pain/temperature?", "Contralateral side (spinothalamic crosses in cord)"],
["9", "What lesion causes cape-like suspended sensory loss?", "Central cord (syringomyelia) — destroys crossing spinothalamic fibers"],
["10", "Clarke's nucleus is the origin of which tract?", "Dorsal spinocerebellar tract (T1-L2)"],
["11", "Which extrapyramidal tract descends only to cervical cord?", "Both rubrospinal and tectospinal tracts"],
["12", "What is the reticulospinal tract's role in autonomic function?", "Relays hypothalamic autonomic signals to preganglionic neurons in IML column"],
]
),
spacer(),
spacer(),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 200, after: 0 },
children: [new TextRun({ text: "— End of Study Guide —", italics: true, color: "888888", size: 20, font: "Calibri" })]
}),
new Paragraph({
alignment: AlignmentType.CENTER,
spacing: { before: 40, after: 0 },
children: [new TextRun({ text: "Generated by Orris AI | Sources: Gray's Anatomy for Students, Guyton & Hall, Neuroanatomy through Clinical Cases 3e, Adams & Victor 12e", italics: true, color: "AAAAAA", size: 16, font: "Calibri" })]
}),
];
// ═══════════════════════════════════════════════════════════════════════════
// BUILD DOCUMENT
// ═══════════════════════════════════════════════════════════════════════════
const doc = new Document({
creator: "Orris AI",
title: "Spinal Cord Tracts — Study Guide",
description: "Comprehensive study guide covering ascending, descending, pyramidal and extrapyramidal tracts of the spinal cord",
styles: {
default: {
document: {
run: { font: "Calibri", size: 20 }
}
}
},
sections: [{
properties: {
page: {
margin: { top: 1000, bottom: 1000, left: 1100, right: 1100 }
}
},
headers: {
default: new Header({
children: [new Paragraph({
alignment: AlignmentType.RIGHT,
children: [new TextRun({ text: "Spinal Cord Tracts — Study Guide", size: 16, color: "888888", font: "Calibri" })]
})]
})
},
footers: {
default: new Footer({
children: [new Paragraph({
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "Page ", size: 16, color: "888888", font: "Calibri" }),
new PageNumber({ type: "current", style: { size: 16, color: "888888", font: "Calibri" } }),
]
})]
})
},
children
}]
});
Packer.toBuffer(doc).then(buf => {
fs.writeFileSync("/home/daytona/workspace/spinal-cord-study-guide/Spinal_Cord_Tracts_Study_Guide.docx", buf);
console.log("Done");
}).catch(e => { console.error(e); process.exit(1); });
cd /home/daytona/workspace/spinal-cord-study-guide && node generate.js 2>&1
~/spinal-cord-study-guide/generate.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/spinal-cord-study-guide/generate.js'
cd /home/daytona/workspace/spinal-cord-study-guide && node generate.js 2>&1
python /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/worksp…
ls -lh /home/daytona/workspace/spinal-cord-study-guide/Spinal_Cord_Tracts_Study_…
Spinal Cord Tracts Study Guide
Word Document · DOCX
| Section | Content |
|---|---|
| 1. Overview | Funiculi, general rules of ascending/descending tracts |
| 2. Ascending Tracts | Posterior column-DCML, spinothalamic, spinoreticular, spinomesencephalic, spinocerebellar tracts - full 3-neuron relay, decussation sites, lesion effects |
| 3. Descending Tracts | Pyramidal (lateral + anterior CST with full course table), extrapyramidal (rubrospinal, vestibulospinal, reticulospinal x2, tectospinal) |
| 4. Master Summary Table | All 14 tracts - type, column, origin, decussation, function in one reference table |
| 5. Clinical Cord Syndromes | Brown-Séquard, central cord, anterior cord, posterior column, complete transection, subacute combined degeneration |
| 6. UMN vs LMN | Quick-reference comparison table |
| 7. Memory Aids | Decussation sites, mnemonics (PPVS, DOVE, lateral vs medial system rules) |
| 8. Quick-Review Q&A | 12 exam-style questions with answers |