Pathogenesis of thrombosis in short.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the content needed. Here is the full answer:
Pathogenesis of Thrombosis
Thrombosis is the formation of a solid blood clot (thrombus) within the vascular system in a living person. The fundamental framework is Virchow's Triad, which identifies three interacting abnormalities that predispose to clot formation.
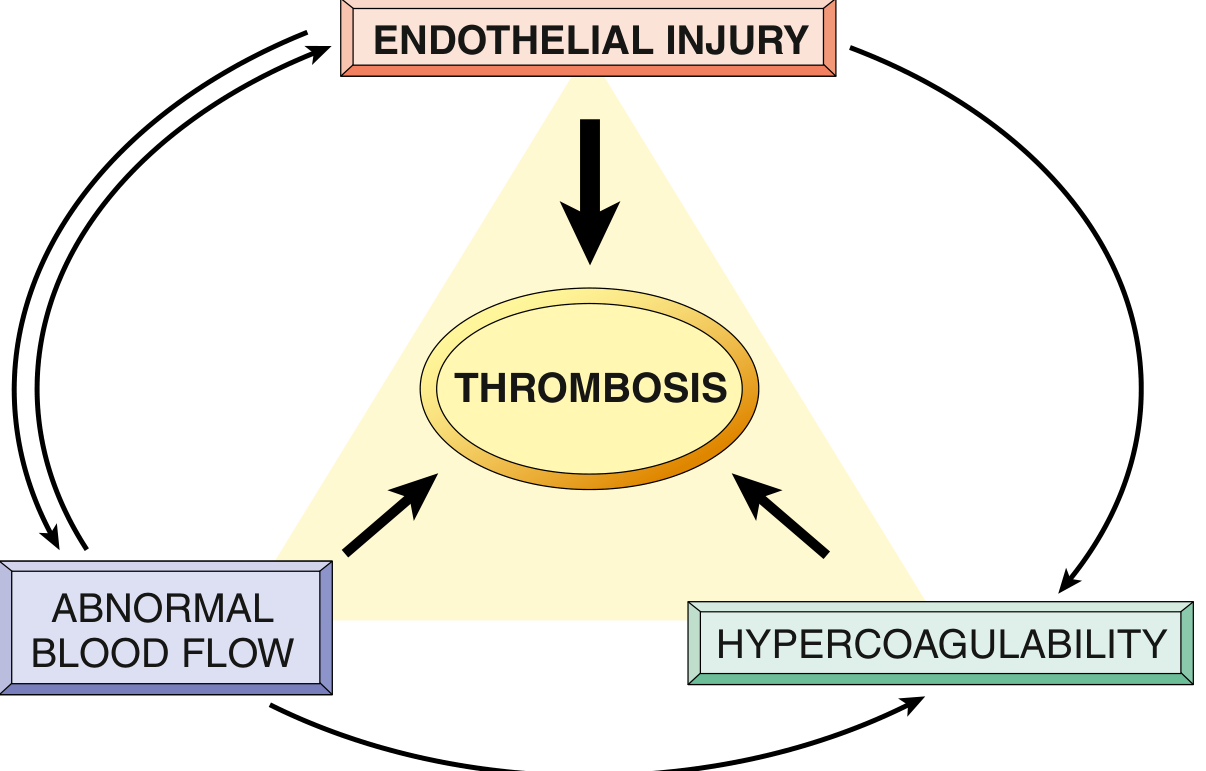
1. Endothelial Injury
Endothelial injury is the most important factor and virtually always underlies arterial and cardiac thrombosis (where high flow would otherwise prevent clotting).
- Direct injury exposes subendothelial von Willebrand factor (vWF) and tissue factor, triggering platelet adhesion and activation of the coagulation cascade.
- Endothelial activation/dysfunction (without frank injury) is triggered by: physical trauma, infectious agents, cytokines, turbulent flow, hypercholesterolemia, homocystinemia, and cigarette smoke toxins.
- Activated endothelium shifts to a prothrombotic phenotype:
- Downregulates thrombomodulin, endothelial protein C receptor, and tissue factor pathway inhibitor (TFPI)
- Upregulates tissue factor expression
- Increases secretion of plasminogen activator inhibitors (PAI), reducing fibrinolysis
- Arterial/cardiac thrombi are platelet-rich ("white thrombi") due to the high-shear environment.
2. Abnormal Blood Flow (Stasis or Turbulence)
Turbulence contributes to arterial and cardiac thrombosis by:
- Causing endothelial injury/dysfunction
- Creating countercurrents and local pockets of stasis
Stasis is the dominant factor in venous thrombosis. It causes:
- Platelets and leukocytes to accumulate at the vessel wall (normally separated from endothelium by laminar flow)
- Slowed washout of activated clotting factors
- Impaired inflow of clotting factor inhibitors
- Activation of endothelial gene expression, promoting a procoagulant state
Clinical examples: Atrial fibrillation, mitral stenosis, ventricular aneurysm, aortic aneurysm, polycythemia vera, ulcerated atherosclerotic plaques, prolonged immobility.
3. Hypercoagulability
Abnormally high tendency of blood to clot, usually from altered coagulation factors. More important in venous thrombosis.
Primary (genetic) causes:
- Factor V Leiden mutation - renders Factor V resistant to cleavage by protein C; heterozygotes have 3-4x risk, homozygotes 25-50x risk; found in ~60% of patients with recurrent DVT
- Prothrombin G20210A mutation - 3' UTR variant causing elevated prothrombin levels; ~3x venous thrombosis risk
- Antithrombin III deficiency
- Protein C or Protein S deficiency - loss of the key anticoagulant pathway
- Elevated homocysteine (anti-phospholipid syndrome-like effects)
Secondary (acquired) causes:
- Prolonged immobility or bed rest
- Myocardial infarction, congestive heart failure
- Cancer (especially mucin-secreting adenocarcinomas - Trousseau syndrome)
- Pregnancy and the postpartum state
- Oral contraceptives/hormone replacement therapy
- Antiphospholipid antibody syndrome
- Heparin-induced thrombocytopenia (HIT)
- Disseminated intravascular coagulation (DIC)
Fate of a Thrombus
Once formed, a thrombus can undergo four outcomes:
| Outcome | Description |
|---|---|
| Propagation | Enlarges by accretion of platelets and fibrin |
| Embolization | Part/all dislodges and travels downstream |
| Dissolution | Fibrinolysis (only effective in early/fresh thrombi; older thrombi resist plasmin) |
| Organization & Recanalization | Ingrowth of endothelial cells, smooth muscle, fibroblasts; may restore partial flow |
The diagram below shows normal endothelial antithrombotic mechanisms (thrombomodulin, protein C/S, antithrombin, TFPI, PGI2/NO, t-PA) that are lost or suppressed when the endothelium is injured or activated:
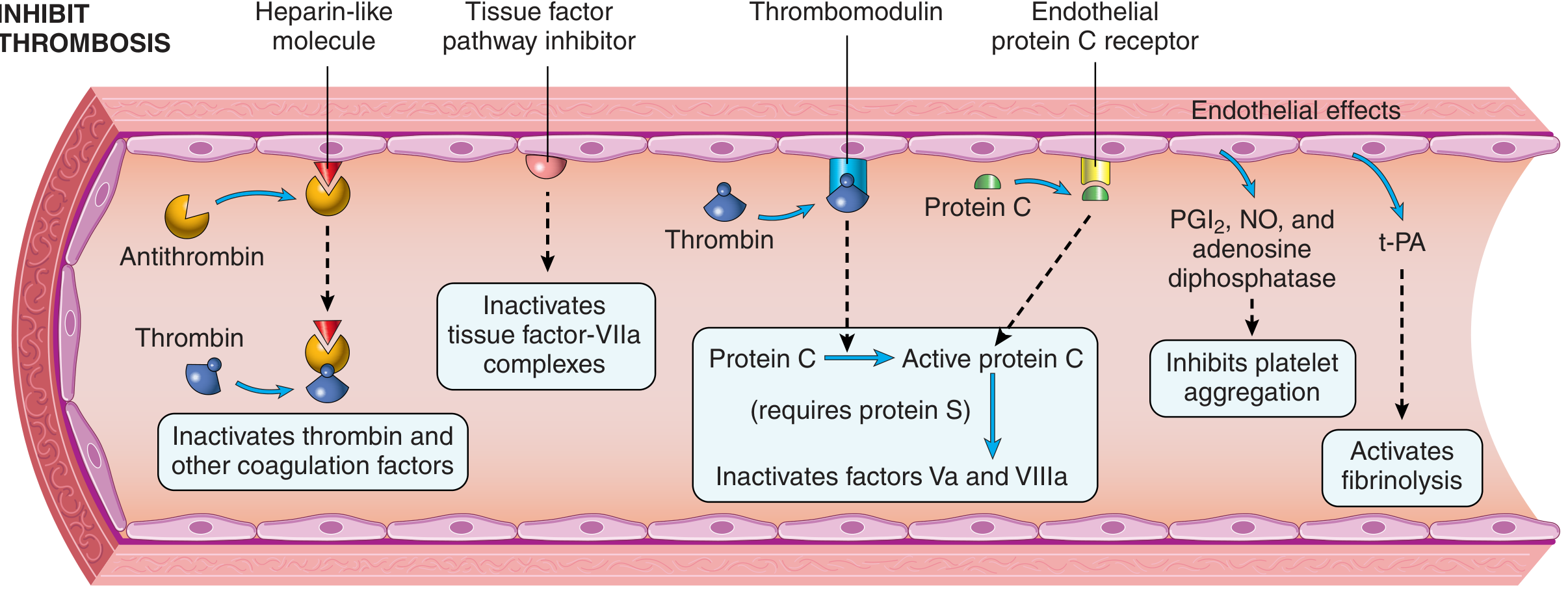
- Robbins & Kumar Basic Pathology, pp. 88-91
This is a shared conversation. Sign in to Orris to start your own chat.