A 55 years old male with history of falling two years ago feel pain in left shoulder region now on again fall pain increase in shoulder region also feel stiffness of neck muscle say feel like stretching of left eye sometime and now headache head stiffness pain increase on lifting arm upward pain increase on shoulder region when he keep arm straight there is no previous history of any medical condition kindly suggest what will be diagnosis any medicine?
cervical spondylosis shoulder pain radiculopathy
Clinical Assessment
⚠️ Important Disclaimer: This is educational information only. The patient must be evaluated in person by a qualified physician — no diagnosis should be made or treatment started without proper clinical examination, neurological assessment, and imaging.
Most Likely Diagnosis: Cervical Spondylosis with Left C5 Radiculopathy (possibly compounded by a Rotator Cuff Pathology)
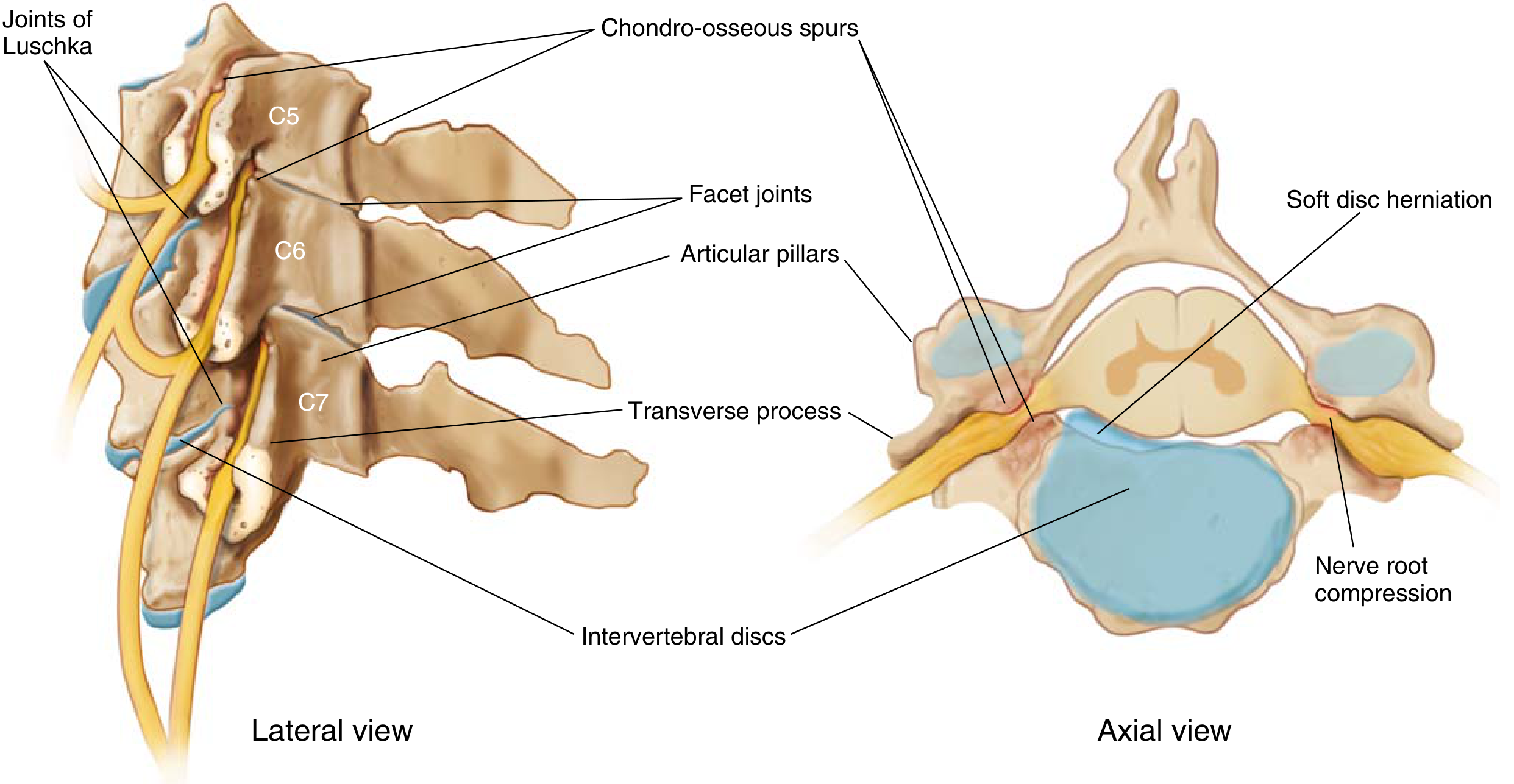
Understanding the Anatomy
Symptom-by-Symptom Analysis
| Patient's Symptom | Clinical Explanation |
|---|---|
| Left shoulder pain (2 years) | C5 root compression: C4–C5 spondylosis causes pain, paresthesias, and sensory loss over the shoulder region |
| Pain worsens with arm raised upward | Abduction/elevation of the arm stretches the C5 root — classic radicular aggravation; also possible rotator cuff impingement |
| Pain worsens with arm held straight (extended) | Brachial stretch sign — stretching the compressed nerve root increases pain |
| Neck stiffness | Loss of cervical flexibility due to disc degeneration, osteophyte formation, and facet arthropathy |
| Headache + head stiffness | Cervical spondylosis causes occipital neuralgia and referred headache — extremely common |
| "Stretching" sensation in the left eye | Referred pain from upper cervical (C2–C3) involvement or occipital nerve irritation radiating to the periorbital/eye region |
| History of falls (triggering/worsening) | Trauma (even minor) can precipitate acute disc herniation or exacerbate existing spondylotic nerve root compression |
| Age 55, male | Peak incidence of cervical spondylosis is 40–50 years, males more affected than females |
Differential Diagnoses to Consider
- Cervical spondylotic radiculopathy (C5) — Most likely ✅
- Cervical disc herniation (C4–C5 or C5–C6) — Often coexists
- Rotator cuff tear / impingement syndrome — Pain on arm elevation; could be a co-existing shoulder pathology worsened by the fall
- Adhesive capsulitis (frozen shoulder) — Shoulder pain with restricted movement; however, stiffness here appears to be primarily cervical
- Cervical myelopathy — If cord is compressed (check for gait problems, hand clumsiness, bladder symptoms)
- Brachial plexopathy — Less likely without trauma to the brachial region
- Referred cardiac pain — Must exclude in a 55-year-old male with left-sided arm/shoulder pain (check for exertional chest pain, ECG)
Key Clinical Tests to Perform
- Spurling's Test: Neck extension + lateral flexion to the left + axial compression → reproduces left shoulder/arm pain = positive for C5 radiculopathy
- Cervical distraction test: Manual traction of the neck → if it relieves pain, confirms root compression
- Shoulder abduction relief sign: Placing the arm on top of the head relieves radicular pain
- Neurological exam: Test deltoid (C5), biceps reflex (C5–C6), sensation over lateral shoulder
Investigations Required
- MRI cervical spine — Gold standard; identifies nerve root compression, disc herniation, osteophytes, canal stenosis
- X-ray cervical spine (AP + lateral) — Shows disc space narrowing, osteophytes, loss of lordosis
- Shoulder X-ray — Rule out rotator cuff calcification or glenohumeral arthritis
- ECG + cardiac workup — Essential in a 55-year-old male with left arm symptoms
- EMG/NCS — If diagnosis remains unclear; loss of CMAP amplitude with preserved SNAP suggests radiculopathy
- MRI shoulder — If rotator cuff tear suspected
Management
Conservative (First Line — Effective in Most Cases)
| Drug | Dose | Purpose |
|---|---|---|
| Diclofenac sodium (NSAID) | 50 mg twice daily with food | Anti-inflammatory, pain relief |
| Methocarbamol or Cyclobenzaprine | 500 mg TDS or 5 mg TDS | Muscle relaxant for neck stiffness |
| Pregabalin or Gabapentin | 75–150 mg BD or 300 mg BD | Neuropathic/radicular pain |
| Pantoprazole | 40 mg once daily | GI protection with NSAIDs |
| Vitamin B12 + B complex | Once daily | Nerve support |
Note: These medications must be prescribed by a licensed physician after proper clinical evaluation. Dosing must be individualized.
- Soft cervical collar — Short-term immobilization to reduce root tension
- Physiotherapy / cervical traction — Reduces foraminal pressure on the nerve root
- Heat therapy to neck and shoulder for muscle stiffness
- Postural correction — Avoid prolonged neck flexion (phones, screens)
- Rotator cuff strengthening exercises (after acute pain subsides)
If Conservative Fails (After 6–8 Weeks)
- Epidural corticosteroid injection (cervical transforaminal steroid injection) — Good for radicular pain
- Surgery (ACDF — Anterior Cervical Discectomy and Fusion) — Reserved for:
- Unrelenting pain despite adequate conservative treatment
- Progressive weakness in the C5 territory (deltoid, biceps)
- Signs of myelopathy (cord compression)
Red Flags — Seek Urgent Evaluation If:
- 🚨 Progressive weakness or paralysis of the arm
- 🚨 Loss of bladder/bowel control (suggests myelopathy)
- 🚨 Bilateral arm/leg symptoms
- 🚨 Chest pain, breathlessness, jaw pain (cardiac cause must be excluded urgently in a 55-year-old male)
- 🚨 Night sweats, unexplained weight loss (rule out malignancy)
Summary
psa normal ramge
PSA (Prostate-Specific Antigen) — Normal Range
General Reference Range
| PSA Level | Interpretation |
|---|---|
| 0 – 4.0 ng/mL | Normal (standard cutoff) |
| 4.0 – 10.0 ng/mL | "Grey zone" — suspicious, biopsy may be needed |
| > 10.0 ng/mL | High — significant risk of prostate cancer |
The normal reference range is 0 to 4 ng/mL — Henry's Clinical Diagnosis and Management by Laboratory Methods
Age-Specific PSA Reference Ranges
| Age Group | Normal PSA Upper Limit |
|---|---|
| 40–49 years | ≤ 2.5 ng/mL |
| 50–59 years | ≤ 3.5 ng/mL |
| 60–69 years | ≤ 4.5 ng/mL |
| 70–79 years | ≤ 6.5 ng/mL |
PSA Velocity (Rate of Rise)
- A PSA rise of > 0.75 ng/mL per year is considered suspicious for prostate cancer, even if the absolute value is within normal range.
Important Caveats
- ✅ BPH (Benign Prostatic Hyperplasia) — most common cause
- ✅ Acute prostatitis (infection/inflammation)
- ✅ Prostate biopsy or instrumentation — causes transient spike
- ✅ Digital rectal examination (DRE) — mild transient rise
- ✅ Ejaculation — can slightly raise PSA (check after 48 hrs abstinence)
- ✅ Urinary tract infection
- 15% of men with PSA < 4.0 ng/mL still have prostate cancer on biopsy (Textbook of Family Medicine)
- PSA is a screening tool, not a definitive diagnostic test
Free vs. Total PSA Ratio
| Free/Total PSA Ratio | Cancer Risk |
|---|---|
| > 25% | Low risk |
| 10–25% | Intermediate |
| < 10% | High risk — biopsy strongly recommended |
Screening Recommendations
- Age 50 — Routine PSA screening for average-risk men
- Age 40–45 — Earlier screening for high-risk men (family history of prostate cancer, African-American men)
how to differentiate between reactive arthritis ajd septic arthritis
Differentiating Reactive Arthritis vs. Septic Arthritis
1. Definition
| Feature | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Nature | Aseptic — sterile joint inflammation triggered by a remote infection | Septic — direct bacterial invasion of the joint |
| Organisms in joint | ❌ None (joint is sterile) | ✅ Bacteria present in synovial fluid |
| Mechanism | Immune-mediated response to antigens from a distant site | Hematogenous seeding, direct inoculation, or spread from adjacent infection |
"Reactive arthritis is an aseptic arthritis that occurs subsequent to an extra-articular infection, most typically of the gastrointestinal or genitourinary tract." — Goldman-Cecil Medicine
"Septic arthritis is an orthopedic emergency... leads to loss of function in 25–50% of patients." — Rosen's Emergency Medicine
2. Preceding History
| Feature | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Preceding infection | Yes — GI (diarrhea, dysentery) or GU (urethritis, STI) infection 1–3 weeks before arthritis | May have bacteremia, skin breach, recent joint surgery, or no clear source |
| Triggering pathogens | Chlamydia trachomatis (GU), Salmonella, Shigella, Yersinia, Campylobacter (GI) | S. aureus (most common), Streptococcus, N. gonorrhoeae (in sexually active), gram-negatives |
| Latency period | Arthritis appears 1–3 weeks AFTER infection | Arthritis is simultaneous with systemic infection / bacteremia |
3. Clinical Features
| Feature | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Joint pattern | Asymmetric oligoarthritis (2–4 joints); lower limbs favored (knee, ankle, heel) | Usually monoarticular (1 joint); knee (50%), hip (25%), shoulder (15%) |
| Fever | Mild or absent | Present in >80% of children, 40–60% of adults |
| Systemic toxicity | Mild | Often significant — sepsis, tachycardia, hypotension possible |
| Extra-articular features | Classic triad: urethritis + conjunctivitis + arthritis (Reiter's syndrome); also oral ulcers, keratoderma blennorrhagica, circinate balanitis | Absent — no mucosal or skin triad |
| Age group | Young adults 20–40 years | Any age; elderly and immunocompromised at higher risk |
| Onset | Subacute over days–weeks | Acute, rapid onset — hours to days |
| Enthesitis / dactylitis | Present (heel pain, Achilles tendinitis, "sausage digit") | Absent |
| HLA-B27 | Positive in 50–80% (associated with axial involvement and chronicity) | Not relevant |
4. Synovial Fluid Analysis — The Most Important Differentiator
| Parameter | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Appearance | Yellow, turbid (inflammatory) | Cloudy, turbid, may be purulent |
| WBC count | 2,000–50,000/mm³ (inflammatory range) | >25,000/mm³ (typically >50,000–100,000) |
| PMN (neutrophils) | >50%, may be >90% | >90% |
| Gram stain | Negative (no organisms) | Positive in 50–60% of confirmed cases |
| Culture | Sterile — no growth | Positive — organisms grow |
| Crystal analysis | Negative | Negative (unless concurrent gout) |
| Antigen testing | May be positive (e.g., Chlamydia, Salmonella antigens) | Not applicable |
"The diagnosis of septic arthritis is established by culture and by analysis of synovial fluid, in which the white blood cell count typically exceeds 25,000/μL, with 90% neutrophils... synovial fluid culture is almost always positive." — Goldman-Cecil Medicine
"In reactive arthritis, synovial fluid demonstrates an inflammatory pattern. The joint fluid is sterile, although antigen testing for Chlamydia, Salmonella, or Yersinia may be positive." — Rosen's Emergency Medicine
5. Laboratory Investigations
| Test | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Blood cultures | Negative | Positive in 30–50% of cases |
| CRP / ESR | Elevated | Markedly elevated |
| WBC (blood) | Mildly elevated | Markedly elevated (leukocytosis) |
| Procalcitonin | Normal to mildly elevated | Often elevated |
| HLA-B27 | Often positive | Not relevant |
| STI screen / stool culture | Positive for triggering pathogen | Not applicable |
| Urine NAAT (Chlamydia) | May be positive | Not applicable |
6. Imaging
| Finding | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| X-ray | Abnormalities at tendon insertion sites (enthesopathy); asymmetric periostitis | Initially normal; later shows joint space narrowing, bone destruction |
| MRI | Enthesitis, sacroiliitis (if axial involvement) | Joint effusion, bone marrow edema, periarticular involvement |
| Ultrasound | Effusion | Effusion (guides arthrocentesis) |
7. Management
| Approach | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Antibiotics | Not routinely needed (sterile joint); treat underlying infection (e.g., doxycycline for Chlamydia) | Mandatory — orthopedic emergency; empirical IV antibiotics immediately |
| First-line empirical antibiotic | N/A (treat trigger) | Vancomycin (for MRSA coverage) ± ceftriaxone (for GN/gonococcal) |
| Anti-inflammatory | NSAIDs — very effective; intra-articular corticosteroids | NSAIDs adjunctively; no steroids in joint until infection excluded |
| Joint drainage | Not routinely needed | Mandatory — joint wash-out (surgical or repeated needle aspiration) |
| DMARDs | Sulfasalazine for chronic/severe cases | Not applicable |
| Urgency | Urgent, but not a surgical emergency | Orthopedic emergency — delay causes permanent cartilage destruction |
8. Quick Summary Table
| Parameter | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Joint sterile? | ✅ Yes | ❌ No |
| Prior infection 1–3 weeks before? | ✅ Yes (GI/GU) | ❌ Usually no |
| Fever | Mild/absent | Usually present |
| Extra-articular features (triad) | ✅ Urethritis, conjunctivitis, skin | ❌ Absent |
| Gram stain/culture positive | ❌ No | ✅ Yes |
| Synovial WBC | <50,000 (inflammatory) | >50,000–100,000 |
| HLA-B27 | Often positive | Not relevant |
| Treatment | NSAIDs + treat trigger | IV antibiotics + surgical drainage (emergency) |
| Prognosis | Mostly self-limited (2–3 months) | Risk of permanent joint damage if delayed |
mild effusion is present on usg in septic or reactive arthritsu
Mild Effusion on USG: Septic or Reactive Arthritis?
The Direct Answer
"The degree of effusion is not reliable in differentiating between infective and non-infective arthritis." — Grainger & Allison's Diagnostic Radiology
What USG Tells You (and Doesn't Tell You)
| USG Finding | Interpretation |
|---|---|
| Effusion present | Confirms joint fluid — present in BOTH septic and reactive arthritis |
| Mild effusion | More consistent with reactive arthritis, transient synovitis, or early inflammation — but does NOT exclude septic arthritis |
| Moderate-to-large effusion | More typical of septic arthritis (especially in knee, hip) — but not exclusive |
| Synovial thickening + hypervascularity (power Doppler) | Suggests active synovitis — seen in BOTH conditions |
| Echogenic fluid / debris / septations in effusion | More suggestive of septic arthritis (pus) |
| Simple, anechoic (clear) effusion | More consistent with reactive/inflammatory arthritis |
| No effusion on hip USG | Strongly argues against septic arthritis of the hip |
"Ultrasound is a rapid and noninvasive method for detecting the presence of a joint effusion... A negative ultrasound of the hip with absence of fluid generally rules out septic arthritis." — Rosen's Emergency Medicine
Key Point: Mild Effusion Leans More Toward Reactive Arthritis — But You Must Aspirate
| Scenario | Likely Diagnosis |
|---|---|
| Mild, anechoic effusion + sterile-looking fluid + young patient + recent GI/GU infection + extra-articular features | Reactive arthritis more likely |
| Mild effusion + fever + acute onset + no preceding infection + diabetic/immunocompromised | Septic arthritis cannot be excluded — aspirate regardless |
| Moderate-large effusion + turbid/echogenic fluid + systemic toxicity | Septic arthritis until proven otherwise |
The Only Way to Definitively Differentiate
| Finding | Reactive Arthritis | Septic Arthritis |
|---|---|---|
| Fluid appearance | Yellow, slightly cloudy | Turbid / frankly purulent |
| WBC count | 2,000–50,000/mm³ | >50,000/mm³ (often >100,000) |
| Gram stain | Negative | Positive in 50–60% |
| Culture | Sterile | Positive — bacteria grow |
| PMN% | >50% | >90% |
Per proposed guidelines (Rosen's): WBC >50,000/mm³ with PMN >90% = positive for pyogenic (septic) arthritis; WBC <5,000/mm³ with PMN <25% = negative → consider reactive arthritis, transient synovitis, or traumatic arthritis.
Practical Clinical Rule
Do NOT use effusion size on USG to rule in or rule out septic arthritis. USG confirms effusion is present and guides aspiration needle placement. Always aspirate the joint when septic arthritis is clinically suspected, regardless of how mild the effusion looks on ultrasound.

what does joint xray depict
X-Ray Analysis — Two Films Present
Film 1 (Top): Chest X-Ray (PA view)
Findings:
- The cardiac silhouette appears mildly to moderately enlarged — cardiothoracic ratio appears to approach or exceed 0.5
- Suggestive of cardiomegaly
- There is increased haziness / opacity in the lower zones bilaterally, more prominent on the right
- The right costophrenic angle appears blunted — possible pleural effusion (right > left)
- Central perihilar haziness is noted — consistent with pulmonary vascular congestion / interstitial edema
- Left lung fields appear more aerated but with some perihilar opacification
- A small metallic density (likely a surgical clip or staple, or possibly an old foreign body) is visible in the left hilar/perihilar region
- Bilateral ribs visible; no obvious rib fractures seen
- Mediastinum appears centrally positioned
Impression — Chest X-Ray:
Cardiomegaly with features of pulmonary venous congestion and possible right-sided pleural effusion — findings consistent with congestive heart failure (CCF) or fluid overload. Clinical correlation with JVP, bilateral leg edema, and echocardiography recommended.
Film 2 (Bottom): Knee Joint X-Ray — AP and Lateral Views
Findings:
- Medial compartment joint space appears narrowed compared to the lateral compartment on the AP view — a hallmark of osteoarthritis
- Lateral compartment appears relatively preserved
- Bones appear normal density — no obvious osteoporosis
- The bony contours are largely intact
- Possible marginal osteophyte formation at the medial tibial and femoral condyles — consistent with degenerative change
- Possible mild subchondral sclerosis (increased whiteness/density below the articular surface) in the medial compartment
- Patella visible on lateral view; no fracture identified
- No obvious calcification in periarticular soft tissues
- No obvious joint effusion density (though plain X-ray is insensitive for effusion)
- No acute fracture lines visible
Impression — Knee X-Ray:
Early-to-moderate medial compartment osteoarthritis of the knee — characterized by medial joint space narrowing, possible marginal osteophytosis, and subchondral sclerosis. No acute fracture seen.
Summary Table
| Film | View | Key Finding | Likely Diagnosis |
|---|---|---|---|
| Chest | PA | Cardiomegaly, lower zone haziness, blunted right CP angle | Congestive Heart Failure / Pulmonary edema |
| Knee | AP + Lateral | Medial joint space narrowing, osteophytes, subchondral sclerosis | Osteoarthritis (medial compartment) |
⚠️ Disclaimer: This is an educational analysis based on visual inspection of a photograph of X-ray films. Image quality is suboptimal (photo of a film, not a digital DICOM). Final radiological interpretation must be done by a qualified radiologist on original high-resolution images with full clinical context.

explaim
Master Chart of Investigations — Full Interpretation
⚠️ Disclaimer: This is an educational analysis. Final clinical decisions must be made by the treating physician with full clinical context.
1. HAEMOGRAM (CBC)
| Parameter | Values Seen | Normal Range | Status |
|---|---|---|---|
| Hb (Haemoglobin) | 12.5 / 13.5 / 12.4 g/dL | Male: 13–17 g/dL | 🔴 Low — mild anaemia |
| TLC (Total Leukocyte Count) | 16.52 / 15.0 (×10³/μL) | 4–11 ×10³/μL | 🔴 High — leukocytosis |
| DLC (Differential) | 93/3 / 85/07 | N: 40–70%, L: 20–40% | 🔴 Neutrophilia (93%, 85%) — suggests bacterial infection / sepsis |
| PLT (Platelets) | 90 / 90 (×10³/μL) | 150–400 ×10³/μL | 🔴 Thrombocytopenia |
| MCV | 144 / 184 fL | 80–100 fL | 🔴 Markedly elevated — Macrocytosis |
| PCV (Haematocrit) | 02/30 / 91/30 | 40–54% (male) | Appears low |
| Retic | 38 / 36 | 0.5–2.5% | 🔴 Elevated — active erythropoiesis / haemolysis |
| ESR | 30 | <20 mm/hr (male) | 🔴 Elevated — inflammation |
| RDW | noted | 11.5–14.5% | Values partially visible |
Haemogram Summary:
Anaemia (mild) + Leukocytosis with neutrophilia + Thrombocytopenia + Macrocytosis + Elevated reticulocyte count + Raised ESR This pattern raises concern for:
- Sepsis / bacterial infection (leukocytosis + neutrophilia + raised ESR)
- Haemolytic anaemia or B12/folate deficiency (macrocytosis + elevated reticulocytes)
- Hypersplenism or consumptive process (thrombocytopenia)
2. ELECTROLYTES
| Parameter | Values | Normal Range | Status |
|---|---|---|---|
| Na⁺ (Sodium) | 124 → 140 → 119 → 119 → 141 mEq/L | 135–145 mEq/L | 🔴 Hyponatraemia in most readings (119–124) |
| K⁺ (Potassium) | 4.0 / 3.3 / 4.33 / 4.33 / 3.59 mEq/L | 3.5–5.0 mEq/L | ✅ Mostly normal (3.3 slightly low) |
Key Finding:
Persistent hyponatraemia (Na as low as 119 mEq/L) — this is severe hyponatraemia and can cause confusion, seizures, cerebral oedema. Needs urgent correction with careful fluid/sodium management.
3. ARTERIAL BLOOD GAS (ABG)
| Parameter | Values | Normal | Status |
|---|---|---|---|
| pH | 7.36 / 7.39 / 7.41 / 7.41 / 7.33 | 7.35–7.45 | Last reading: 🔴 Acidosis (7.33) |
| PCO₂ | 39 / 40 / 44 / 44 / 36 mmHg | 35–45 mmHg | ✅ Normal range |
| HCO₃ | 21.5 / 24 / 27.9 / 27 / 23 mEq/L | 22–26 mEq/L | Mostly normal; some borderline low |
| SaO₂ | not clearly visible | >95% | — |
ABG Interpretation:
- pH 7.33 with PCO₂ 36 and HCO₃ 23 → Metabolic acidosis with respiratory compensation (low pH, normal-to-low PCO₂, low-normal HCO₃)
- Earlier readings (7.39–7.41) were compensated/normal
- Trend shows worsening acidosis over time → concerning for deteriorating metabolic state
4. KFT (Kidney Function Tests)
| Parameter | Values | Normal Range | Status |
|---|---|---|---|
| Urea | 25, 25 mg/dL | 15–40 mg/dL | ✅ Normal |
| Creatinine | 1.0 / 0.89 mg/dL | 0.7–1.3 mg/dL | ✅ Normal |
| 24hr Protein / Creat. Clearance | partially visible | — | — |
KFT Summary:
Kidney function appears preserved — normal urea and creatinine. No evidence of renal failure at this point.
5. SERUM CHEMISTRY
| Parameter | Values | Normal Range | Status |
|---|---|---|---|
| FBG (Fasting Blood Glucose) | 129 mg/dL | 70–100 mg/dL | 🔴 Elevated — hyperglycaemia / possible diabetes |
| Uric Acid | 5.2 / 4.06 mg/dL | 3.5–7.2 mg/dL | ✅ Normal |
| Calcium | 8.59 / 8.8 mg/dL | 8.5–10.5 mg/dL | ✅ Normal |
| Phosphorus | 1.88 / 2.42 mg/dL | 2.5–4.5 mg/dL | 🔴 Low — hypophosphataemia |
| Mg (Magnesium) | 1.8 mg/dL | 1.7–2.2 mg/dL | ✅ Normal |
6. ENZYMES
| Parameter | Value | Normal Range | Status |
|---|---|---|---|
| CK (Creatine Kinase) | 79 U/L | 30–200 U/L | ✅ Normal |
| LDH (Lactate Dehydrogenase) | 290 U/L | 140–280 U/L | 🔴 Elevated — suggests haemolysis, tissue damage, or malignancy |
| Amy (Amylase) | 76 U/L | 30–110 U/L | ✅ Normal |
| cTnT (Troponin T) | not filled | — | Not done / not visible |
Enzyme Note:
Elevated LDH is significant — in the context of macrocytosis and thrombocytopenia, this strongly points to haemolysis or possibly megaloblastic anaemia (B12/folate deficiency). LDH is markedly elevated in haemolytic anaemia, megaloblastic states, lymphoma, and sepsis.
7. LFT (Liver Function Tests)
| Parameter | Value | Normal Range | Status |
|---|---|---|---|
| Bilirubin | 1.4 / 1.7 mg/dL | Total <1.2 mg/dL | 🔴 Mildly elevated — hyperbilirubinaemia |
| AST (SGOT) | 74 U/L | <40 U/L | 🔴 Elevated |
| ALT (SGPT) | 76 / 50 U/L | <40 U/L | 🔴 Elevated — hepatocellular damage |
| ALP | 83 / 79 U/L | 44–147 U/L | ✅ Normal |
| Protein (Total) | 5.7 / 6.54 g/dL | 6.4–8.3 g/dL | 🔴 Low — hypoproteinaemia |
| Albumin | 3.9 / 3.67 g/dL | 3.5–5.0 g/dL | 🟡 Low-normal / borderline |
| GGT | 49 U/L (noted at bottom) | <50 U/L | 🟡 Upper limit of normal |
LFT Summary:
Raised AST/ALT + elevated bilirubin + low total protein = hepatocellular injury pattern — could be due to infection, drug-induced liver disease, haemolysis (raised bilirubin from RBC breakdown), or systemic illness.
8. COAGULOGRAM
| Parameter | Values Noted | Normal | Status |
|---|---|---|---|
| BT (Bleeding Time) | 1.8 | 2–7 min | ✅ Normal |
| CT (Clotting Time) | 3.17 | 5–11 min | ✅ Normal |
| PTI / INR / PTT / FDP / Dimes | Not clearly filled | — | Pending / not readable |
Overall Clinical Picture — Possible Diagnoses
| Cluster of Findings | Likely Cause |
|---|---|
| Leukocytosis + neutrophilia + raised ESR + metabolic acidosis | Sepsis / severe bacterial infection |
| Macrocytosis (MCV 144–184) + elevated LDH + reticulocytosis + thrombocytopenia + raised bilirubin | Haemolytic anaemia OR megaloblastic anaemia (B12/folate deficiency) |
| Hyponatraemia (Na 119–124) | SIADH, dilutional, or sepsis-related |
| Raised AST/ALT + bilirubin + low protein | Hepatocellular injury (infection, haemolysis, sepsis) |
| Elevated fasting glucose | Diabetes mellitus or stress hyperglycaemia |
| Hypophosphataemia | Malnutrition, refeeding, or systemic illness |
Priority Actions for the Clinician:
- 🔴 Correct hyponatraemia urgently (Na 119 is critically low)
- 🔴 Blood cultures — treat underlying sepsis
- 🔴 Peripheral blood film — look for haemolysis, blast cells, megaloblasts
- 🔴 Serum B12 + Folate — rule out megaloblastic anaemia (MCV 144–184 is very high)
- 🔴 LDH + Direct Coombs Test — confirm haemolytic anaemia
- 🟡 Repeat LFTs — monitor hepatocellular trend
- 🟡 HbA1c — assess diabetic control
septic arthritis
septic arthritis joint pathology bacteria synovium
Septic Arthritis — Complete Review
Definition
Epidemiology
- Incidence: 2–10 per 100,000 in the general population
- Rises to 30–70 per 100,000 in patients with rheumatoid arthritis
- Boys affected twice as often as girls (pediatric)
- Most common joint: Knee (50%), hip (25%), shoulder (15%)
- Lower extremity involved in majority of cases
- Incidence is increasing globally
Pathogenesis & Routes of Infection
| Route | Details |
|---|---|
| Hematogenous (most common) | Bacteremia seeds the synovial membrane (lacks basement membrane — bacteria spread easily into joint) |
| Contiguous spread | From adjacent osteomyelitis, soft tissue infection, or abscess |
| Direct inoculation | Trauma, joint aspiration, injection, surgery, IV drug use |
Bacterial toxins + lysosomal enzymes + neutrophil-released collagenase, elastase, hyaluronidase + matrix metalloproteinases → cartilage destruction begins within 8 hours of inoculation
Causative Organisms (Age-Specific)
| Age Group | Most Common Organisms |
|---|---|
| Neonates (0–3 mo) | Group B Streptococcus, S. aureus, gram-negative organisms, N. gonorrhoeae |
| Infants/Children (3 mo–5 yr) | S. aureus (MSSA and CA-MRSA), Group A Streptococcus, S. pneumoniae |
| Children (5–15 yr) | S. aureus, Kingella kingae |
| Sexually active adolescents/young adults | N. gonorrhoeae — most common in this group |
| Adults >40 yr or with comorbidities | S. aureus — most common overall |
| IV drug users | S. aureus, Pseudomonas aeruginosa, polymicrobial |
| Sickle cell disease | Salmonella spp. (more prevalent than in general population) |
| Prosthetic joints | S. epidermidis, S. aureus, Pseudomonas, Enterobacteriaceae |
⚠️ CA-MRSA is isolated in up to 63% of pediatric cases and can be polymicrobial, rapidly destructive, and involve multiple joints.
Risk Factors
- Age >80 years
- Diabetes mellitus
- Rheumatoid arthritis (20× higher risk)
- Prosthetic joint or recent joint surgery
- Immunosuppression (steroids, chemotherapy, HIV)
- IV drug use
- Skin infection / bacteremia
- Pre-existing joint disease (OA, gout)
- Intravenous catheters
Clinical Features
Symptoms
- Acute-onset severe joint pain (80–100% sensitive)
- Inability to bear weight or move the joint
- Fever — >80% of children, 40–60% of adults
- Constitutional symptoms: malaise, weakness, anorexia (inconsistent)
⚠️ Immunosuppressed patients (especially on corticosteroids) may have minimal pain and no fever — high index of suspicion required.
Signs
| Sign | Details |
|---|---|
| Joint tenderness | 100% sensitive |
| Swelling + warmth + erythema | Cardinal signs of inflammation |
| Restricted range of motion | Any passive/active movement causes severe pain |
| Position of comfort | Limb held in slight flexion to reduce intracapsular pressure |
| Tachycardia / hypotension | Indicates systemic sepsis |
| Pseudoparalysis | In neonates — limb appears paralyzed (mimic of neurologic problem) |
Clinical Images

Investigations
1. Synovial Fluid Analysis (Most Important — Gold Standard)
| Parameter | Septic Arthritis | Normal/Inflammatory |
|---|---|---|
| Appearance | Cloudy, turbid, purulent | Clear/yellow |
| WBC count | >50,000/mm³ (often >100,000) | <2,000 (normal); 2,000–50,000 (inflammatory) |
| PMN % | >90% | Variable |
| Gram stain | Positive in 50–70% (gram +ve), 40–50% (gram −ve), 25% (gonococcal) | Negative |
| Culture | Positive — definitive diagnosis | Sterile |
| Glucose | Low (synovial fluid/blood glucose <0.5) | Normal |
"A positive Gram stain is immediately diagnostic of septic arthritis." — Roberts & Hedges' Clinical Procedures
2. Blood Tests
- WBC — leukocytosis (elevated, but normal does not exclude infection)
- CRP / ESR — elevated
- Blood cultures — positive in 30–50% of non-gonococcal cases; 20–30% of gonococcal cases
- Procalcitonin — elevated in bacterial sepsis
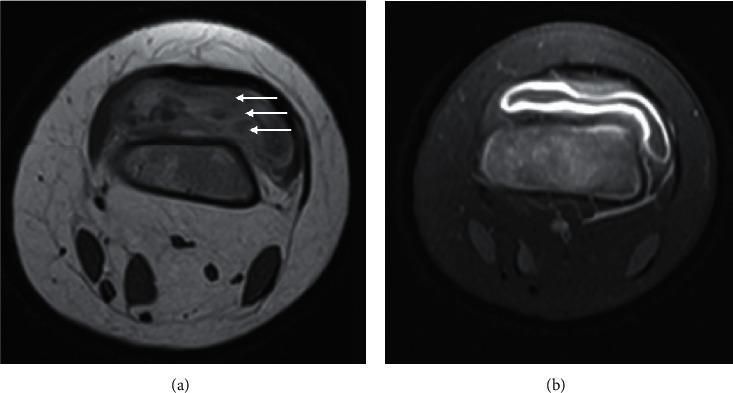
3. Imaging
| Modality | Findings |
|---|---|
| X-ray | Normal early; late: joint space narrowing, bone erosions, subchondral destruction |
| Ultrasound | Detects effusion — guides aspiration; negative hip USG rules out septic arthritis; shows synovial thickening and hypervascularity |
| MRI (preferred) | Gadolinium MRI sensitivity 100%, specificity 77%; shows effusion, synovial enhancement, bone marrow edema, adjacent osteomyelitis. Findings visible within 24 hours of infection |
| CT | Joint effusion, bone erosions; useful if MRI contraindicated |
Kocher Criteria (for pediatric hip — predicts likelihood of septic arthritis)
| No. of Criteria Met | Likelihood of Septic Arthritis |
|---|---|
| 1 | 3% |
| 2 | 40% |
| 3 | 93% |
| 4 | 99% |
Differential Diagnosis
| Condition | Key Differentiating Feature |
|---|---|
| Reactive arthritis | Sterile joint; prior GI/GU infection 1–3 weeks before |
| Gout / Pseudogout | Crystals on polarized light microscopy |
| Transient synovitis | Children; afebrile; WBC <5,000; self-limiting |
| Rheumatoid arthritis | Chronic; bilateral; RF/anti-CCP positive |
| Osteomyelitis | Adjacent bone involved; may coexist with septic arthritis |
| Trauma / Hemarthrosis | History of injury; bloody aspirate with fat droplets (lipohemarthrosis) |
| Lyme arthritis | Endemic area; large effusion; positive Lyme serology |
"The simultaneous occurrence of gout and septic arthritis is possible — a diagnosis of crystal-induced disease should NOT stop a thorough search for infection."
Treatment
1. Joint Drainage — Mandatory, Urgent
Timely decompression via open arthrotomy, irrigation, and debridement is the recommended treatment.
| Method | When Used |
|---|---|
| Needle aspiration (serial) | Accessible joints (knee, ankle, wrist); may need repeat aspiration |
| Arthroscopic lavage | Preferred for knee, shoulder |
| Open arthrotomy | Hip (due to avascular necrosis risk), failed aspiration, complex cases |
⚠️ Hip septic arthritis requires urgent surgical decompression due to risk of avascular necrosis of the femoral head from capsular pressure.
2. Antibiotics — Empirical, Start Immediately
| Age Group | Empirical Antibiotic |
|---|---|
| Neonates | Nafcillin/oxacillin + cefotaxime/cefepime |
| Children >3 months | Vancomycin (for CA-MRSA coverage) |
| Adults — gram-positive | Vancomycin (MRSA coverage) or nafcillin (MSSA) |
| Adults — gram-negative / gonoccal | + Ceftriaxone |
| Gonococcal arthritis | Ceftriaxone 1g IV/IM daily — responds rapidly |
| IV drug users | Vancomycin + anti-pseudomonal coverage |
- IV antibiotics for 2–4 days, then switch to oral if CRP declining and clinical improvement
- Total course: typically 3–6 weeks depending on organism and response
- Blood and joint cultures MUST be obtained BEFORE antibiotics — but do not delay antibiotics if sepsis is present
Complications
| Complication | Details |
|---|---|
| Permanent joint destruction | Cartilage degradation → ankylosis, stiff joint; function lost in 25–50% |
| Osteomyelitis | Infection spreads from joint to bone (or vice versa) |
| Avascular necrosis | Especially femoral head in hip septic arthritis |
| Epiphyseal damage | In children — growth impairment, limb length discrepancy |
| Sepsis / septic shock | Hematogenous spread → endocarditis, pneumonia, systemic sepsis |
| Sinus tracts | Chronic infection → tracking through skin |
Summary Mnemonic: "FAST-AID"
- F — Fever + rapid onset
- A — Acute monoarthritis (usually)
- S — Swelling, warmth, erythema
- T — Tenderness (100% sensitive)
- A — Aspiration mandatory (arthrocentesis)
- I — IV antibiotics (empirical, urgent)
- D — Drainage (surgical/arthroscopic)