ms case tell al findings
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
multiple sclerosis MRI brain periventricular plaques lesions
I now have comprehensive content for a complete MS findings overview. Let me compile everything:
Multiple Sclerosis (MS) — All Findings
Overview
MS is a chronic immune-mediated demyelinating disease of the CNS. It occurs 2–2.5× more often in women, typically manifests in the 3rd–4th decade, and has a prevalence of ~309/100,000 in the US (~730,000 Americans; ~2.8 million worldwide).
Clinical Findings
Presenting Symptoms
| System | Symptoms |
|---|---|
| Visual | Optic neuritis — monocular blurring, pain on eye movement, central scotoma (centrocecal), red color desaturation |
| Sensory | Paresthesias (circumferential, non-dermatomal), bandlike pain around trunk or limb, Lhermitte sign |
| Motor | Limb weakness, spasticity, hyperreflexia |
| Cerebellar | Imbalance, incoordination, intention tremor, scanning speech |
| Bladder | Urgency, frequency, incomplete emptying |
| Fatigue | Most common symptom overall |
| Cognitive/Psych | Depression (37–54%), cognitive slowing, euphoria |
Key Signs on Examination
- Lhermitte sign — electrical sensation down the spine into limbs on neck flexion; indicates cervical cord demyelination
- Optic neuritis — afferent pupillary defect (Marcus Gunn), swollen or normal-appearing disc; visual recovery common but often incomplete
- Internuclear ophthalmoplegia (INO) — impaired adduction of one eye with nystagmus in the abducting eye; due to MLF demyelination — highly suggestive of MS in a young patient
- Sensory levels — incomplete, often asymmetric, may differ by modality (dorsal columns vs. spinothalamic)
- Upper motor neuron signs — hyperreflexia, extensor plantar response (Babinski sign), clonus
- Charcot triad — intention tremor, scanning speech, nystagmus (classic but rare)
- Uhthoff phenomenon — worsening of symptoms with increased body temperature (hot weather, exercise, fever)
MRI Findings (Most Sensitive Investigation — >95% Abnormal in Definite MS)
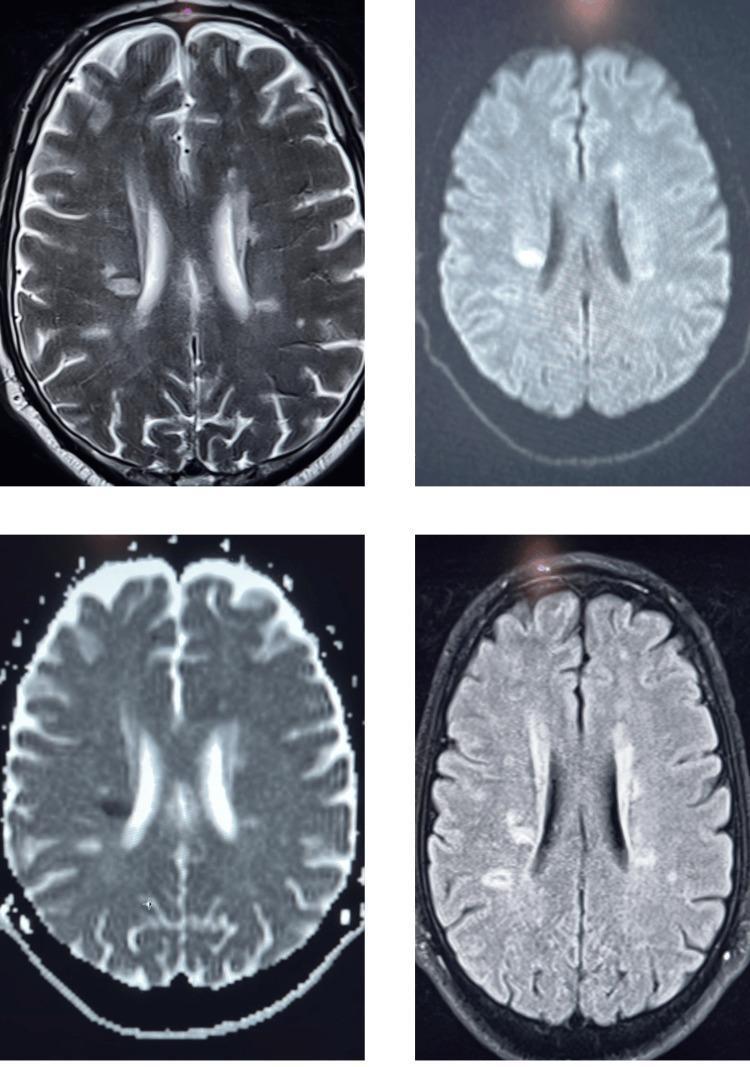
T2 / FLAIR — White Lesions (Most Sensitive)
- Size: 2 mm – 2 cm (occasionally tumor-like)
- Shape: Ovoid, elliptical, discrete borders, no mass effect
- Classic locations (McDonald 2017 criteria — lesions in ≥2 of 4 areas):
- Periventricular — perpendicular to ventricle walls = "Dawson's fingers" (most characteristic)
- Juxtacortical/cortical
- Infratentorial — cerebellar peduncles, brainstem
- Spinal cord — dorsolateral cervical cord
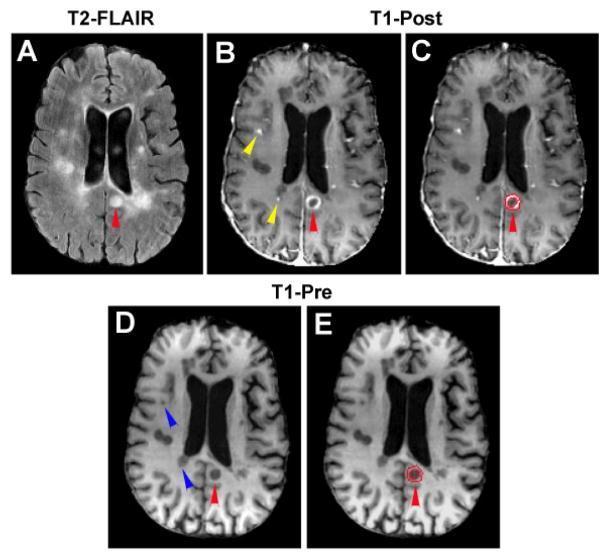
T1 Post-Gadolinium — Active Inflammation
- Gadolinium enhancement = blood-brain barrier breakdown = active/new lesion
- Pattern: homogeneous, central, or ring-enhancing
- Typically persists 2–8 weeks
- Provides evidence for dissemination in time (DIT) when concurrent non-enhancing T2 lesions are present
T1 Pre-Contrast — Chronic Damage
- "Black holes" = persistent T1 hypointensities = axonal loss and atrophy (irreversible damage)
Spinal Cord MRI
- Dorsolateral plaques on sagittal T2; typically <2 vertebral segments (vs. NMO which spans ≥3 segments)
CSF Findings
| Test | Finding |
|---|---|
| Cell count | Mild lymphocytic pleocytosis (usually <50 WBCs/µL); >50 cells or neutrophils is atypical |
| Total protein | Mildly elevated or normal; >100 mg/dL is unusual for MS |
| Glucose | Normal |
| Oligoclonal IgG bands (OCBs) | Present in 85–90% of clinically definite MS (absent in serum = intrathecal production) |
| IgG index | Elevated (>0.7) — indicates intrathecal immunoglobulin synthesis |
| Myelin basic protein | May be elevated but non-specific (elevated in any CNS tissue destruction) |
CSF is not mandatory when clinical + MRI evidence is sufficient; it is recommended when the diagnosis is uncertain or infection/malignancy must be excluded.
Evoked Potentials
| Type | Finding |
|---|---|
| Visual evoked potentials (VEP) | Prolonged P100 latency — most clinically useful; documents subclinical optic nerve lesion |
| Brainstem auditory evoked potentials (BAEP) | Delay of central conduction; wave I may be abnormal |
| Somatosensory evoked potentials (SSEP) | Prolonged central conduction time |
Evoked potentials can reveal clinically silent lesions, aiding in demonstrating dissemination in space.
2017 McDonald Diagnostic Criteria (Summary)
The diagnosis requires evidence of dissemination in space (DIS) and dissemination in time (DIT):
DIS on MRI = ≥1 T2 lesion in ≥2 of 4 regions:
- Periventricular, juxtacortical/cortical, infratentorial, spinal cord
DIT on MRI = simultaneous presence of:
- Asymptomatic gadolinium-enhancing AND non-enhancing T2 lesions, OR
- A new T2/enhancing lesion on follow-up scan
CSF shortcut: Positive CSF-specific oligoclonal bands can substitute for DIT in a clinically isolated syndrome (CIS).
Pathological Findings (Gross & Microscopic)
| Finding | Description |
|---|---|
| Plaques | Sharply demarcated areas of demyelination in white matter ± gray matter |
| Active plaques | Perivascular lymphocytic infiltrates (CD4+/CD8+ T cells, macrophages), myelin stripping |
| Chronic plaques | Hypocellular, gliotic, axonal loss, "shadow plaques" at edges (remyelination) |
| Axonal transection | Occurs even in acute lesions; underlies irreversible disability |
| Cortical demyelination | Common but underdetected by conventional MRI; correlates with cognitive impairment |
Disease Course Subtypes
| Type | Features |
|---|---|
| RRMS (85–90% at onset) | Distinct relapses with full or partial recovery; most common |
| SPMS | Progressive accumulation of disability after initial RR phase |
| PPMS (~10–15%) | Progressive from onset, no relapses; more spinal cord-dominant |
| CIS | First demyelinating event; converts to MS if McDonald criteria are later fulfilled |
Disability Measurement
Expanded Disability Status Scale (EDSS) (Kurtzke scale) — assesses 7 functional systems:
- Pyramidal, cerebellar, brainstem, sensory, bowel/bladder, visual, cerebral
Sources: Goldman-Cecil Medicine 26e, Ch. 380; Harrison's Principles of Internal Medicine 22e, Ch. 50; Bradley and Daroff's Neurology in Clinical Practice
no tell everything about mitral stenosis not multiple sclerosis include images also
Finding Sources
Searching Images
mitral stenosis echocardiography fish mouth valve
Reading File
Reading File
Reading File
Searching Images
mitral stenosis chest X-ray ECG findings
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Here it is:
Mitral Stenosis (MS) — Complete Findings
Definition & Aetiology
Mitral stenosis is obstruction to left ventricular inflow at the mitral valve level, causing a persistent diastolic pressure gradient between the left atrium and left ventricle.
Normal mitral valve area: 4–6 cm²
| Cause | Notes |
|---|---|
| Rheumatic fever (most common worldwide) | Commissural fusion + leaflet thickening; 3× more common in women; pure MS in 40% of rheumatic heart disease |
| Mitral annular calcification (MAC) | Increasing cause in elderly/developed nations |
| Congenital | Parachute mitral valve, supravalvular ring |
| Rare | Ball-valve thrombus, LA myxoma, carcinoid, radiation, mucopolysaccharidosis, cor triatriatum (mimics MS) |
Pathophysiology
- Obstructed LV inflow → ↑ LA pressure → pulmonary venous hypertension → dyspnoea / pulmonary oedema
- Restricted inflow + reflex vasoconstriction → ↓ cardiac output
- Chronic ↑ LA pressure → LA dilatation → atrial fibrillation
- AF with MS: rapid rate shortens diastolic filling time → acute decompensation
- Progressive pulmonary hypertension → RV pressure overload → RV failure
- Symptoms typically appear when MVA < 1.5 cm² (one-third of normal)
Symptoms
| Symptom | Mechanism |
|---|---|
| Dyspnoea on exertion (earliest) | ↑ LA & pulmonary venous pressure |
| Orthopnoea / PND | Pulmonary congestion worsened by recumbency |
| Haemoptysis | Rupture of bronchial–pulmonary venous anastomoses (high LA pressure); characteristic of MS, uncommon in other causes of LA hypertension |
| Palpitations | Atrial fibrillation |
| Ortner syndrome | Hoarseness from compression of left recurrent laryngeal nerve by giant LA |
| Dysphagia | LA impinging on oesophagus |
| Systemic embolism / stroke | LA thrombus (especially LAA) from stasis ± AF |
| Ascites, ankle oedema | Right ventricular failure |
| Fatigue | ↓ cardiac output |
Physical Examination Findings
General & Precordium
- Malar flush (mitral facies) — peripheral cyanosis with rosy cheeks due to ↓ CO + vasoconstriction
- Quiet apical impulse (LV not volume overloaded)
- Parasternal lift — if RV hypertrophy from pulmonary hypertension
Heart Sounds
| Finding | Mechanism |
|---|---|
| Loud S1 (most prominent sign) | Transmitral gradient holds valve open; LV systole closes fully open valve forcefully |
| Opening snap (OS) after S2 | Sudden halt of leaflets; only present if leaflets still mobile (absent if calcified) |
| Short S2–OS interval | High LA pressure; interval 0.04–0.12 sec; closer = more severe |
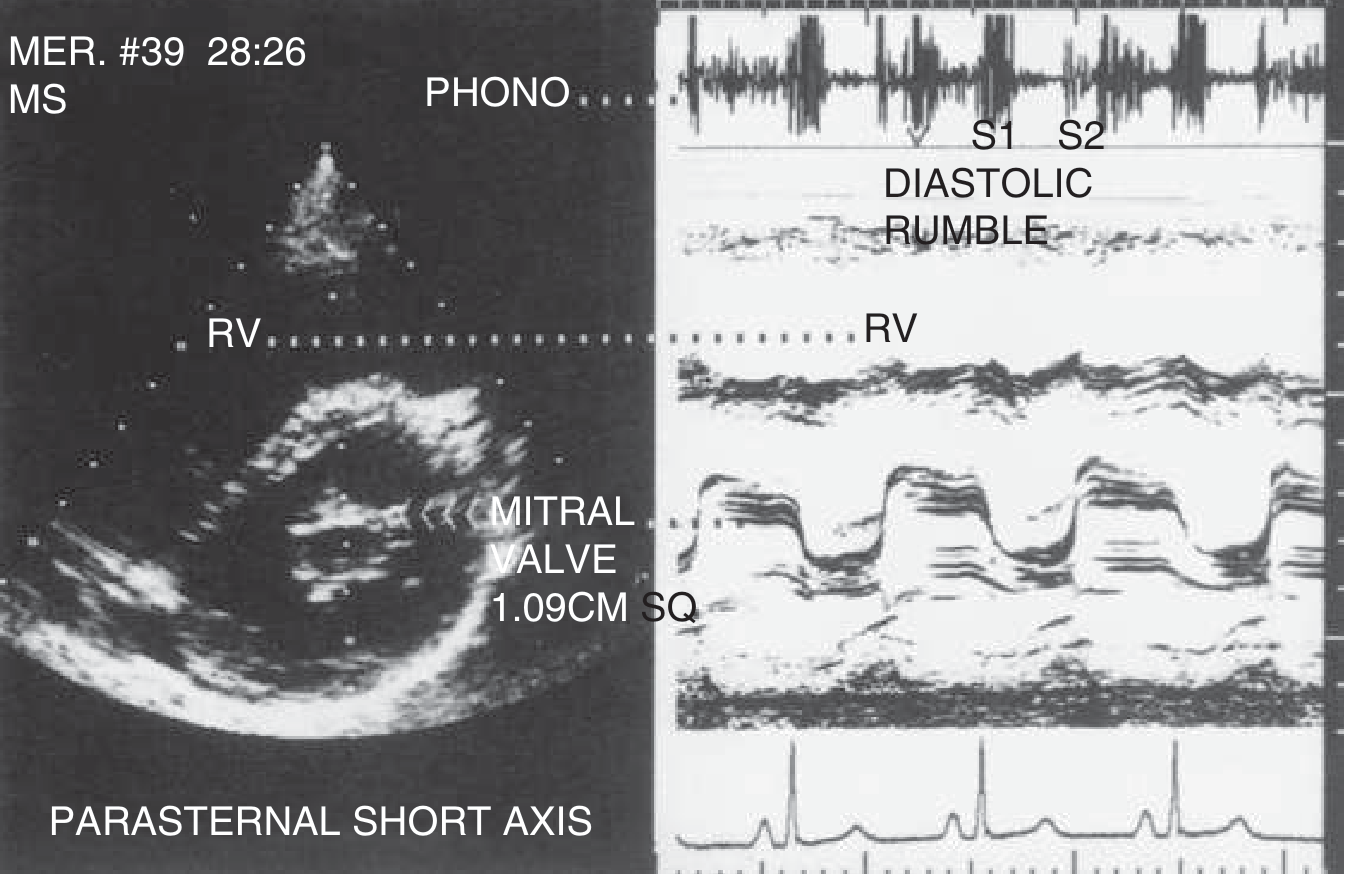
| Low-pitched mid-diastolic rumble at apex | Classic murmur; best heard with bell in LLD position; increases in length as severity worsens |
| Presystolic accentuation | Atrial systole accelerating flow across valve (sinus rhythm only; absent in AF) |
| Graham Steell murmur | High-pitched early diastolic murmur of pulmonary regurgitation from pulmonary hypertension |
| Loud P2 (pulmonic component of S2) | Pulmonary hypertension |
| S3 and S4 absent | Obstruction prevents rapid LV filling |
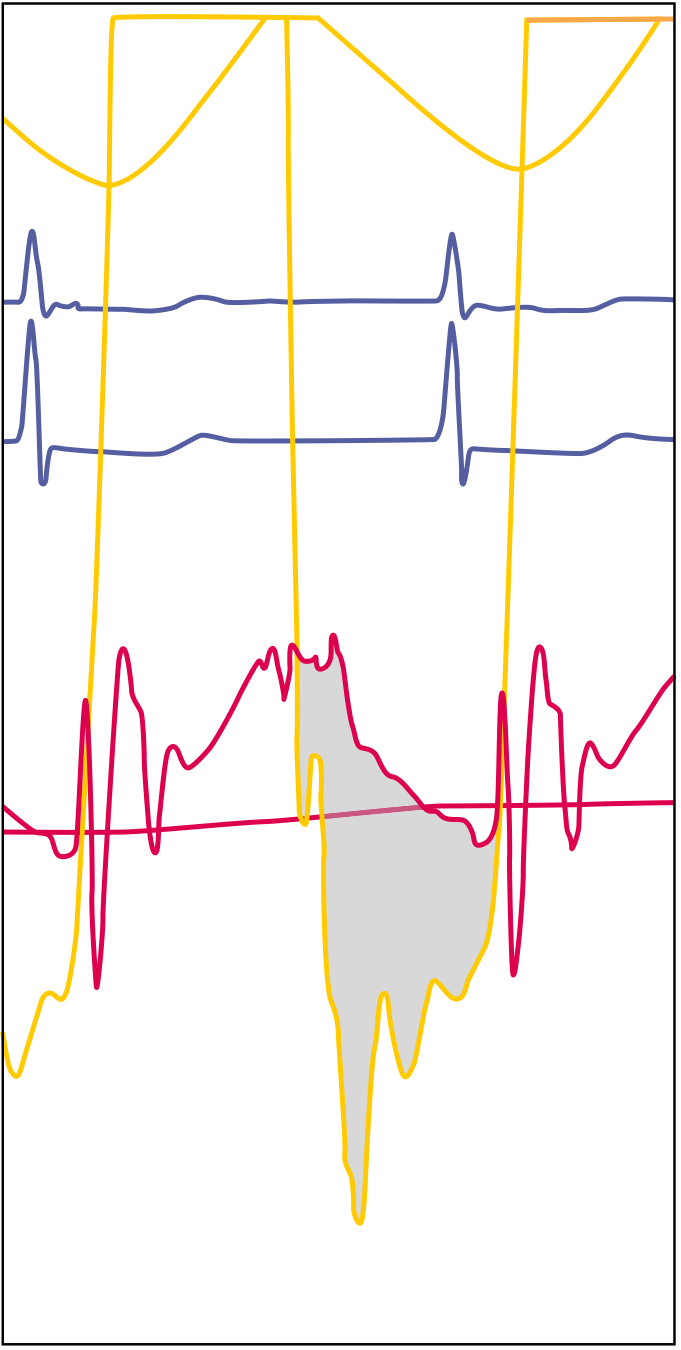
ECG Findings
| Finding | Cause |
|---|---|
| P mitrale — broad, bifid P wave (>0.12 sec) in lead II; biphasic P in V1 | LA enlargement (sinus rhythm) |
| Atrial fibrillation | LA dilatation and rheumatic atrial inflammation |
| Right axis deviation | RV hypertrophy |
| RV hypertrophy pattern — tall R in V1, deep S in V5–V6 | Pulmonary hypertension |
Chest X-Ray Findings
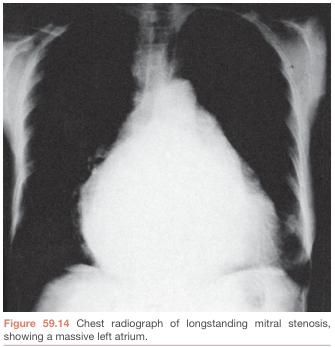
| Feature | Sign |
|---|---|
| Left atrial enlargement | Double shadow at right heart border; straightening of left heart border; elevation of left main bronchus (carinal angle >70°) |
| Mitral valve calcification | Visible on lateral film or fluoroscopy |
| Pulmonary venous hypertension | Upper lobe blood diversion (cephalization); Kerley B lines (horizontal interstitial lines at lung bases) |
| Pulmonary oedema | Bilateral perihilar haziness in decompensated state |
| RV enlargement | Filling of retrosternal space on lateral view |
| Pulmonary artery enlargement | Prominent main pulmonary artery on PA film |
| Overall cardiac silhouette | May be normal or only mildly enlarged (LV is not dilated) |
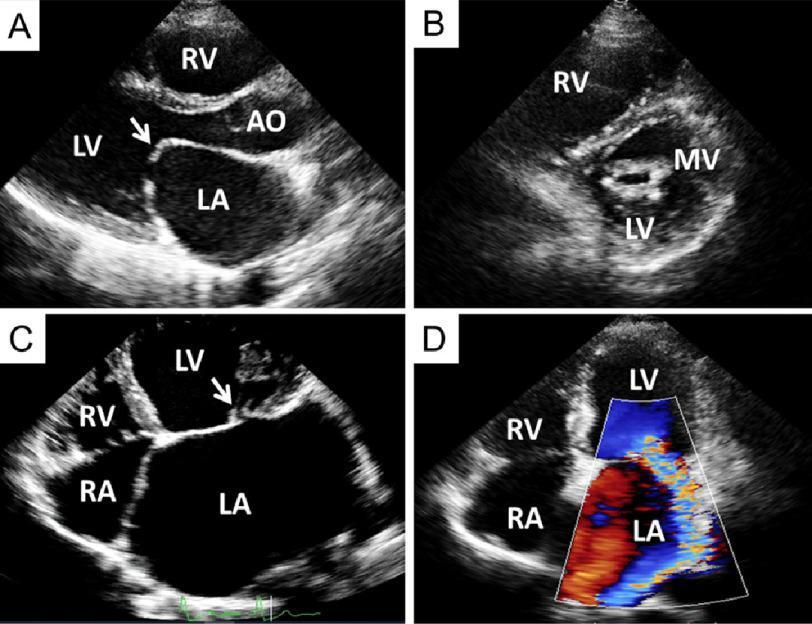
Echocardiography Findings (Gold Standard — ~100% Diagnostic)
2D / Morphological Findings
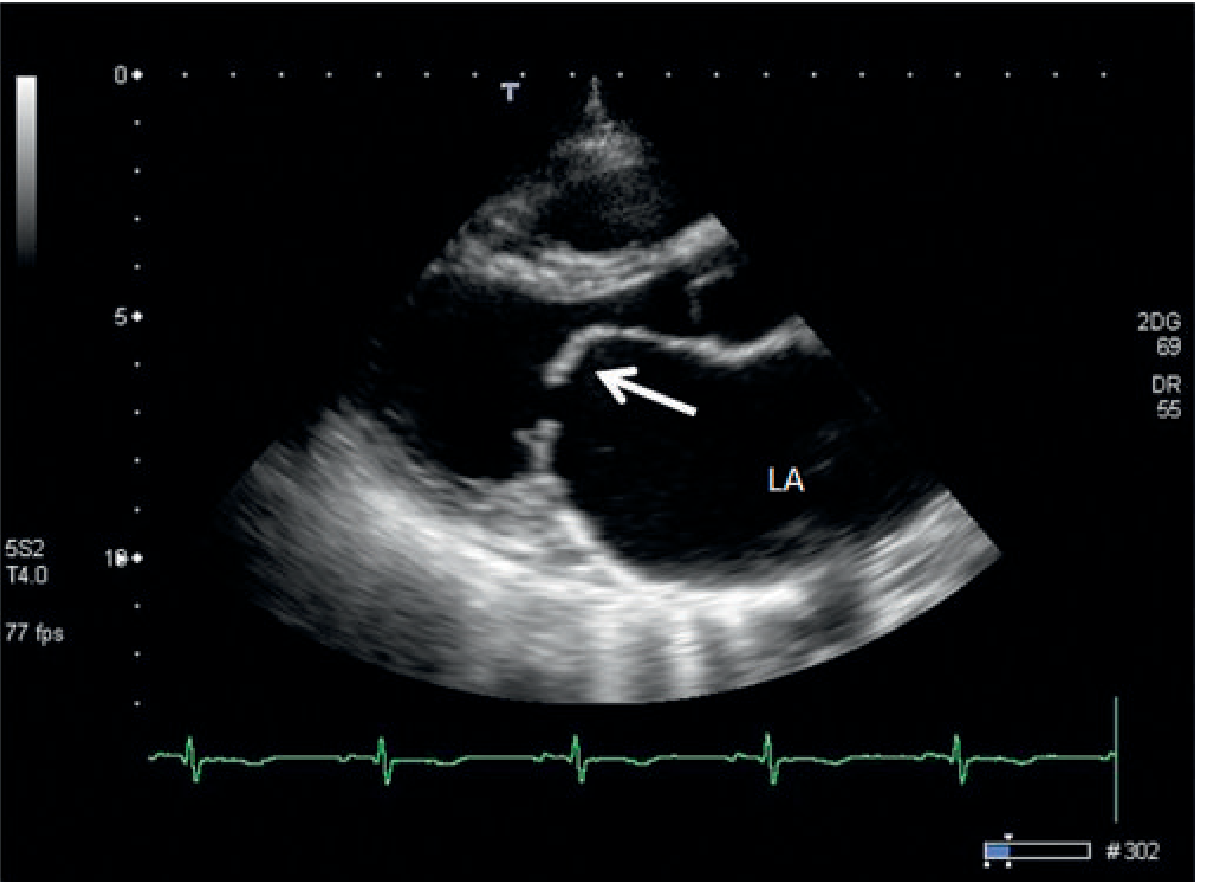
| Feature | Finding |
|---|---|
| Leaflet morphology | Thickening, calcification, nodularity |
| Hockey stick deformity | Anterior mitral leaflet bows anteriorly in diastole (posterior leaflet pulled back) — rheumatic |
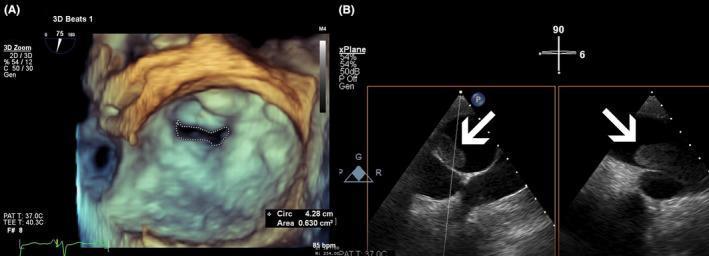
| Fish-mouth / buttonhole appearance | Commissural fusion on short-axis view |
| Commissures | Fusion (anterolateral and/or posteromedial) |
| Chordae tendineae | Thickening, shortening, fusion |
| LA enlargement | Chronic pressure overload |
| LA thrombus | Most commonly in LA appendage; look with TEE |
| LV | Usually normal size and function; reduced in ~1/3 due to ↓ preload |
| RV | Dilated + hypertrophied with pulmonary hypertension |
Doppler Findings
| Measurement | Severe MS |
|---|---|
| Mean transmitral gradient | ≥10 mmHg |
| Mitral valve area (MVA) — pressure half-time | MVA = 220 / T½ (T½ = time for gradient to fall by 50%) |
| Severe MVA | < 1.0 cm² |
| Moderate MVA | 1.0–1.5 cm² |
| Mild MVA | > 1.5 cm² |
| Peak E-wave velocity | Elevated (>1.5 m/s in significant MS) |
| E-wave deceleration | Prolonged (slow filling) |
| TR jet velocity | Elevated if pulmonary hypertension |
Grading by Severity
| Grade | MVA (cm²) | Mean Gradient (mmHg) |
|---|---|---|
| Mild | > 1.5 | < 5 |
| Moderate | 1.0–1.5 | 5–10 |
| Severe | < 1.0 | > 10 |
3D Echo Findings
Cardiac Catheterisation Findings
- Elevated LA / PCWP with persistent LA–LV diastolic gradient
- Gorlin formula to calculate MVA from simultaneously measured pressures and cardiac output
- Used when echo is inconclusive or when coronary anatomy must be assessed pre-operatively
Cardiac MRI Findings
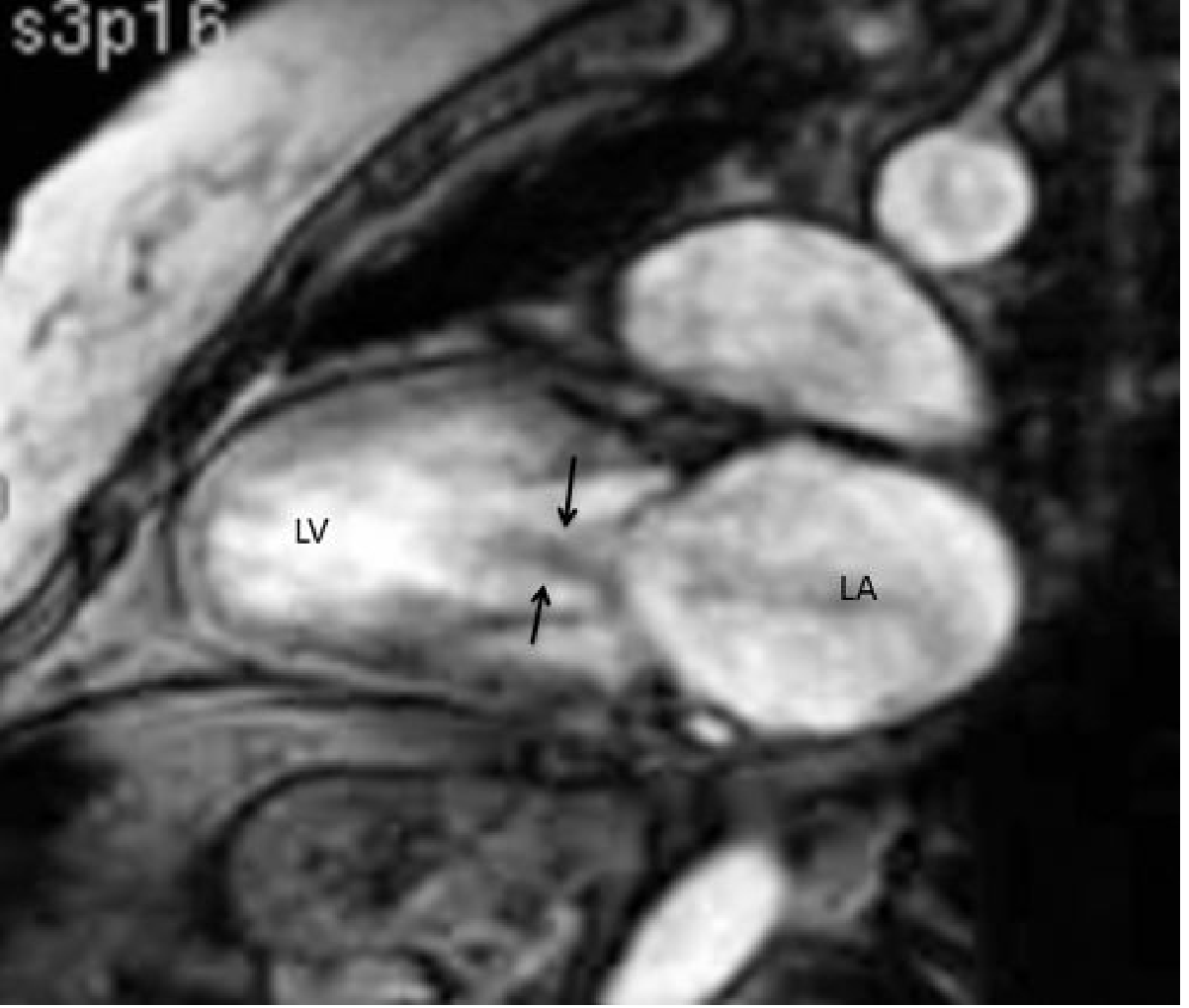
- Flow void / turbulent jet across stenotic valve on cine imaging
- Direct planimetry of valve orifice
- LA enlargement clearly demonstrated
- Velocity-encoded MRI allows pressure half-time calculation of MVA
Complications
| Complication | Notes |
|---|---|
| Atrial fibrillation | Most common arrhythmia; precipitates acute decompensation |
| Systemic thromboembolism / stroke | LA thrombus; most dreaded complication |
| Pulmonary hypertension | Secondary, initially reactive (reversible); later fixed |
| RV failure | Late complication of severe pulmonary hypertension |
| Infective endocarditis | Risk higher in non-calcified, mobile leaflets |
| Ortner syndrome | Hoarseness from giant LA compressing LRLN |
| Haemoptysis | Bronchial vein rupture |
Management Overview
| Scenario | Management |
|---|---|
| Asymptomatic, sinus rhythm | No therapy needed; serial monitoring |
| Mild dyspnoea | Diuretics |
| AF with MS | Rate control (β-blocker, diltiazem, digoxin); warfarin (INR 2.5–3.5) — NOACs are NOT recommended for rheumatic MS with AF |
| Severe symptomatic MS, suitable anatomy | Percutaneous balloon mitral commissurotomy (PBMC/PTMC) — suitable if pliable, non-calcified valve, no significant MR, no LA thrombus |
| Unsuitable for PBMC | Open surgical commissurotomy or mitral valve replacement |
| MAC-related MS | Surgical debridement + MVR (PBMC not effective) |
| Pulmonary HTN ≥50 mmHg | Indication for mechanical intervention |
Wilkins Echo Score (leaflet mobility, thickening, calcification, subvalvular fusion — each 0–4, total 0–16): score ≤8 predicts good outcome with balloon commissurotomy.
Sources: Goldman-Cecil Medicine 26e, Ch. 60; Braunwald's Heart Disease 12e; Grainger & Allison's Diagnostic Radiology; Textbook of Clinical Echocardiography
This is a shared conversation. Sign in to Orris to start your own chat.