temporal swelling in MRI with a history of headache, chronic lacrimation, and fever since two days.
giant cell arteritis temporal artery MRI imaging
Temporal Swelling on MRI + Headache + Chronic Lacrimation + Fever (2 days)
🔴 Primary Diagnosis: Giant Cell Arteritis (Temporal Arteritis)
Clinical Features
- Granulomatous inflammation of large and medium-sized arteries (especially temporal branches of the external carotid)
- Almost exclusively in patients >55 years (rarely younger)
- Dull, unilateral temporal headache with a thick, tortuous, tender temporal artery on palpation
- Low-grade fever, malaise, fatigue, anorexia
- Jaw claudication (ischemia of masseter muscles)
- Scalp tenderness, occasionally ear pain
- Risk of anterior ischemic optic neuropathy → sudden vision loss (most feared complication; second eye involved in 65% of untreated patients within 10 days)
- Chronic lacrimation can occur from periorbital/ocular inflammation
MRI Findings in GCA
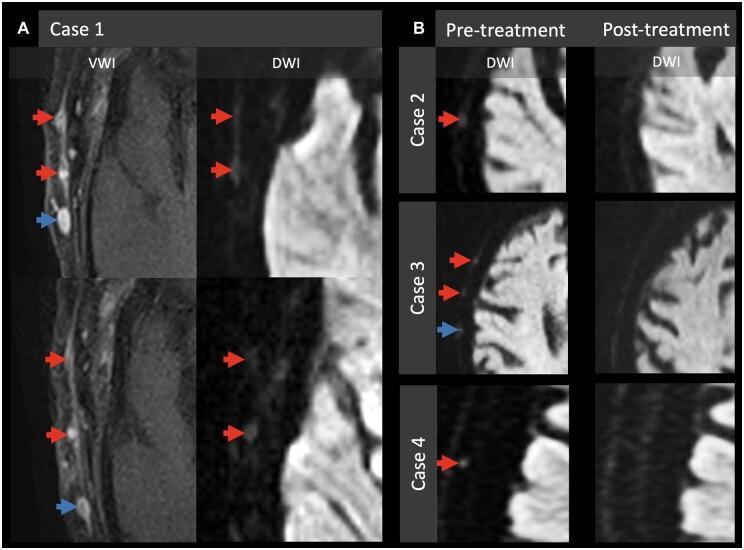
- Vessel Wall Imaging (VWI): Concentric wall thickening + mural enhancement of the superficial temporal artery (STA)
- DWI: Hyperintense "dots" along the scalp corresponding to inflamed STA segments with restricted diffusion — these resolve post-corticosteroid treatment
- CE-T1 fat-sat: Circumferential mural enhancement of the temporal artery (the key sign)
- STIR: High-signal edema in the anterior and lateral extracranial soft tissues — the "multifocal arcuate sign"
Workup
| Test | Finding in GCA |
|---|---|
| ESR (Westergren) | Typically >80 mm/hr, sometimes >120 mm/hr |
| CRP | Markedly elevated |
| CBC | Normochromic anemia, thrombocytosis |
| Temporal artery biopsy | Gold standard — skip-lesion granulomatous inflammation |
| High-resolution MRI / Ultrasound | Halo sign, mural thickening |
ESR >30 mm/hr in men >60y and >35 mm/hr in women >60y is abnormal. Normal ESR does not exclude GCA (occurs in a minority of cases).
Treatment
- Do not delay steroids for biopsy — start immediately on clinical suspicion
- Prednisone 1.0–1.5 mg/kg/day (up to 100 mg) orally; IV methylprednisolone if visual symptoms present
- Biopsy remains positive for up to 1 week after starting steroids
- Taper guided by symptoms + ESR/CRP over months to years
- Tocilizumab (IL-6 receptor inhibitor) allows steroid-sparing remission in refractory/relapsing cases
— Textbook of Family Medicine 9e, p. 374 | Adams and Victor's Principles of Neurology, 12th Ed, p. 872
🟡 Important Differential: Cluster Headache / Trigeminal Autonomic Cephalalgia (TAC)
Cluster Headache Features
- Severe unilateral orbital, supraorbital, or temporal pain lasting 15–180 minutes
- Ipsilateral autonomic features: lacrimation, conjunctival injection, nasal congestion, eyelid edema, miosis, ptosis, facial sweating
- Attacks 1–8×/day, often precipitated by alcohol/histamine/nitroglycerin
- Seasonal/circadian periodicity
- Hypothalamic (inferior posterior) activation on functional MRI
- MRI indicated at first presentation to exclude secondary causes (infection, vascular malformation, carotid dissection, pituitary tumor)
TAC Comparison Table
| Feature | Cluster | Paroxysmal Hemicrania | SUNCT |
|---|---|---|---|
| Sex | M >> F (3–7:1) | F > M (2:1) | M > F |
| Attack duration | 15–180 min | 2–30 min | 5–240 sec |
| Frequency | 1–8/day | Up to 40/day | 3–200/day |
| Indomethacin response | No | Complete (pathognomonic) | No |
| Acute Rx | O₂, sumatriptan SQ | None (indomethacin preventive) | Lamotrigine |
| Prevention | Verapamil, lithium, steroids, galcanezumab | Indomethacin | Lamotrigine, topiramate |
— Goldman-Cecil Medicine, p. 381
Other Differentials to Consider
| Condition | Key Distinguishing Features |
|---|---|
| Intracranial granulomatous arteritis (isolated CNS) | Normal/mildly elevated ESR, MRI shows white matter changes, brain biopsy needed |
| Temporomandibular joint (TMJ) disease | No fever, no lacrimation; jaw movement-related |
| Temporal fossa abscess/cellulitis | Focal erythema, warmth, purulent focus; CT/MRI shows fluid collection |
| Sinusitis (sphenoid/ethmoid) | Nasal symptoms, sinus opacification on MRI |
| Meningitis/encephalitis | Meningism, altered consciousness, CSF pleocytosis |
| Orbital pseudotumor / Tolosa-Hunt syndrome | Painful ophthalmoplegia, periorbital enhancement on MRI |
Clinical Approach Summary
History + Exam
│
├─ Age >55 + tender temporal artery + elevated ESR/CRP
│ └─ → GCA: Start steroids IMMEDIATELY → Temporal artery biopsy within 1 week
│
├─ Younger patient + episodic attacks + autonomic features
│ └─ → TAC/Cluster headache: MRI to exclude secondary cause → Verapamil prophylaxis
│
└─ Fever + focal soft tissue swelling + erythema
└─ → Infectious: CT/MRI with contrast for abscess → Antibiotics
not chronic lacrimation, Seizures tonic clonic
Temporal Swelling on MRI + Headache + Tonic-Clonic Seizures + Fever (2 days)
🔴 #1 Diagnosis: Herpes Simplex Encephalitis (HSE)
Pathology
- Caused by HSV-1 in >90% of adult cases
- Arises from reactivation of latent HSV in the trigeminal ganglion, reaching the brain via trigeminal tracts or olfactory nerves
- Pathological hallmark: hemorrhagic necrotizing encephalitis with a striking predilection for the medial temporal lobe, insula, cingulate gyrus, and inferior frontal lobe
- Cowdry type A intranuclear inclusion bodies in neurons and glial cells
- Perivascular lymphocytic infiltration, microglial nodules, focal cortical necrosis
Clinical Features (All Present in This Case)
| Feature | Present? |
|---|---|
| Acute fever | ✅ |
| Headache | ✅ |
| Seizures (tonic-clonic) | ✅ |
| Temporal lobe involvement on MRI | ✅ |
| Behavioral/personality change, agitation | Often early |
| Aphasia (dominant hemisphere) | If left temporal |
| Olfactory/gustatory hallucinations | Highly characteristic |
| Altered consciousness → stupor → coma | Late, if untreated |
"Clinically, herpes simplex encephalitis begins with the acute onset of a confusional state, aphasia, or behavioral changes, often accompanied by headache, fever, and seizures… behavioral disturbances or agitated delirium, particularly with olfactory or gustatory hallucinations, precedes coma by hours or days — a pattern so characteristic as to suggest the diagnosis." — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
MRI Findings in HSE
| Sequence | Finding |
|---|---|
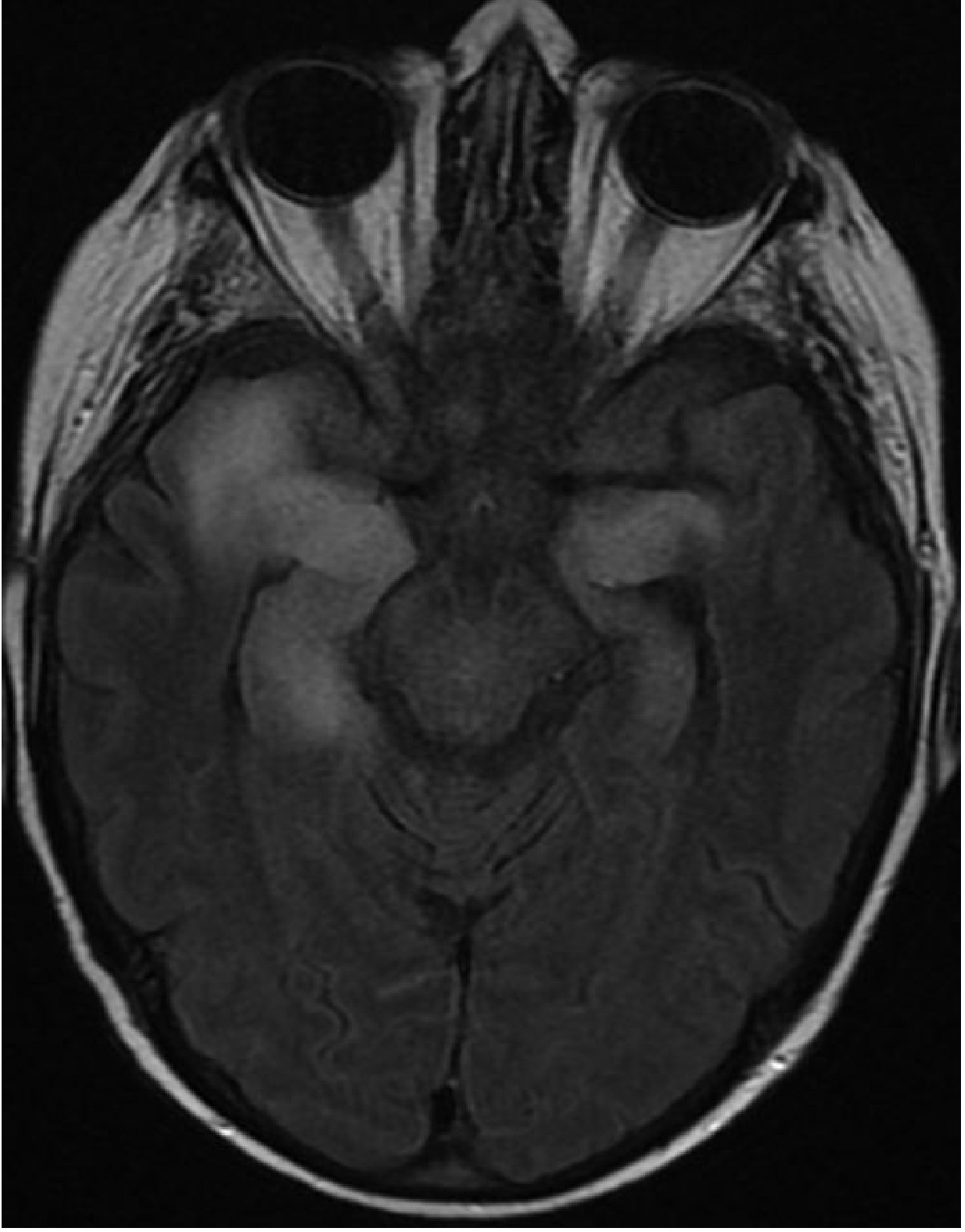
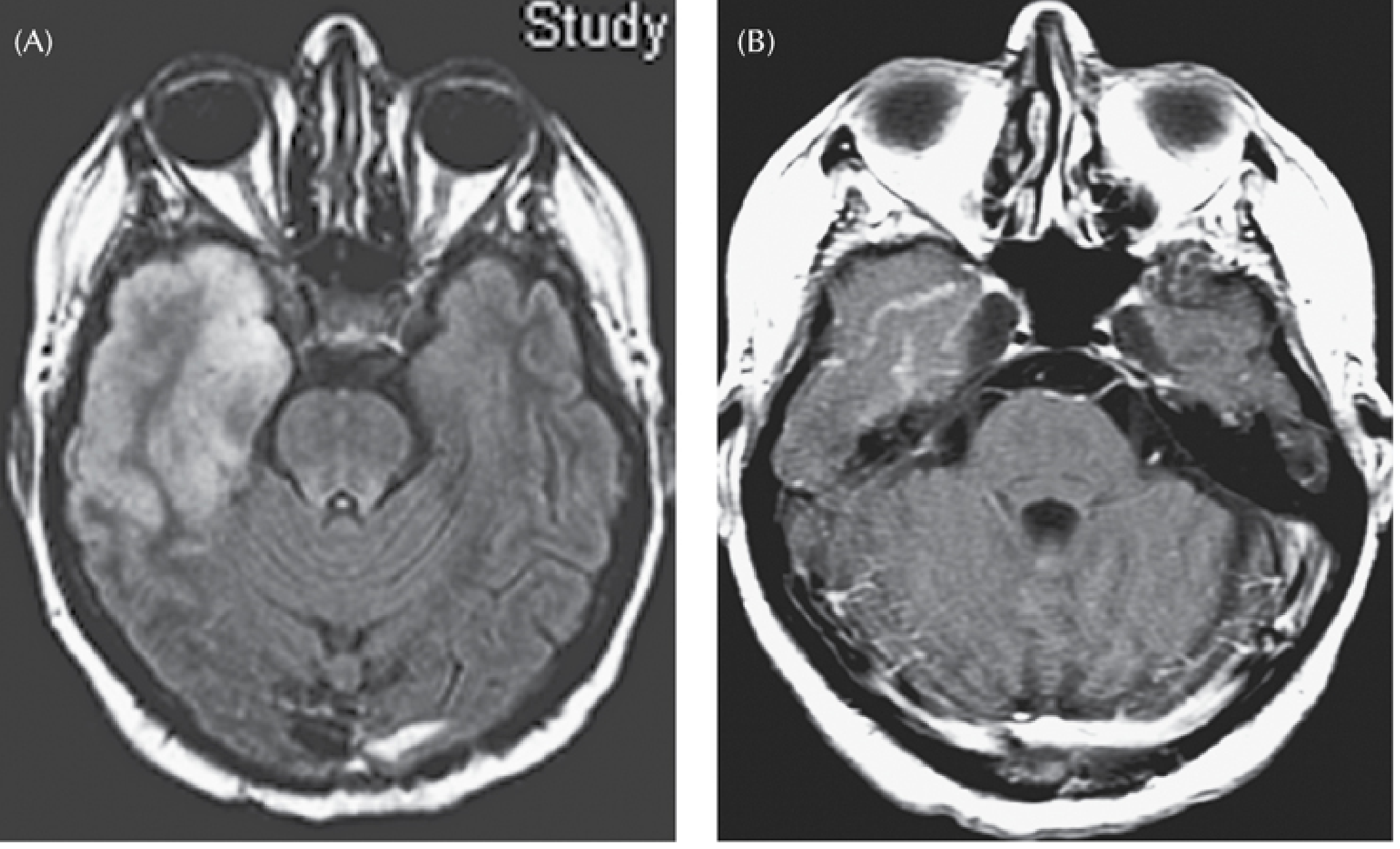
| FLAIR / T2 | High signal + cortical swelling in anteromedial temporal lobe, insula, cingulate — earliest and most sensitive; abnormal within 2 days |
| DWI | Cortical hyperintensity with restricted diffusion — even more sensitive than conventional MRI |
| CE-T1 | Patchy or gyriform enhancement in affected cortex (develops later) |
| T2*/SWI | Foci of microhemorrhage (late feature; reflects hemorrhagic necrosis) |
| CT (less sensitive) | Low attenuation + swelling in anteromedial temporal lobe; may appear normal for 3–5 days |
Abnormalities start unilaterally but frequently spread to the contralateral temporal lobe. Bilateral involvement on MRI is a poor prognostic sign.
Diagnostic Workup
- MRI brain with FLAIR, DWI, CE-T1, SWI — temporal lobe swelling/hyperintensity
- CSF analysis (LP — after imaging to exclude mass effect):
- Lymphocytic pleocytosis: 25–75 WBC/μL (mononuclear predominance)
- Protein mildly elevated (65–85 mg/dL)
- Glucose usually normal
- RBCs (up to 500/μL) from hemorrhagic necrosis
- CSF HSV PCR — gold standard; sensitivity >95%, specificity ~100%
- EEG — always abnormal; periodic lateralized epileptiform discharges (PLEDs) arising from one or both temporal lobes at ~1 Hz are highly characteristic and correlate with poor prognosis
- Functional imaging — hyperperfusion in the temporal lobe
⚠️ Do NOT delay LP for PCR if CT/MRI shows no herniation risk — but start acyclovir immediately regardless.
Treatment
| Drug | Dose | Duration |
|---|---|---|
| IV Acyclovir | 10 mg/kg every 8 hours | 14–21 days |
| Anti-epileptics | Levetiracetam, phenytoin | For seizure control |
- Mortality >70%
- <10% return to normal neurological function
- Mortality reduced to 10–25%
- 40–55% resume activities of daily living
- Best outcomes when started before coma — do not wait for PCR confirmation
"Early treatment of herpes simplex encephalitis is vital as treatment with acyclovir yields the best results when administered before patients become comatose. Most patients with suspected herpes encephalitis are now treated immediately, with the drug discontinued later if the diagnosis is not confirmed." — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Differential Diagnoses
🟡 Brain Abscess
- Headache + fever + seizures + focal mass on MRI — but MRI shows a ring-enhancing lesion with central restricted diffusion (DWI bright, ADC dark) rather than diffuse cortical swelling
- Look for a source: otitis media (temporal lobe abscess is classically from otogenic origin), sinusitis, dental infection, endocarditis
- LP contraindicated (risk of herniation/rupture)
- Management: CT-guided aspiration + vancomycin + metronidazole + cefotaxime ≥6–8 weeks
🟡 Bacterial Meningitis with Cortical Involvement
- High fever, meningism (neck stiffness, Kernig's, Brudzinski's), photophobia
- MRI shows leptomeningeal enhancement rather than temporal parenchymal swelling
- CSF: neutrophilic pleocytosis, low glucose, high protein
🟡 Autoimmune/Limbic Encephalitis (Anti-NMDAR, LGI1, etc.)
- Can mimic HSE on MRI — medial temporal T2/FLAIR signal
- Key differentiator: subacute/slower onset (weeks not days), prominent psychiatric features, less fever
- Triggered by relapsing symptoms after initial HSV encephalitis (post-HSE autoimmune encephalitis)
- Workup: serum and CSF autoantibody panel
🟡 Subdural Empyema
- Rapid-onset fever, seizures, focal deficits
- MRI: crescent-shaped extra-axial collection with DWI restriction and rim enhancement
- Neurosurgical emergency
🟠 Temporal Lobe Tumor (Glioma/Metastasis)
- No fever typically; slower progression
- Ring-enhancing mass with surrounding edema; no CSF pleocytosis
Immediate Management Algorithm
Temporal swelling MRI + Headache + Seizures + Fever
│
├─ STAT CT/MRI brain → if no herniation:
│ └─ Lumbar puncture → CSF for cell count, glucose, protein, HSV PCR, culture
│
├─ START IV Acyclovir 10 mg/kg q8h IMMEDIATELY (do not wait for PCR result)
│
├─ Anti-epileptic therapy (levetiracetam IV if actively seizing)
│
├─ If bacterial meningitis also suspected → add empirical antibiotics
│ (ceftriaxone 2g q12h + dexamethasone)
│
└─ EEG monitoring — look for PLEDs from temporal lobe
— Goldman-Cecil Medicine International Edition | Adams and Victor's Principles of Neurology 12e | Grainger & Allison's Diagnostic Radiology | Plum and Posner's Diagnosis and Treatment of Stupor and Coma
in CNS infection usmkle step 1 is mostly focusing on n HSV 1 encephalitis, like wise HIV realted dementia, sypilis , prions dieases and tuberculous based questionns i will first add and paste them individually but i want a small compressed notes like mehlman to rule out this questions and break down reasily.
🧠 CNS Infections — USMLE Step 1 Rapid Crush Sheet
1️⃣ HSV-1 Encephalitis
- Fever + headache + temporal lobe involvement
- Behavioral change / personality change (medial temporal/limbic)
- Olfactory or gustatory hallucinations ← most specific clue
- Tonic-clonic seizures
- Rapidly progressive → stupor/coma
- Hemorrhagic necrotizing encephalitis
- Medial temporal lobe + insula + cingulate (limbic predilection)
- Cowdry type A inclusion bodies (intranuclear, in neurons + glia)
- Perivascular lymphocytes, microglial nodules
- T2/FLAIR: high signal + swelling in anteromedial temporal lobe (starts unilateral → bilateral)
- DWI: cortical restricted diffusion (most sensitive early)
- CE-T1: gyriform enhancement (late)
- SWI: microhemorrhage (late, hemorrhagic stage)
- Lymphocytic pleocytosis + ↑ protein + normal glucose + RBCs
- HSV PCR → gold standard (sensitivity >95%)
- Periodic lateralized epileptiform discharges (PLEDs) at ~1 Hz from temporal lobe ← pathognomonic pattern
- IV Acyclovir 10 mg/kg q8h × 14–21 days — start IMMEDIATELY, don't wait for PCR
- Without Rx: mortality >70%; with Rx: mortality 10–25%
2️⃣ HIV-Associated Dementia (HAND / AIDS Dementia Complex)
- Subcortical dementia pattern: psychomotor slowing, forgetfulness, poor concentration
- Gait disorder, leg weakness (vacuolar myelopathy)
- No fever (unless superinfection)
- NOT aphasia/apraxia (those are cortical → think Alzheimer)
- Multinucleated giant cells (HIV-infected macrophages fusing) ← Step 1 favorite
- Microglial nodules
- Perivascular foamy macrophages + lymphocytic infiltrates
- Diffuse white matter pallor/rarefaction (myelin breakdown)
- Direct HIV infection of microglia/macrophages (not neurons directly)
- Diffuse white matter T2/FLAIR hyperintensity (ill-defined, bilateral, symmetric)
- Cortical atrophy + ventriculomegaly (sulcal widening)
- No ring-enhancing lesion (that's toxo/lymphoma)
- Mild ↑ protein; mild lymphocytosis or normal; HIV detectable in CSF
- HAART (antiretrovirals) — only effective treatment; reverses cognitive decline if started early
Differentiator from Toxo/PML/CNS Lymphoma:
HIV Dementia Toxoplasmosis PML CNS Lymphoma Lesion Diffuse WM Ring-enhancing WM (no enhancement) Periventricular, enhancing CD4 <200 <100 <50–100 <50 Fever No Yes No No Organism HIV T. gondii JC virus EBV-driven
3️⃣ Neurosyphilis (Treponema pallidum)
| Stage | Onset after infection | Syndrome | Key Features |
|---|---|---|---|
| Meningeal | 2 years | Aseptic meningitis | Fever, headache, stiff neck, CN palsies (VIII → deafness, VII → facial weakness), seizures |
| Meningovascular | 5–12 years | Stroke-like | Hemiplegia, aphasia → thrombosis of CNS vessels; Argyll Robertson pupil |
| Tabes Dorsalis | 10–25 years | Dorsal column/dorsal root degeneration | Lightning/lancinating pains, Argyll Robertson pupils, Romberg+, loss of proprioception + vibration, areflexia, Charcot joints, painless ulcers |
| General Paresis | 10–25 years | Cortical dementia | Personality change → grandiosity → megalomania → dementia |
- Accommodates but does NOT react to light
- Bilateral, irregular, small pupils
- Mnemonic: "Prostitute's pupil — accommodates but won't react"
- VDRL in CSF = specific (positive = neurosyphilis confirmed), but not sensitive
- FTA-ABS in CSF = sensitive (negative = rules out)
- Lymphocytic pleocytosis + ↑ protein
- Aqueous crystalline penicillin G IV × 10–14 days (benzathine penicillin does NOT reach treponemicidal CSF levels)
4️⃣ Prion Disease (CJD — Creutzfeldt-Jakob Disease)
| Type | Cause | Notes |
|---|---|---|
| Sporadic CJD | Spontaneous PrP^c → PrP^sc | >90% of cases; age ~60 |
| Familial CJD | PRNP gene mutation | Autosomal dominant |
| Variant CJD (vCJD) | Eating BSE-infected beef ("mad cow") | Younger patients; psychiatric onset first |
| Iatrogenic | Contaminated instruments/dura/cornea transplant | |
| Kuru | Ritual cannibalism (Fore tribe, PNG) | Cerebellar ataxia > dementia |
- Rapidly progressive dementia (weeks–months, not years)
- Myoclonus (startle myoclonus)
- Ataxia, visual disturbances
- Death within 1 year (median ~4 months sporadic CJD)
- No fever (not infectious in usual sense)
- Spongiform change — cytoplasmic vacuoles in neurons + glia ← Step 1 loves this
- Kuru plaques (PrP^sc deposits)
- Neuronal loss + reactive astrocytosis
- No inflammation (distinguishes from encephalitis)
- MRI: cortical ribboning on DWI (restricted diffusion basal ganglia/cortex) ← most sensitive
- EEG: periodic sharp wave complexes (1 Hz, triphasic)
- CSF: 14-3-3 protein (marker of rapid neuronal death; not specific)
- Brain biopsy: spongiform change + PrP^sc immunostaining after proteinase K digestion ← gold standard
vCJD tip: Younger patient + psychiatric symptoms first + florid PrP plaques (surrounded by spongiform change like a "daisy") + tonsil biopsy positive
5️⃣ Tuberculous Meningitis
- Subacute onset (weeks, not days like bacterial)
- Fever + headache + meningism
- Cranial nerve palsies (III, VI, VII — basilar involvement) ← most specific
- Hydrocephalus (communicating → basilar exudate obstructs CSF)
- Tuberculoma = focal granuloma (ring-enhancing on MRI)
- Basilar exudate (thick, gelatinous material at base of brain) ← #1 Step 1 clue
- Granulomas with Langhans giant cells, central caseous necrosis, epithelioid macrophages
- Vasculitis → stroke
- Hydrocephalus
- Basilar meningeal enhancement (post-contrast T1) ← hallmark
- Communicating hydrocephalus
- Ring-enhancing tuberculoma
- Infarcts (vasculitis)
- Lymphocytic pleocytosis (100–500 cells)
- ↑↑ Protein (100–500 mg/dL)
- ↓ Glucose (very low — <45 mg/dL, CSF:serum ratio <0.5)
- AFB smear (low sensitivity ~10–40%); culture (weeks); PCR (faster)
- Adenosine deaminase (ADA) elevated in CSF
- RIPE × 2 months → RI × 7–10 months (longer than pulmonary TB)
- Add dexamethasone (reduces mortality, prevents vasculitis complications)
- Treat hydrocephalus with shunt if needed
⚡ MASTER COMPARISON TABLE
| Feature | HSV Encephalitis | HIV Dementia | Neurosyphilis | CJD | TB Meningitis |
|---|---|---|---|---|---|
| Onset | Acute (days) | Subacute/chronic | Variable (years) | Subacute (weeks–months) | Subacute (weeks) |
| Fever | ✅ High | ❌ (no active infxn) | ✅ Early | ❌ | ✅ Low-grade |
| Seizures | ✅ Common | Late | ✅ Early syphilis | ✅ (myoclonus) | ✅ |
| Dementia | Acute delirium | Subcortical progressive | Late (general paresis) | Rapidly progressive | Possible |
| Key path finding | Cowdry A bodies; hemorrhagic necrosis | Multinucleated giant cells | Dorsal column degeneration (tabes); meningovascular | Spongiform vacuoles; kuru plaques | Basilar granulomatous exudate |
| MRI hallmark | Temporal T2/FLAIR swelling | Diffuse WM T2, atrophy | Meningeal enhancement; infarcts | DWI cortical ribboning | Basilar enhancement; hydrocephalus |
| CSF glucose | Normal | Normal | Low-normal | Normal | ↓↓ Very low |
| CSF cells | Lymphocytes + RBCs | Mild lymphocytosis | Lymphocytes | Normal/mild ↑ | Lymphocytes |
| Key CSF test | HSV PCR | HIV viral load | VDRL (specific) | 14-3-3 protein | AFB culture/PCR, ADA |
| EEG finding | PLEDs (temporal, 1 Hz) | Non-specific slowing | Normal | Periodic sharp waves | Non-specific |
| Treatment | IV Acyclovir | HAART | Penicillin G IV | None (fatal) | RIPE + Dex |
🎯 High-Yield Step 1 Trigger Phrases
| If you see this... | Think... |
|---|---|
| Temporal lobe + hemorrhagic necrosis + olfactory hallucinations | HSV-1 |
| Multinucleated giant cells + WM changes + AIDS | HIV dementia |
| Accommodates but doesn't react to light | Argyll Robertson = Syphilis |
| Lightning pains + ataxia + areflexia + old syphilis | Tabes dorsalis |
| Rapidly progressive dementia + myoclonus + spongiform vacuoles | CJD/Prion |
| Subacute meningitis + basilar CN palsies + very low CSF glucose | TB meningitis |
| Ring-enhancing lesion + CD4 <100 + immunocompromised | Toxoplasmosis (≠ HIV dementia) |
| WM demyelination + no enhancement + CD4 <50 + JC virus | PML |
| EBV + periventricular enhancing mass + AIDS | CNS lymphoma |
mater comparison table pattern i ddint like make for nice ansd should fit inn a4 paper
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
~/cns-table/make_table.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm
from reportlab.platypus import SimpleDocTemplate, Table, TableStyle, Paragraph, Spacer
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT
from reportlab.platypus import HRFlowable
OUTPUT = "/home/daytona/workspace/cns-table/CNS_Infections_Step1.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=1.0*cm,
rightMargin=1.0*cm,
topMargin=1.2*cm,
bottomMargin=1.0*cm,
)
W, H = A4
styles = getSampleStyleSheet()
# ── colour palette ──────────────────────────────────────────────
C_NAVY = colors.HexColor("#0D1B2A")
C_BLUE = colors.HexColor("#1B4F8A")
C_LBLUE = colors.HexColor("#2E86AB")
C_MINT = colors.HexColor("#D4EAF7")
C_ALTROW = colors.HexColor("#EEF5FB")
C_WHITE = colors.white
C_RED = colors.HexColor("#C0392B")
C_GREEN = colors.HexColor("#1A7A4A")
C_GOLD = colors.HexColor("#F4A300")
C_GRAY = colors.HexColor("#F5F5F5")
C_BORDER = colors.HexColor("#A8C8E8")
# ── styles ───────────────────────────────────────────────────────
title_style = ParagraphStyle("title", fontSize=13, fontName="Helvetica-Bold",
textColor=C_WHITE, alignment=TA_CENTER, spaceAfter=0, spaceBefore=0, leading=16)
sub_style = ParagraphStyle("sub", fontSize=7.5, fontName="Helvetica",
textColor=C_WHITE, alignment=TA_CENTER, spaceAfter=0, spaceBefore=0, leading=10)
hdr_style = ParagraphStyle("hdr", fontSize=7, fontName="Helvetica-Bold",
textColor=C_WHITE, alignment=TA_CENTER, leading=9, spaceAfter=0)
row_label = ParagraphStyle("rl", fontSize=6.8, fontName="Helvetica-Bold",
textColor=C_NAVY, alignment=TA_LEFT, leading=8.5)
cell_style = ParagraphStyle("cell", fontSize=6.3, fontName="Helvetica",
textColor=C_NAVY, alignment=TA_LEFT, leading=8, spaceAfter=0)
cell_red = ParagraphStyle("cr", parent=cell_style, textColor=C_RED, fontName="Helvetica-Bold")
cell_grn = ParagraphStyle("cg", parent=cell_style, textColor=C_GREEN, fontName="Helvetica-Bold")
trigger_title = ParagraphStyle("tt", fontSize=7.5, fontName="Helvetica-Bold",
textColor=C_WHITE, alignment=TA_CENTER)
trigger_key = ParagraphStyle("tk", fontSize=6.5, fontName="Helvetica-Bold",
textColor=C_NAVY, leading=8.5)
trigger_val = ParagraphStyle("tv", fontSize=6.5, fontName="Helvetica",
textColor=C_NAVY, leading=8.5)
def P(text, s=cell_style): return Paragraph(text, s)
def B(text): return Paragraph(text, cell_red)
def G(text): return Paragraph(text, cell_grn)
# ═══════════════════════════════════════════════════════════════
# MAIN TABLE DATA
# ═══════════════════════════════════════════════════════════════
col_headers = [
P("", hdr_style),
P("HSV-1\nEncephalitis", hdr_style),
P("HIV\nDementia", hdr_style),
P("Neuro-\nsyphilis", hdr_style),
P("CJD\n(Prion)", hdr_style),
P("TB\nMeningitis", hdr_style),
]
rows = [
# label, HSV, HIV, Syphilis, CJD, TB
("Onset",
"Acute\n(hours–days)",
"Subacute/chronic\n(months)",
"Variable\n(years by stage)",
"Subacute\n(weeks–months)",
"Subacute\n(weeks)"),
("Fever",
"✔ High",
"✘ Absent",
"✔ Early stage",
"✘ Absent",
"✔ Low-grade"),
("Seizures",
"✔ Common\n(tonic-clonic)",
"Late only",
"✔ Early syphilis",
"✔ Myoclonus\n(startle)",
"✔ Yes"),
("Dementia\nType",
"Acute delirium\n(limbic)",
"Subcortical\n(slow, forgetful)",
"General Paresis\n(late, grandiose)",
"Rapidly progressive\n(weeks→death)",
"Possible late"),
("Hallmark\nSymptom",
"Olfactory/gustatory\nhallucinations",
"Psychomotor\nslowing",
"Argyll Robertson\npupil",
"Myoclonus\n+ startle",
"Cranial nerve\npalsies (III, VI)"),
("Key\nPathology",
"Cowdry A bodies\nHemorrhagic necrosis\nMedial temporal",
"Multinucleated\ngiant cells\nMicroglial nodules",
"Tabes: dorsal column\ndegeneration\nGeneral paresis: cortex",
"Spongiform\nvacuoles\nKuru plaques",
"Basilar granuloma-\ntous exudate\nLanghans giant cells"),
("MRI\nHallmark",
"T2/FLAIR: temporal\nswelling & high signal\nDWI: cortical restrict.",
"Diffuse WM T2\nhyperintensity\nAtrophy + ventricles↑",
"Meningeal enhance.\nInfarcts (meningovasc)\nNormal (tabes)",
"DWI: cortical\nribboning\nBasal ganglia restrict.",
"Basilar meningeal\nenhancement\nHydrocephalus"),
("CSF\nGlucose",
"Normal",
"Normal",
"Low-normal",
"Normal",
"↓↓ Very low\n(<45 mg/dL)"),
("CSF\nCells",
"Lymphocytes\n+ RBCs",
"Mild lymphocytosis\nor normal",
"Lymphocytes",
"Normal or\nmild ↑",
"Lymphocytes\n(100–500/μL)"),
("Gold-Standard\nCSF Test",
"HSV PCR\n(sens >95%)",
"HIV viral load\nin CSF",
"VDRL (specific)\nFTA-ABS (sensitive)",
"14-3-3 protein\n+ RT-QuIC",
"AFB culture\nPCR / ADA↑"),
("EEG\nFinding",
"PLEDs 1 Hz\ntemporal lobe",
"Non-specific\nslowing",
"Normal",
"Periodic sharp\nwave complexes",
"Non-specific"),
("Treatment",
"IV Acyclovir\n10 mg/kg q8h\n×14–21 days",
"HAART\n(antiretrovirals)",
"Penicillin G IV\n×10–14 days\n(NOT benzathine)",
"None\n(always fatal)",
"RIPE ×2 mo\n→RI ×7–10 mo\n+ Dexamethasone"),
]
# Build table data
table_data = [col_headers]
for i, row in enumerate(rows):
label_para = P(row[0], row_label)
cells = [label_para] + [P(row[j+1]) for j in range(5)]
table_data.append(cells)
# Column widths — label col wider, 5 disease cols equal
avail_w = W - 2.0*cm
label_w = 2.0*cm
disease_w = (avail_w - label_w) / 5
col_widths = [label_w] + [disease_w]*5
# Row heights
row_heights = [1.0*cm] + [None]*len(rows)
tbl = Table(table_data, colWidths=col_widths, rowHeights=row_heights, repeatRows=1)
# Alternating row colors
style_cmds = [
# Header row
("BACKGROUND", (0,0), (-1,0), C_BLUE),
("TEXTCOLOR", (0,0), (-1,0), C_WHITE),
("ROWBACKGROUNDS", (0,1), (-1,-1), [C_WHITE, C_ALTROW]),
# Label column
("BACKGROUND", (0,1), (0,-1), C_MINT),
# Grid
("GRID", (0,0), (-1,-1), 0.4, C_BORDER),
("LINEBELOW", (0,0), (-1, 0), 1.2, C_LBLUE),
# Alignment
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("ALIGN", (1,0), (-1,0), "CENTER"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1),3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING",(0,0), (-1,-1), 3),
# Treatment row — highlight
("BACKGROUND", (1, len(rows)), (-1, len(rows)), colors.HexColor("#FFF8E1")),
("LINEABOVE", (0, len(rows)), (-1, len(rows)), 1.0, C_GOLD),
]
tbl.setStyle(TableStyle(style_cmds))
# ═══════════════════════════════════════════════════════════════
# TRIGGER PHRASES TABLE
# ═══════════════════════════════════════════════════════════════
trigger_data_raw = [
("Temporal lobe + hemorrhagic necrosis + olfactory hallucinations", "HSV-1 Encephalitis → IV Acyclovir"),
("Multinucleated giant cells + white matter changes + AIDS", "HIV Dementia → HAART"),
("Accommodates but doesn't react to light (small, irregular pupils)","Argyll Robertson = Neurosyphilis"),
("Lightning pains + ataxia + areflexia + Charcot joints", "Tabes Dorsalis → Pen G IV"),
("Rapidly progressive dementia + myoclonus + spongiform vacuoles", "CJD/Prion → No cure"),
("Subacute meningitis + basilar CN palsies + ↓↓ CSF glucose", "TB Meningitis → RIPE + Dex"),
("Ring-enhancing lesion + CD4 <100", "Toxoplasmosis (≠ HIV dementia)"),
("WM demyelination, no enhancement + JC virus + CD4 <50", "PML (Progressive Multifocal Leukoencephalopathy)"),
("EBV + periventricular enhancing mass + AIDS", "CNS Lymphoma"),
]
trigger_rows = []
for clue, dx in trigger_data_raw:
trigger_rows.append([
P("🔑 " + clue, trigger_key),
P("→ " + dx, trigger_val),
])
trig_col_w = [avail_w * 0.56, avail_w * 0.44]
trig_tbl = Table(trigger_rows, colWidths=trig_col_w)
trig_tbl.setStyle(TableStyle([
("ROWBACKGROUNDS", (0,0), (-1,-1), [C_WHITE, C_GRAY]),
("GRID", (0,0), (-1,-1), 0.3, C_BORDER),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING",(0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
("LEFTPADDING",(0,0), (-1,-1), 5),
("RIGHTPADDING",(0,0),(-1,-1), 4),
("LINEAFTER", (0,0), (0,-1), 1.2, C_LBLUE),
]))
# ═══════════════════════════════════════════════════════════════
# TITLE BANNER
# ═══════════════════════════════════════════════════════════════
banner_data = [[P("🧠 CNS INFECTIONS — USMLE Step 1 Master Sheet", title_style),
P("HSV-1 · HIV Dementia · Neurosyphilis · CJD · TB Meningitis", sub_style)]]
banner = Table(banner_data, colWidths=[avail_w])
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_NAVY),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING",(0,0),(-1,-1), 7),
("LINEBELOW", (0,0), (-1,-1), 2, C_GOLD),
]))
# Trigger section header
trig_hdr_data = [[P("⚡ STEP 1 TRIGGER PHRASES — Clue → Diagnosis", trigger_title)]]
trig_hdr = Table(trig_hdr_data, colWidths=[avail_w])
trig_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), C_LBLUE),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
]))
footer_style = ParagraphStyle("ft", fontSize=6, textColor=colors.HexColor("#888888"),
alignment=TA_CENTER, fontName="Helvetica-Oblique")
footer = Paragraph("Orris AI · CNS Infections Step 1 Rapid Sheet · April 2026", footer_style)
# ═══════════════════════════════════════════════════════════════
# BUILD
# ═══════════════════════════════════════════════════════════════
story = [
banner,
Spacer(1, 0.18*cm),
tbl,
Spacer(1, 0.20*cm),
trig_hdr,
trig_tbl,
Spacer(1, 0.15*cm),
footer,
]
doc.build(story)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/cns-table && python make_table.py
ls -lh /home/daytona/workspace/cns-table/CNS_Infections_Step1.pdf
~/cns-table/make_table.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-table/make_table.py'
~/cns-table/make_table.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-table/make_table.py'
~/cns-table/make_table.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-table/make_table.py'
~/cns-table/make_table.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/cns-table/make_table.py'
cd /home/daytona/workspace/cns-table && python make_table.py && ls -lh CNS_Infections_Step1.pdf
cd /home/daytona/workspace/cns-table && python -c " from pypdf import PdfReader r = PdfReader('CNS_Infections_Step1.pdf') print('Pages:', len(r.pages)) print('Text sample:', r.pages[0].extract_text()[:300]) "
cd /home/daytona/workspace/cns-table && python -c " from pypdf import PdfReader r = PdfReader('CNS_Infections_Step1.pdf') print('Pages:', len(r.pages)) full = r.pages[0].extract_text() print(full) "
CNS Infections Step1
PDF Document · PDF
- Navy/blue header with each disease as a column
- Rows: Onset · Fever · Seizures · Dementia Type · Hallmark Symptom · Key Pathology · MRI Hallmark · CSF Glucose · CSF Cells · Gold-Standard CSF Test · EEG Finding · Treatment
- Treatment row highlighted in gold
- Alternating row shading for easy reading
- 9 clue → diagnosis pairs covering HSV, HIV dementia, Argyll Robertson, Tabes, CJD, TB meningitis, Toxo, PML, CNS Lymphoma
A 23-year-old man with no prior history of seizure is brought to the emergency department after experiencing a generalized tonic-clonic seizure. His roommate says that the patient has had a fever and headache for the past 2 days and that today he was talking nonsensically. The patient works for a fast-food chain and occasionally smokes cigarettes on his breaks. He does not use alcohol or illicit drugs. Temperature is 38.6 C (101.5 F). MRI of the brain shows swelling of the temporal lobes. CSF analysis is most likely to reveal which of the following patterns? Explanation Cerebrospinal fluid analysis Diagnosis Cell count Cell type Glucose Protein Bacterial meningitis ↑↑ Neutrophils ↓ ↑↑ Viral meningitis ↑ Lymphocytes Normal Normal or ↑ Fungal or tuberculous meningitis ↑ Lymphocytes ↓ ↑ Herpes encephalitis ↑ Lymphocytes & erythrocytes Normal ↑ Guillain-Barré syndrome Normal Normal Normal ↑ Herpes simplex virus (HSV) type 1 is the most common cause of sporadic encephalitis. Patients usually present with acute-onset fever, headache, altered mental status, and focal neurologic deficits or seizure. MRI classically shows temporal lobe edema because the virus enters the brain via the olfactory tract and travels to the olfactory cortex (located in the medial temporal lobe). Most patients have a "viral pattern" on cerebrospinal fluid (CSF) analysis with lymphocytic pleocytosis, normal glucose, and normal to slightly elevated protein. Hemorrhagic inflammation of the temporal lobes also usually causes elevated erythrocytes in the CSF. (Choice A) Trauma from inserting the lumbar puncture needle can lead to a "traumatic tap," which is characterized by CSF evidence of normal glucose, elevated protein, and elevated erythrocytes. (Choice B) Bacterial meningitis is usually associated with CSF evidence of low glucose, high protein, and a markedly elevated white blood cell count with a neutrophil predominance. Bacterial meningitis classically causes the triad of fever, neck stiffness, and altered mental state. The presence of temporal lobe swelling on brain imaging makes HSV encephalitis far more likely than bacterial meningitis. (Choice D) Tuberculous or fungal meningitis is often associated with CSF evidence of low glucose, moderately elevated protein, and lymphocytic pleocytosis. Most patients with herpes encephalitis have normal CSF glucose and elevated CSF erythrocytes. In addition, the presence of temporal lobe swelling makes HSV encephalitis more likely than tuberculous or fungal meningitis. (Choice E) Patients with Guillain-Barré syndrome (GBS) often have CSF protein elevations with normal cell counts (albuminocytologic dissociation), which is thought to be due to increased permeability of the blood-nerve-barrier at the level of the nerve root. GBS usually presents with progressive, symmetric ascending muscle weakness, not seizures and fevers. Educational objective: Viral infections of the central nervous system are usually characterized by an elevated white blood cell count with a lymphocytic predominance, normal glucose, and elevated (or normal) protein. Patients with herpes encephalitis also usually have elevated erythrocytes in the cerebrospinal fluid due to hemorrhagic inflammation of the temporal lobes. Herpes encephalitis often presents with acute fever, headache, confusion, focal neurologic deficits, and/or seizure.
Question Breakdown — HSV-1 Encephalitis CSF Pattern
Step 1: Read the Stem for Buzzwords
| Clue in Stem | What It Points To |
|---|---|
| 23 M, no prior seizures | New-onset seizure = pathological cause |
| Fever + headache × 2 days | Infectious/inflammatory CNS process |
| Talking nonsensically | Altered mental status / limbic involvement |
| Temporal lobe swelling on MRI | HSV-1 — this is the pathognomonic clue |
| No alcohol/drugs | Eliminates withdrawal seizure |
Temporal lobe swelling = HSV-1 until proven otherwise. No other common entity has this specific MRI pattern in an acute febrile presentation.
Step 2: Eliminate Wrong Choices Rapidly
| Choice | Pattern | Why Wrong |
|---|---|---|
| A — Traumatic tap | ↑ RBCs, normal WBC, normal glucose | No cells, no inflammation — just blood from needle. No WBC rise. |
| B — Bacterial meningitis | ↑↑ WBC (neutrophils), ↓ glucose, ↑↑ protein | Neutrophilic, glucose LOW. No temporal swelling in bacterial. |
| D — TB / Fungal meningitis | ↑ lymphocytes, ↓ glucose, ↑ protein | Glucose is LOW — key differentiator from HSV. |
| E — Guillain-Barré | Normal cells, ↑ protein | No fever, no seizures, ascending weakness — not this picture at all. |
Step 3: Arrive at the Answer
| Parameter | Finding | Reason |
|---|---|---|
| WBC | ↑ (mild-moderate) | Inflammatory pleocytosis |
| Cell type | Lymphocytes + RBCs | Viral = lymphocytic; RBCs from hemorrhagic necrosis of temporal lobe |
| Glucose | Normal | Virus doesn't consume glucose (unlike bacteria/fungi/TB) |
| Protein | ↑ (mild) | Blood-brain barrier disruption from inflammation |
The One Rule to Lock This In
"Normal glucose + lymphocytes + RBCs + temporal lobe MRI swelling = HSV encephalitis"
- Viral meningitis = lymphocytes + normal glucose + normal/↑ protein (no RBCs)
- HSV encephalitis = lymphocytes + normal glucose + ↑ protein + RBCs (hemorrhagic necrosis)
Memory Hook
HSV hits the TEMPLE
→ Temporal lobe hemorrhagic NECROSIS
→ Blood leaks into CSF → RBCs
→ Virus doesn't eat glucose → glucose NORMAL
→ Lymphocytes (viral pattern)
→ TREAT with Acyclovir BEFORE PCR comes back
CSF Master Table (from your sheet — apply here)
| HSV Encephalitis | Viral Meningitis | Bacterial | TB/Fungal | |
|---|---|---|---|---|
| WBC | ↑ | ↑ | ↑↑ | ↑ |
| Cells | Lymphs + RBCs | Lymphocytes | Neutrophils | Lymphocytes |
| Glucose | Normal | Normal | Low | Low |
| Protein | ↑ | Normal/↑ | ↑↑ | ↑ |
Convert this UWorld question into ultra high-yield USMLE notes: 1. Diagnosis: 2. Key clue from question stem (1 line): 3. Why correct answer (max 2 lines): 4. Why others wrong (1 line each): 5. Buzzword trigger: 6. Trap / trick tested: 7. One-liner memory hook: Make it extremely concise. No paragraphs.
UWorld → Step 1 Flash Card
- Traumatic tap — RBCs only, no WBCs, no inflammation
- Bacterial meningitis — neutrophils + low glucose + ↑↑ protein; no temporal swelling
- TB/Fungal — lymphocytes + low glucose; glucose is the differentiator from HSV
- GBS — ↑ protein + normal cells (albuminocytologic dissociation); no fever/seizure
Temporal lobe swelling on MRI + fever + altered mental status + seizure = HSV-1
HSV Temples BLEED — Temporal lobe, Lymphs, Erythrocytes, Encephalitis, Died (>70% without Acyclovir), Glucose normal
make with heading of the topic for mr to usually copy paste and revisew
CNS Infections — HSV-1 Encephalitis
Topic: CSF Analysis Pattern in Encephalitis
- Traumatic tap — RBCs only, no WBCs, no inflammation
- Bacterial meningitis — neutrophils + low glucose + ↑↑ protein; no temporal swelling
- TB/Fungal — lymphocytes + low glucose; glucose is the key differentiator from HSV
- GBS — ↑ protein + normal cells (albuminocytologic dissociation); no fever/seizure
A 44-year-old man with a history of advanced HIV is brought to the office by his family due to progressive cognitive decline. Over the last several years he has had worsening memory deficits and difficulty carrying out simple mental tasks. The patient has had no headaches, slurred speech, muscle weakness, or changes in vision. He was diagnosed with HIV 7 years ago, but his medical follow-up and treatment compliance have been poor. The patient does not use tobacco, alcohol, or recreational drugs. Vital signs are normal. He has difficulty with delayed recall as well as several executive function tasks. The remainder of his neurologic examination is unremarkable. Two weeks later, he dies from severe pneumonia and respiratory failure. Which of the following histopathologic findings would most likely be found on biopsy of this patient's brain? his patient with a history of long-standing HIV infection, medical noncompliance, and progressive cognitive decline likely had HIV-associated dementia. Most cases occur in those with advanced HIV who have CD4 counts <200/mm3. Patients usually develop features of subcortical dementia, including attention or working memory deficits, executive dysfunction, and slow information processing. HIV enters the central nervous system via infected monocytes and establishes a productive infection in microglial cells (resident macrophages of the central nervous system) and blood-derived perivascular macrophages. Activation of these cells occurs in response to the infection, inflammatory cytokines, and HIV-derived proteins, which leads them to cluster around small areas of necrosis (forming microglial nodules) and fuse together to form multinucleated giant cells. Because HIV does not directly infect neurons, the underlying pathology of HIV-associated dementia is thought to stem from the release of neurotoxic compounds by these activated monocytes. (Choices A and B) Cerebral amyloid angiopathy is marked by beta-amyloid deposits in the walls of cortical blood vessels. This condition is usually asymptomatic but can be associated with intracerebral hemorrhage or Alzheimer dementia. Alzheimer dementia is also associated with neuritic (senile) plaques, which are extracellular deposits of beta-amyloid surrounded by dystrophic neurites; they stain positive with Congo red and are often located in the hippocampus. Alzheimer dementia is typically seen in older adults and is characterized by slowly progressive memory impairment and higher cortical dysfunction (eg, aphasia, agnosia, apraxia). (Choice C) Patients with rabies develop eosinophilic inclusion bodies in the cytoplasm of neuronal cells (Negri bodies). Rabies is a neurotropic virus that is transmitted by the saliva of infected animals, usually via a bite wound. Patients classically develop fever, hydrophobia (fear of water), and pharyngeal spasms. (Choice E) Huntington disease is an autosomal dominant disorder that causes choreiform movement, psychiatric disturbances, and dementia. It is characterized by severe neuronal loss in the caudate nucleus. (Choice F) Lacunar infarctions cause slit-like white matter cavities with surrounding gliosis. Recurrent lacunar infarctions can result in vascular dementia, which is often characterized by sudden/stepwise cognitive decline and focal neurologic deficits. Patients with vascular dementia are typically older and usually have cardiovascular risk factors. Educational objective: HIV-associated dementia should be suspected in patients with AIDS who have progressive cognitive decline. The characteristic histopathologic finding is microglial nodules (groups of activated microglia/macrophages around small areas of necrosis) and multinucleated giant cells.
CNS Infections — HIV-Associated Dementia (HAND)
Topic: Histopathology of HIV Brain Involvement
- Beta-amyloid vessel deposits — Cerebral amyloid angiopathy; hemorrhage risk, not dementia pattern
- Neuritic (senile) plaques + tangles — Alzheimer's; older age, aphasia/apraxia, Congo red +ve
- Negri bodies (cytoplasmic eosinophilic inclusions) — Rabies; animal bite, hydrophobia, pharyngeal spasms
- Caudate nucleus neuronal loss — Huntington's; choreiform movements, autosomal dominant
- Slit-like WM cavities + gliosis — Lacunar infarcts → vascular dementia; stepwise decline, CV risk factors
not that big heading just like subheading from next time please.
HIV-Associated Dementia | Histopathology of HIV Brain Involvement
A 57-year-old man is hospitalized for aspiration pneumonia. The patient was healthy and worked as an engineer without difficulty until about 4 months ago. Since that time, he has developed severe confusion, mood changes, and memory impairment and had to take medical leave from work. The patient is now completely dependent on his wife for toileting, feeding, and general self-care. Physical examination shows disorientation and sporadic, jerky extremity movements. During hospitalization, the patient lapses into a coma and dies. Postmortem examination of his brain shows widespread atrophy of the cerebral cortex and cerebellum. Histologic analysis of the patient's brain tissue would most likely show accumulation of which of the following? his previously healthy patient developed rapidly progressive dementia associated with myoclonus (eg, involuntary, jerky extremity movements) and brain atrophy (due to widespread neuronal loss). These findings are consistent with Creutzfeldt-Jakob disease (CJD), a rapidly fatal transmissible spongiform encephalopathy caused by prions. Prion protein (PrP) is found in both neuronal and nonneuronal brain cells and normally exist in an alpha-helical structure (PrPC). Prion disease occurs after a domain in this protein undergoes a conformational change from an alpha helix into a beta pleated sheet isoform (PrPSC), which confers the ability to induce similar conformational changes in other proteins. This beta sheet conformation is resistant to proteases and forms long, highly neurotoxic fibrils that accumulate intracellularly in neurons and form extracellular deposits. On microscopy, there is spongiform degeneration of the gray matter, which is characterized by formation of microscopic vacuoles within the neuronal processes. This leads to widespread neuronal loss and reactive gliosis without associated inflammation. This may be evident on imaging or gross pathology as widespread atrophy involving both the cerebrum and cerebellum (in contrast to many other neurodegenerative diseases that spare the cerebellum). (Choice A) Cytoplasmic inclusions of alpha-synuclein are characteristic of dementia with Lewy bodies, which is characterized by visual hallucinations, parkinsonism, cognitive fluctuations, and REM sleep disorder. (Choice B) Deposition of beta-amyloid occurs in Alzheimer dementia, which commonly presents with early and prominent memory impairment with language deficits and spatial disorientation. It is characterized by a slow (years to decades) decline in function until death. (Choice C) Phosphorylated tau forms paired helical filaments that create intracellular neurofibrillary tangles. This is seen in both Alzheimer disease as well as frontotemporal dementia. Although memory impairment and behavioral changes can occur in these diseases, this patient's myoclonus and rapid progression leading to death are more consistent with CJD. (Choice E) Prion diseases are the only known diseases that are transmissible by protein. Prion isoforms do not contain nucleic acids. Although HIV (an RNA virus) can cause dementia, it typically causes mild, subacute cognitive impairment without myoclonus. Educational objective: Creutzfeldt-Jakob disease is a prion disease characterized by rapidly progressive dementia, myoclonus, and death within a year of symptom onset. It is caused by the accumulation of an abnormally folded (ie, beta pleated sheet) protein that is resistant to proteases and can trigger similar conformational changes in other normally folded proteins.
CJD (Prion Disease) | Protein Accumulation & Histopathology
- Alpha-synuclein — Lewy body dementia; visual hallucinations + parkinsonism + REM sleep disorder; slow course
- Beta-amyloid — Alzheimer's; slow decline over years; no myoclonus; early memory + language
- Phosphorylated tau (neurofibrillary tangles) — Alzheimer's/FTD; no myoclonus, no rapid death
- RNA/nucleic acid — Prions have NO nucleic acid; transmitted by protein alone
A 54-year-old man is brought to the office by his friend because of worsening memory impairment over the past several months. The patient is also withdrawn and not focused during conversations. He is slow to answer questions or carry out instructions. The patient has a prolonged history of HIV infection and has had several opportunistic infections due to inconsistent antiretroviral medication use. On physical examination, he is alert and oriented. Muscle strength, deep tendon reflexes, and sensation are normal. MRI of the head shows diffuse cerebral atrophy with no focal mass lesions or areas of demyelination. Viral proliferation in which of the following central nervous system cells is most likely involved in this patient's disease process? A. CD4+ helper T cells (17%) B. Cortical neurons (23%) C. Endothelial cells (2%) D. Macrophages (36%) E. Oligodendrocytes (19%) n the context of a long history of HIV infection, this patient's memory impairment, subcortical dysfunction (ie, inattention, impaired psychomotor speed), and cerebral atrophy on MRI of the head are consistent with HIV-associated dementia (HAD). HAD is characteristically a subcortical dementia with prominent mood, attention, memory, and psychomotor dysfunction. It is uncommon in patients receiving antiretroviral treatment but can occur in those with inconsistently treated, advanced HIV infection. Although HIV-1 preferentially infects and replicates in CD4+ helper T cells in peripheral blood (Choice A), CNS infection is associated with a change in viral tropism (ie, ability to infect different cell types) to microglia and macrophages, which allows the virus to penetrate deeper into the brain parenchyma. This macrophage tropic (M-tropic) version of the virus becomes "compartmentalized" in the CNS and evolves independently from the strain found in the blood. (Choices B and E) HIV is not neuron or oligodendrocyte tropic. Viruses that are neuron tropic include the lyssaviruses that cause rabies. (Choice C) HIV does not preferentially infect and replicate in endothelial cells in the CNS. Cytomegalovirus is an example of an endothelial cell–tropic virus. Educational objective: HIV-associated dementia has become rare since the advent of antiretroviral treatment but may still develop in patients with inadequately treated, late-stage HIV infection. In the CNS, HIV preferentially infects and replicates in macrophages.
HIV-Associated Dementia | CNS Cell Tropism of HIV
- CD4+ T cells — HIV's peripheral blood target, NOT CNS; wrong compartment
- Cortical neurons — HIV is NOT neurotrophic; neurotoxicity is indirect via macrophage cytokines
- Endothelial cells — CMV is endothelial-tropic, not HIV
- Oligodendrocytes — JC virus targets oligodendrocytes → PML (demyelination); MRI here shows NO demyelination
A 55-year-old man with HIV comes to the emergency department due to 3 weeks of increasing headache, fever, and vomiting. Examination shows low blood pressure and neck stiffness. The patient's condition quickly deteriorates, and he dies in the hospital despite appropriate treatment. Autopsy of the brain shows a diffuse gelatinous exudate covering the base of the brain. Cut sections of the brain show marked ventriculomegaly and frontal lobe infarcts but no intraparenchymal mass lesions. Which of the following is the most likely diagnosis? his patient's subacute symptoms and autopsy findings are highly suggestive of tuberculous (TB) meningitis, the most common central nervous system (CNS) manifestation of disseminated TB. TB meningitis arises when circulating bacilli lodge in the subependymal or subpial space, forming a tubercle that subsequently ruptures into the subarachnoid space. Common findings include the following: A thick, gelatinous exudate most prominent in the basal portion of the brain. This exudate can encase the cranial nerves, leading to cranial nerve palsy, and invade the circle of Willis, leading to stroke. Tuberculous vasculitis of the cerebral arteries. This can cause multiple bilateral brain infarctions, particularly in the periventricular cerebral areas. Hydrocephalus due to obstruction of cerebrospinal fluid outflow by tubercular proteins. This can cause elevated intracranial pressure (eg, headache, nausea, vomiting) and ventriculomegaly. Although CNS invasion occurs in only ~5% of extrapulmonary TB, risk is increased in those with significant immunocompromise due to HIV, immunosuppressive medications, advanced age, or malnutrition. (Choice A) Herpes simplex virus type 1 can spread via the trigeminal nerve (CN V) to the brain. Patients usually develop rapid-onset (not subacute) fever, headache, seizure, altered mental status, and neurologic deficits. Autopsy typically shows unilateral temporal lobe inflammation, not hydrocephalus or a gelatinous exudate in the basal brain. (Choice B) Neurocysticercosis is caused by the larval stage of the pork tapeworm Taenia solium. It is generally marked by intraparenchymal cysts at several stages of development. The lack of intraparenchymal lesions makes neurocysticercosis unlikely. In addition, patients generally present with seizures or focal neurologic deficits. (Choice C) Primary CNS lymphoma is more common in patients with HIV but is usually marked by a single large mass in the parenchyma of the brain. The presence of a thick, gelatinous exudate and no intraparenchymal brain lesions would be atypical. (Choice D) Toxoplasma encephalitis is common in patients with advanced HIV who are not on prophylaxis. Although it often presents with slowly progressive headache, vomiting, and/or fever, it is marked by multiple intraparenchymal lesions in the brain. Educational objective: Tuberculous (TB) meningitis is characterized by formation of a thick, gelatinous exudate in the base of the brain; cerebral vasculitis; and hydrocephalus. It frequently presents with subacute, slowly progressive nausea, vomiting, fever, cranial nerve deficits, and strokes.
TB Meningitis | Autopsy Findings & CNS Manifestations
- HSV encephalitis — rapid onset, unilateral temporal lobe inflammation, no basal exudate or hydrocephalus
- Neurocysticercosis — intraparenchymal cysts at multiple stages; presents with seizures; no basal exudate
- CNS Lymphoma — single large intraparenchymal mass; more common in HIV but NOT a basal exudate
- Toxoplasma encephalitis — multiple ring-enhancing intraparenchymal lesions; CD4 <100; no basal exudate
A 44-year-old man comes to the office due to several weeks of difficulty walking and frequent falls. He has had no headache or visual impairment but reports episodes of sharp, stabbing pain in his extremities. The patient has HIV acquired from unprotected sexual contact and is nonadherent with treatments. Temperature is 37 C (98.6 F). Neurologic examination shows 5/5 motor power in all extremities. Deep-tendon reflexes are absent at the knee and ankle bilaterally. Proprioception and vibration sensation are reduced throughout the lower extremities. He has a wide-based gait and a positive Romberg sign. Which of the following diagnostic findings is most likely associated with this patient's current symptoms? Explanation Tabes dorsalis Epidemiology Years → decades after initial infection Increased incidence/more rapid progression in those with HIV Pathogenesis Treponema pallidum directly damages dorsal sensory roots Secondary degeneration of the dorsal columns Clinical findings Sensory ataxia Lancinating pains Neurogenic urinary incontinence Associated with Argyll Robertson pupils Treatment 10-14 days of intravenous penicillin G This patient's sensory ataxia and lancinating pains raises suspicion for tabes dorsalis, a late form of neurosyphilis that usually manifests several years or decades after initial infection with Treponema pallidum. Tabes dorsalis is characterized by a slow degeneration of nerve fibers in the dorsal column of the spinal cord and dorsal nerve roots, which leads to diminished vibratory, proprioception, and discriminative touch sensation. Common manifestations include: Sensory ataxia: Wide-based gait and loss of equilibrium when the patient's eyes are closed (positive Romberg sign); due to damaged lower extremity proprioception Absent deep-tendon reflexes: Due to damaged dorsal nerve roots Lancinating pains: Sharp, stabbing pains that may last minutes or hours; the exact cause is unclear Spirochetal damage to the midbrain tectum also commonly results in Argyll Robertson pupil. This finding is marked by small, irregularly shaped pupils that fail to constrict to light but that constrict normally to accommodation (light-near dissociation). Most patients with tertiary syphilis will have a positive VDRL and mild lymphocytic pleocytosis on cerebrospinal fluid analysis. (Choice A) Central nervous system infection with Mycobacterium tuberculosis, an acid-fast bacillus, is usually characterized by headache, vomiting, cranial nerve deficits, and confusion. Lancinating pains and altered lower extremity sensation would be atypical. (Choice B) Herpes simplex encephalitis primarily affects the temporal lobe and causes fever, headache, impaired consciousness, and seizures. (Choice C) Cryptococcal meningitis can be diagnosed by examining the cerebrospinal fluid for encapsulated yeasts using India ink. However, cryptococcal meningitis usually manifests with fever, malaise, and headache. Lancinating pains, absent deep-tendon reflexes, and altered sensation would be atypical. (Choice D) JC virus is a polyomavirus that replicates in oligodendrocytes (glial cells). Reactivation of JC virus causes progressive multifocal leukoencephalopathy, which occurs primarily in severely immunocompromised patients (eg, AIDS, lymphoma, leukemia) and causes progressive dementia, motor deficits, and visual impairment. (Choice F) Patients with untreated HIV are at high risk for cerebral toxoplasmosis, which usually manifests with headache, confusion, fever, and focal neurologic deficits. MRI of the brain usually reveals ring-enhancing lesions. Educational objective: Tabes dorsalis, a late form of neurosyphilis, causes progressive degeneration of the dorsal columns and dorsal roots of the spinal cord. Manifestations include loss of proprioception and vibratory sensation, severe lancinating pains, and sensory ataxia (eg, wide-based gait, positive Romberg sign). Many patients also have Argyll Robertson pupils.
Neurosyphilis — Tabes Dorsalis | Dorsal Column Degeneration
- TB meningitis (AFB) — headache, vomiting, CN palsies, confusion; no lancinating pains or dorsal column signs
- HSV encephalitis — fever, temporal lobe, seizures, altered consciousness; no spinal cord involvement
- Cryptococcal meningitis — fever, headache, malaise; India ink + in CSF; no DTR loss or lancinating pains
- JC virus / PML — oligodendrocyte destruction, demyelination, dementia, motor/visual deficits; no dorsal column pattern
- Toxoplasmosis — ring-enhancing brain lesions, headache, confusion, focal deficits; CD4 <100