Side effects of ocp And criteria for pcod
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information for both topics. Here is the full answer:
Side Effects of OCP (Oral Contraceptive Pill)
Cardiovascular Effects
- Thromboembolic disease - the most serious risk. Estrogen stimulates hepatic synthesis of clotting factors and increases platelet aggregability. Thromboembolism risk is greatest in smokers over 35 years of age.
- Hypertension - seen in ~5% of users, especially those with pre-existing hypertension. Lower with newer low-dose preparations.
- Lipid effects - progestins tend to raise LDL and lower HDL; estrogens do the opposite. Modern low-dose pills generally do not produce unfavorable lipid profiles, though slight triglyceride elevation is possible.
- Migraine - risk of stroke with combined OCP in women who have migraine with aura.
Metabolic and Endocrine Effects
- Early high-dose pills impaired glucose tolerance; current low-dose preparations may actually improve insulin sensitivity.
- Estrogen component increases hepatic synthesis of binding proteins for thyroid hormones, glucocorticoids, and sex steroids - this can affect interpretation of endocrine function tests.
- Increased risk of gallbladder disease (weak association, mainly in current or very long-term users).
GI and Hepatic Effects
- Nausea and vomiting - common early side effect, usually transient.
- Hepatic adenoma and hepatocellular carcinoma - approximately 2-fold increased risk of liver cancer after 4-8 years of use, but these are rare cancers and absolute increases are small.
- Cholestasis (rare).
Breast and Reproductive Effects
- Breakthrough bleeding / irregular spotting - especially in early cycles.
- Breast tenderness - due to estrogenic effect.
- Small increase in breast cancer relative risk (1.1-1.2x) in current users of childbearing age. Importantly, 10 years after stopping, there is no difference vs. never-users. Cancers diagnosed in users tend to be more localized.
- Cervical cancer - ~2-fold increased risk only in long-term users (>5 years) with persistent HPV infection.
Protective / Beneficial Effects (Worth Noting)
- Reduces endometrial cancer by ~50% (lasts 15 years after stopping).
- Reduces ovarian cancer incidence.
- Likely reduces colorectal cancer risk.
- Reduces dysmenorrhea, menorrhagia, and pelvic inflammatory disease.
CNS / Mood
- Headache, mood changes, decreased libido reported in some users.
- Interaction with St. John's Wort - reduces OCP efficacy.
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics
Diagnostic Criteria for PCOS (Polycystic Ovary Syndrome)
Three Major Criteria Sets
1990 NIH Criteria (BOTH must be present)
- Chronic anovulation
- Clinical and/or biochemical signs of hyperandrogenism + exclusion of other etiologies
2003 Rotterdam Consensus Criteria (2 out of 3 required) - Most Widely Used
- Oligoovulation or anovulation (oligomenorrhea or amenorrhea)
- Clinical and/or biochemical signs of hyperandrogenism
- Polycystic ovaries on ultrasound + exclusion of other etiologies (congenital adrenal hyperplasia, androgen-secreting tumors, Cushing syndrome)
PCOS is a diagnosis of exclusion - other disorders mimicking it must be ruled out first.
Four Rotterdam Phenotypes
| Phenotype | HA | Ovarian Dysfunction | PCO Morphology |
|---|---|---|---|
| 1 | + | + | + |
| 2 | + | + | - |
| 3 | + | - | + |
| 4 | - | + | + |
Ultrasound Criteria for PCO Morphology
- ≥20 follicles in either ovary measuring 2-9 mm in diameter, AND/OR
- Increased ovarian volume (>10 mL)
- A single ovary meeting the criteria is sufficient.
Note: PCO appearance alone is found in ~23% of reproductive-age women. Only a fraction of these have the full clinical syndrome of PCOS (prevalence 5-10%).
Clinical Features of Hyperandrogenism
- Hirsutism (most common - ~70% of PCOS in the US)
- Acne
- Male-pattern alopecia
- Biochemical: elevated free/total testosterone, elevated DHEAS
Minor Diagnostic Criteria (less consistent)
- Elevated LH:FSH ratio
- Insulin resistance (IR)
- Perimenarchal onset of hirsutism
- Obesity (present in >50% of PCOS patients; central/android distribution)
Conditions to Exclude (Differential Diagnosis)
- Hyperprolactinemia
- Non-classic congenital adrenal hyperplasia (measure basal 17-OHP)
- Cushing's syndrome
- Androgen-secreting neoplasm
- Thyroid disorder
- Hypo/hypergonadotropic disorders
PCOS Diagnostic Algorithm
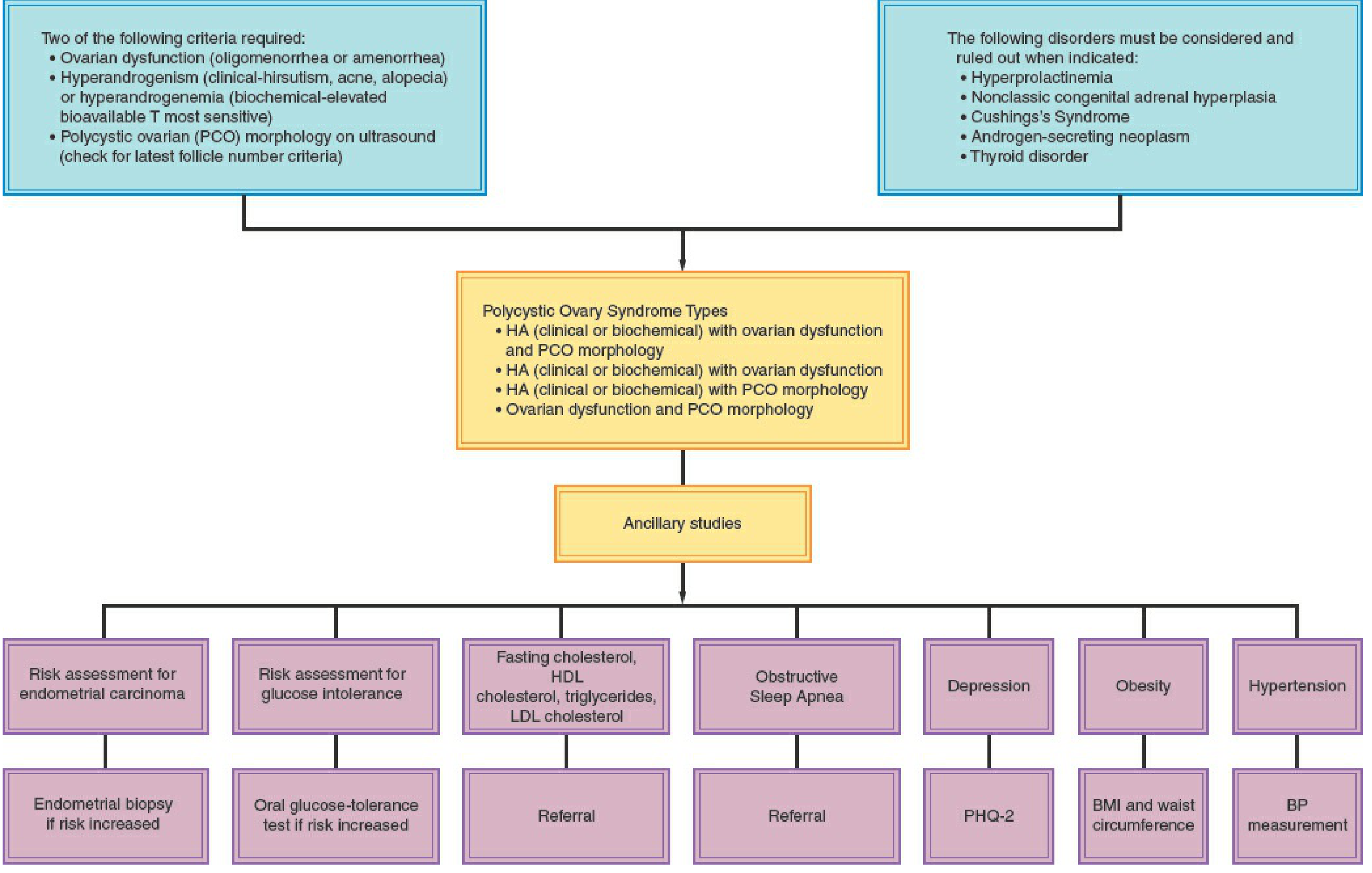
Associated Metabolic Risks (Workup Indicated)
- ~1/3 of obese PCOS patients have impaired glucose tolerance; 7.5-10% have type 2 DM
- Increased cardiovascular risk (check fasting lipids)
- Obstructive sleep apnea
- Endometrial carcinoma risk (from chronic unopposed estrogen due to anovulation)
- Depression screening (PHQ-2)
Source: Berek & Novak's Gynecology
What is insulin resistance and bro a gyne diagnosed pcod in me But i have no symptoms of pcod at all I have regular periods like 2-3 days irrigalir and no hirautism but yeah my usg said
Finding Sources
Finding Sources
Reading File
Reading File
I have all I need. Here's a clear, honest answer for you:
About Your Diagnosis - Is It Really PCOS?
This is genuinely important. Based on what you described - regular periods (only 2-3 days irregular), no hirsutism, and only an ultrasound finding - you may not actually meet the criteria for a PCOS diagnosis. Here's why:
Rotterdam Criteria (the standard used globally)
You need 2 out of 3 of these:
- Oligomenorrhea/anovulation (irregular periods)
- Clinical or biochemical hyperandrogenism (hirsutism, acne, elevated testosterone)
- Polycystic ovarian morphology on USG
From what you've described, you only clearly have criterion 3 (the USG finding). That alone is not enough to diagnose PCOS.
The Key Point
An ultrasound showing polycystic ovarian appearance is found in about 23% of all reproductive-age women - but only 5-10% actually have PCOS. An English study confirmed that a PCO appearance alone, without symptoms, is not associated with impaired fertility or fecundity.
- Berek & Novak's Gynecology
So many women get told they have "PCOD" based only on an ultrasound, when they don't actually have the syndrome. The ultrasound is just one part of the picture.
What You Should Do
Ask your gynecologist to check:
- Testosterone levels (free and total)
- LH:FSH ratio (elevated LH suggests true PCOS)
- Fasting insulin and glucose (to check insulin resistance)
- Prolactin, TSH (to rule out other causes)
- AMH (anti-Mullerian hormone - reflects follicle count)
If these are all normal and your periods are mostly regular, the diagnosis needs to be reconsidered.
What is Insulin Resistance?
Normally, when you eat, insulin is released by the pancreas. Insulin acts like a "key" that lets glucose enter your cells (especially muscle and liver) for energy.
Insulin resistance means your cells stop responding properly to insulin - the "lock" is broken. So your pancreas has to produce more and more insulin to get the same effect. This leads to:
- High circulating insulin levels (hyperinsulinemia)
- Eventually, blood sugar starts rising (pre-diabetes, then type 2 diabetes)
How it connects to PCOS
In PCOS, high insulin levels stimulate the ovaries to produce excess androgens (male hormones like testosterone). This is the main hormonal driver behind hirsutism, acne, and irregular cycles in PCOS.
Cascade:
Insulin resistance → Hyperinsulinemia → Ovarian androgen overproduction → Irregular ovulation + Hyperandrogenism
Harrison's Principles of Internal Medicine (2025)
Signs that might suggest insulin resistance even without obvious PCOS symptoms:
- Dark, velvety skin patches at the neck/armpits/groin (acanthosis nigricans)
- Weight gain around the belly
- Fatigue after carb-heavy meals
- Craving sweets constantly
Bottom line for you: Get blood work done (testosterone, LH/FSH, fasting insulin, TSH, prolactin) before fully accepting a PCOS label. An ultrasound alone isn't a diagnosis. If your bloodwork is normal and periods are regular, you may simply have polycystic ovarian morphology - which is a variant of normal, not a disease.
Find latest guidelines on PCOS diagnosis in asymptomatic women
Reading File
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND "diagnosis"[MeSH Terms] AND guideline
Searching the Web
PCOS diagnosis guidelines 2023 2024 asymptomatic women ultrasound only Rotterdam criteria update
Reading Article
PMID: 37804097
Searching the Web
Teede 2023 international evidence-based guideline PCOS diagnosis recommendations asymptomatic ultrasound morphology only
Reading Article
PMID: 37580861
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10505534
Excellent - I now have everything needed for a thorough, guideline-based answer. Here it is:
Latest Guidelines on PCOS Diagnosis (2023 International Evidence-Based Guideline)
Source: Teede HJ et al. (2023). Recommendations from the 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS. European Journal of Endocrinology. PMID: 37580861 - cited over 2,200 times. This is the most current global gold standard, covering 71 countries and 39 professional organizations.
Core Diagnostic Rule (Still 2 out of 3 - Rotterdam Backbone)
The 2023 guideline builds on the 2003 Rotterdam criteria. You still need 2 of these 3:
| Criterion | What it means |
|---|---|
| 1. Hyperandrogenism | Clinical (hirsutism, acne, alopecia) OR biochemical (elevated free testosterone) |
| 2. Ovulatory dysfunction | Irregular or absent periods (oligomenorrhea/anovulation) |
| 3. Polycystic ovarian morphology (PCOM) | On ultrasound OR now also by elevated AMH (new in 2023) |
Key update in 2023: Anti-Mullerian hormone (AMH) can now be used as an alternative to ultrasound for criterion 3 in adults. This is a new addition not in previous guidelines.
What the 2023 Guideline Says About Ultrasound-Only / Asymptomatic Cases
This is directly relevant to your situation:
Ultrasound Criteria (Updated Thresholds)
| Marker | Threshold (2023) | Notes |
|---|---|---|
| FNPO (follicle number per ovary) | ≥20 follicles in at least 1 ovary | Gold standard, most accurate (sensitivity 84%, specificity 91%) |
| Ovarian volume (OV) | ≥10 mL in at least 1 ovary | Use if full follicle count can't be done |
| FNPS (follicle number per cross-section) | ≥10 in at least 1 ovary | Alternative if older tech |
Note: The 2003 Rotterdam criteria used ≥12 follicles. The threshold was later raised to ≥25, and the 2023 guideline now sets it at ≥20. If your USG used the old ≥12 cutoff, the finding may not even meet modern criteria.
The Critical Practice Points (Direct Quotes from 2023 Guideline):
PP 1.4.9: "In patients with irregular menstrual cycles and hyperandrogenism, an ovarian ultrasound is NOT necessary for PCOS diagnosis."
PP 1.4.6: "There are no definitive criteria to define PCOM on ultrasound in adolescents; hence, it is NOT recommended in adolescents."
The guideline explicitly states: "Where irregular menstrual cycles and hyperandrogenism are present, diagnosis is simplified and ultrasound or AMH are NOT required for diagnosis."
What this means for you:
The guideline works in reverse too - if you only have the ultrasound finding (criterion 3) but neither hyperandrogenism nor ovulatory dysfunction, you do NOT meet the diagnosis. PCOM on ultrasound alone is never sufficient.
The Systematic Review on USG Accuracy (2024)
Pea et al., 2024 - Hum Reprod Update - the most rigorous meta-analysis on USG criteria for PCOS to date:
- Analyzed 31 studies, 3,883 controls vs. 3,859 PCOS patients
- FNPO = best single marker (sensitivity 84%, specificity 91%, AUC 0.905)
- The meta-analysis could NOT determine a single definitive cutoff due to heterogeneity across geographic regions - Asian studies showed different diagnostic accuracy than European or North American ones
- Significant geographical variation: BMI, age, ethnicity affect what "polycystic morphology" means
For Adolescents Specifically
The 2023 guideline is even stricter:
- Ultrasound should not be used for PCOS diagnosis in adolescents (poor specificity - many teens normally have multi-follicular ovaries)
- In adolescents, both hyperandrogenism AND ovulatory dysfunction are required
- AMH also not recommended for adolescent diagnosis
Bottom Line for Your Case
Based on the 2023 International Guidelines:
- USG showing polycystic morphology alone = NOT a PCOS diagnosis. Full stop.
- You need at least one more criterion - either hyperandrogenism (blood tests for testosterone, clinical signs) OR confirmed anovulation (not just slightly irregular periods).
- A 2-3 day irregularity in cycle length is within normal variation and does not constitute oligomenorrhea (which means cycles >35 days or <8 cycles/year).
- The gynecologist should have ordered blood tests (free testosterone, LH/FSH, AMH, insulin, TSH, prolactin) before diagnosing you.
- If only an ultrasound was done, the diagnosis is not evidence-based per current guidelines.
The most appropriate next step is to ask your doctor: "Do I meet 2 out of 3 Rotterdam criteria confirmed by clinical exam and blood tests, or only the ultrasound criterion?"
This is a shared conversation. Sign in to Orris to start your own chat.