The tinged edema is caused due to elevated vascular hydrostatic pressure and reduced plasma osmotic pressure. Can you explain to me clearly how?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the material needed to give a thorough, well-illustrated answer. Let me compose it.
Edema from Elevated Hydrostatic Pressure and Reduced Plasma Osmotic Pressure
The term you are referring to - "tinged edema" - most likely refers to non-inflammatory (transudate) edema, the type of fluid accumulation driven purely by disturbances in Starling forces across the capillary wall. Here is how each mechanism works.
The Normal Balance: Starling Forces
At any capillary bed, fluid movement is governed by two opposing pressures:
| Force | Direction of Action | Normal Value (approx.) |
|---|---|---|
| Capillary hydrostatic pressure | Pushes fluid OUT of vessels into interstitium | ~37 mmHg (arteriolar end), ~17 mmHg (venous end) |
| Plasma colloid osmotic pressure (oncotic pressure) | Pulls fluid INTO vessels | ~25 mmHg |
| Tissue/interstitial pressure | Opposes outward flow | ~1 mmHg |
At the arteriolar end: hydrostatic pressure (37 mmHg) > osmotic pressure + tissue pressure (26 mmHg), so fluid filters out into the interstitium.
At the venous end: hydrostatic pressure falls to ~17 mmHg, which is now less than osmotic pressure (25 mmHg), so fluid is drawn back in.
The small net excess that leaks out is handled by lymphatics, which return it to the bloodstream through the thoracic duct. This keeps tissues "dry."
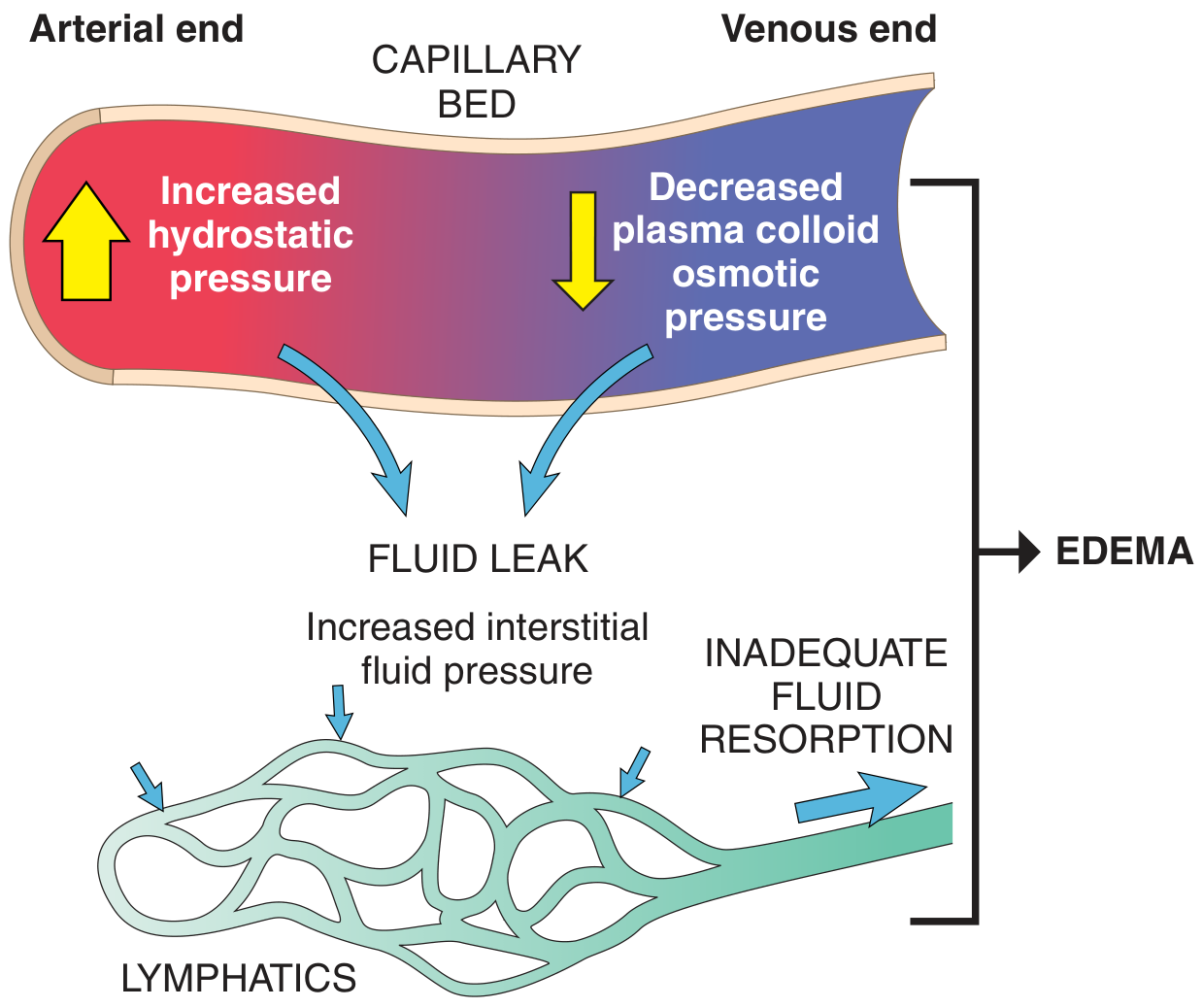
Fig. 3.2 - Factors influencing fluid movement across capillary walls. Both increased hydrostatic pressure and decreased plasma osmotic pressure shift the balance toward fluid accumulation in the interstitium. - Robbins & Kumar Basic Pathology
Mechanism 1: Elevated Vascular Hydrostatic Pressure
When venous hydrostatic pressure rises, the gradient at the venous end changes dramatically:
- Normally, the venous-end hydrostatic pressure (~17 mmHg) is overcome by osmotic pressure (~25 mmHg), allowing reabsorption.
- If hydrostatic pressure rises (say to 30+ mmHg), the capillary now pushes fluid out at both ends, and osmotic pressure is no longer sufficient to reclaim the leaked fluid.
- The lymphatics are overwhelmed, and interstitial fluid accumulates = edema.
Common causes of elevated hydrostatic pressure:
| Cause | Mechanism |
|---|---|
| Congestive heart failure (CHF) | Reduced cardiac output → blood pools in venous system → increased capillary back-pressure |
| Deep vein thrombosis (DVT) | Venous obstruction → raised pressure distally |
| Renal failure / Na+ retention | Expanded blood volume → increased intravascular pressure |
In CHF specifically, reduced cardiac output also triggers the renin-angiotensin-aldosterone system (RAAS), causing sodium and water retention by the kidneys. This further expands blood volume and worsens hydrostatic pressure - a self-reinforcing cycle that perpetuates the edema unless diuretics or RAAS blockers are used.
Mechanism 2: Reduced Plasma Osmotic (Colloid Oncotic) Pressure
Plasma osmotic pressure depends predominantly on albumin, which makes up ~60% of total plasma protein and contributes 70-80% of total osmotic pressure. When albumin levels fall:
- The "pulling-in" force at the venous end is weakened.
- Even at a normal venous hydrostatic pressure of ~17 mmHg, the reduced osmotic pressure (now below 17 mmHg) can no longer pull fluid back into the vessel.
- Net fluid movement is outward throughout the capillary, and edema results.
Common causes of reduced plasma albumin:
| Cause | Mechanism |
|---|---|
| Nephrotic syndrome | Glomerular damage → albumin lost in urine (albuminuria) |
| Liver cirrhosis / liver failure | Reduced hepatic albumin synthesis |
| Protein malnutrition (kwashiorkor) | Inadequate protein intake → decreased albumin production |
A secondary effect makes this worse: falling albumin reduces intravascular volume, which triggers renal hypoperfusion, activating RAAS again. The kidney retains more sodium and water - but because the fundamental problem (low protein) persists, this extra volume just leaks back into the interstitium, worsening edema rather than fixing it.
The Nature of the Fluid: Transudate
The edema fluid that results from either of these two mechanisms is characteristically a protein-poor transudate - because the capillary wall is structurally intact. No proteins leak through. This distinguishes it from inflammatory edema (exudate), where vessel permeability is increased and protein-rich fluid leaks out.
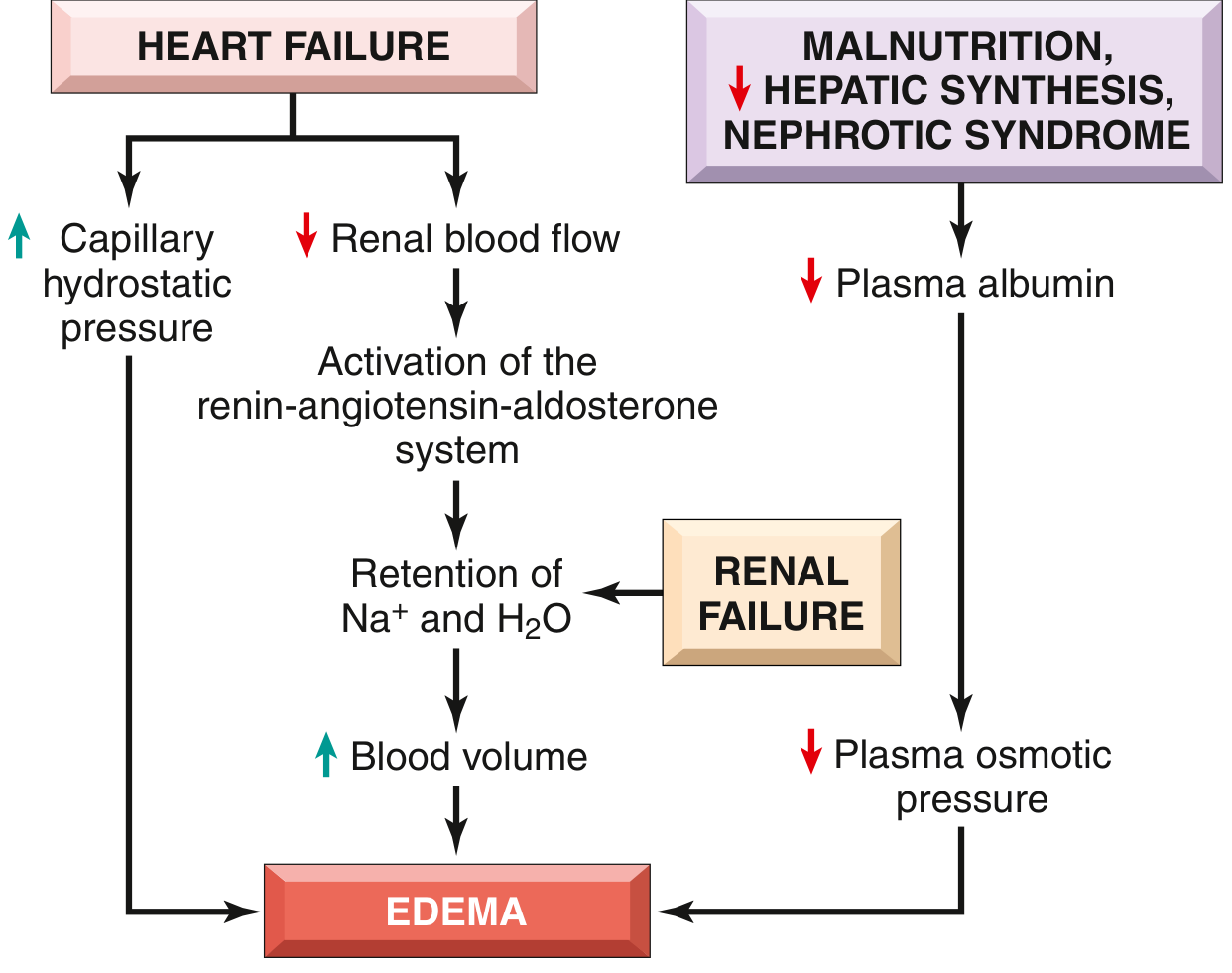
Fig. 3.3 - Pathways leading to systemic edema from heart failure, renal failure, or reduced plasma osmotic pressure. - Robbins & Kumar Basic Pathology
Summary Table
| Parameter | Elevated Hydrostatic Pressure | Reduced Osmotic Pressure |
|---|---|---|
| Primary disturbance | Increased outward pressure | Decreased inward pull |
| Net effect | Fluid pushed out at venous end too | Fluid not reabsorbed at venous end |
| Fluid type | Protein-poor transudate | Protein-poor transudate |
| Key clinical examples | CHF, DVT, renal failure | Nephrotic syndrome, cirrhosis, kwashiorkor |
| Secondary RAAS activation | Yes (via low cardiac output) | Yes (via low intravascular volume) |
Both mechanisms converge on the same final result: the lymphatic system's capacity to drain excess interstitial fluid is overwhelmed, and fluid accumulates in the tissues as edema.
- Robbins & Kumar Basic Pathology, pp. 78-81
- Basic Medical Biochemistry: A Clinical Approach (6e), p. 1549-1551
Explain how pitting pedal edema occurs
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed. Let me compose a clear, detailed answer.
How Pitting Pedal Edema Occurs
Pitting pedal edema is the accumulation of excess protein-poor fluid in the interstitial spaces of the feet and ankles, which produces a visible, temporary indentation (a "pit") when firm pressure is applied with a finger. Understanding it requires breaking it down into three layers: why fluid accumulates, why it collects in the feet specifically, and why it pits.
Step 1: Disruption of Starling Forces (Fluid Accumulation)
As we discussed, the capillary bed is governed by two opposing forces:
- Capillary hydrostatic pressure - pushes fluid out into the interstitium
- Plasma colloid oncotic (osmotic) pressure - pulls fluid back in
At baseline, these forces are roughly balanced. Pitting pedal edema develops when this balance is broken by one or more of the following:
| Mechanism | What Happens | Examples |
|---|---|---|
| Elevated capillary hydrostatic pressure | Increased outward fluid push overwhelms oncotic reabsorption | Heart failure, DVT, venous insufficiency |
| Reduced plasma oncotic pressure | Inward pull is weakened; fluid leaks even at normal pressures | Nephrotic syndrome, liver cirrhosis, malnutrition |
| Sodium/water retention | Expanded blood volume raises venous back-pressure | Renal failure, RAAS activation |
When the excess fluid leaked into the interstitium exceeds the lymphatic drainage capacity, it accumulates - this is edema.
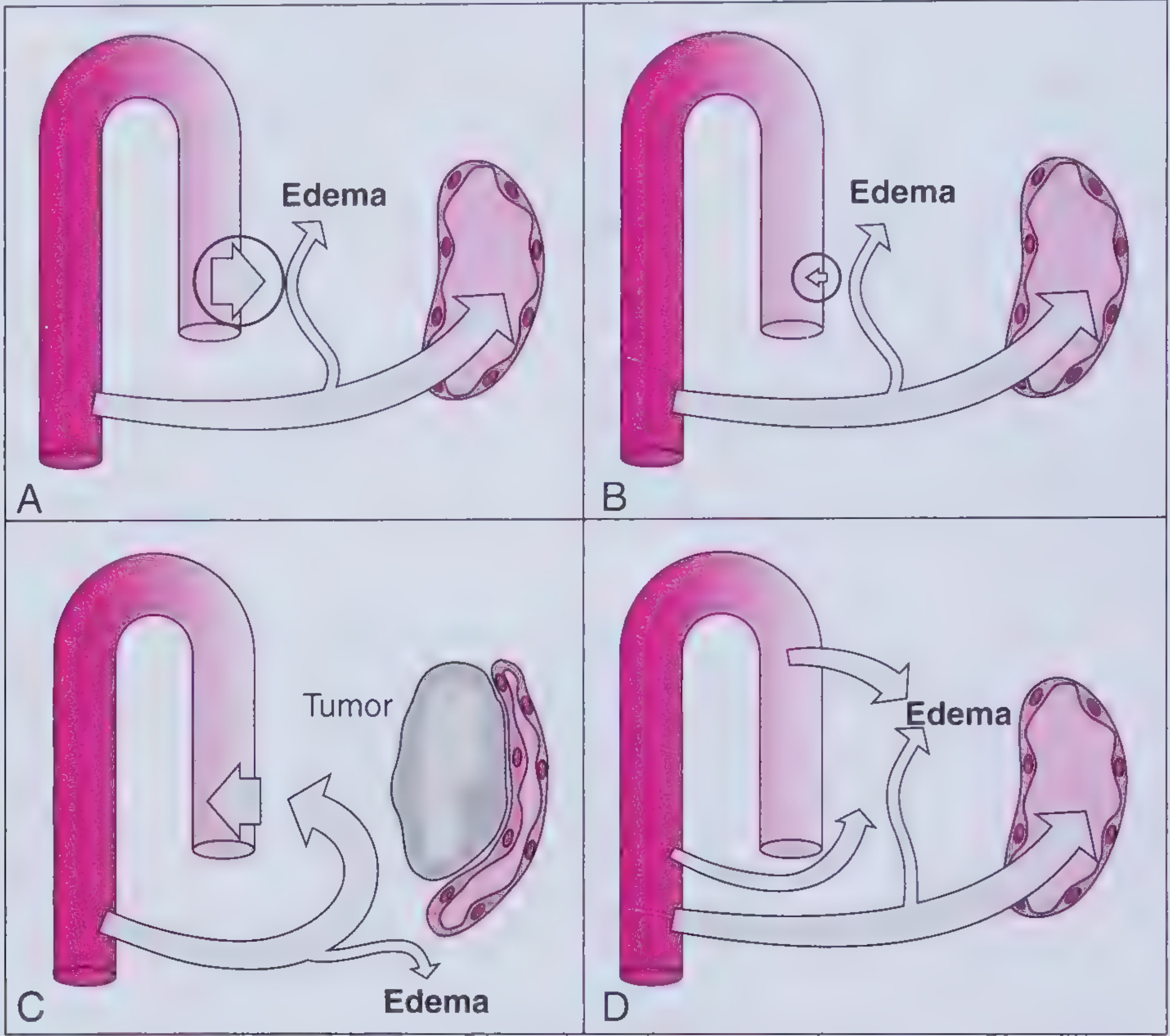
A - Increased hydrostatic pressure; B - Decreased oncotic pressure; C - Lymphatic obstruction (tumor); D - Increased capillary permeability. - Frameworks for Internal Medicine
Step 2: Why Fluid Collects in the Feet (Dependent Edema)
Gravity is the key reason. Subcutaneous edema preferentially accumulates in the most dependent parts of the body - the parts positioned farthest below the heart. This is called dependent edema.
Here is why gravity matters at the capillary level:
- The hydrostatic pressure inside capillaries is not uniform throughout the body. It is substantially higher in the lower extremities than in, say, the neck or chest - because the column of blood above adds pressure.
- In an upright (standing or sitting) person, capillary hydrostatic pressure in the feet is significantly higher than the same person's arm or face. This extra gravitational pressure tilts the Starling balance further toward fluid efflux in the feet.
- The venous return from the feet also has to work against gravity, so any impairment in venous return (e.g., from heart failure or venous insufficiency) raises venous back-pressure most severely in the feet.
Clinical corollary:
- In ambulatory patients - edema is worst in the feet and ankles at the end of the day
- In bed-bound patients - edema shifts to the sacral area, which is now the most dependent part
- With worsening disease - edema climbs up to the legs, thighs, genitalia, and eventually becomes anasarca
"Subcutaneous edema preferentially occurs in parts of the body positioned the greatest distance below the heart, where hydrostatic pressures are highest. Thus, edema is most pronounced in the legs with standing and the sacrum with recumbency, a relationship termed dependent edema." - Robbins & Kumar Basic Pathology, p. 79
Step 3: Why it PITS
This is the mechanically distinctive feature of pitting vs. non-pitting edema.
When pressure is applied (e.g., a finger pressed over the dorsum of the foot or over the tibia):
- The interstitial fluid is a free, mobile liquid - it is not bound to matrix components. It is essentially a protein-poor transudate sitting loosely in the extracellular spaces between cells and collagen fibers.
- The applied pressure physically displaces this free fluid away from the compression site into surrounding tissues.
- When pressure is removed, the fluid slowly seeps back into the compressed area - but this takes time (seconds to minutes), leaving a visible pit.
- The pit persists because the interstitial fluid has no immediate restoring force - it must redistribute passively by hydrostatic equalization within the interstitium.
Why some edema is NON-pitting: In lymphedema or long-standing edema, proteins accumulate in the interstitium (because lymphatics - which normally drain proteins - are overwhelmed or obstructed). These proteins stimulate fibrosis and fat deposition, which fills the interstitial spaces with solid material. Fluid can no longer be easily displaced, so no pit forms.
Grading of Pitting Edema
| Grade | Indentation Depth | Resolution Time |
|---|---|---|
| 1+ | < 2 mm | Immediate |
| 2+ | 2-4 mm | < 15 seconds |
| 3+ | 4-6 mm | 15-30 seconds |
| 4+ | > 6 mm | > 30 seconds |
A more precise clinical method is to measure the indentation depth in millimeters over a bony prominence (e.g., the medial malleolus or tibia).
Note on Systemic Hypertension
A common misconception: systemic arterial hypertension does not cause pitting pedal edema. This is because precapillary sphincters (autoregulation) prevent elevated arterial pressure from being transmitted into the capillary bed. It is specifically venous/capillary pressure that drives edema - not arterial pressure.
Summary Flow
Elevated venous hydrostatic pressure
AND/OR reduced plasma oncotic pressure
↓
Excess fluid leaks into interstitium
↓
Lymphatic drainage is overwhelmed
↓
Fluid accumulates in tissues
↓
Gravity → collects in feet (dependent site)
↓
Free interstitial fluid displaced by finger pressure
↓
PITTING PEDAL EDEMA
- Robbins & Kumar Basic Pathology, pp. 78-81
- Frameworks for Internal Medicine, pp. 305-307
- Harrison's Principles of Internal Medicine 22E, Chap. 43
This is a shared conversation. Sign in to Orris to start your own chat.