Intestinal obstruction
Reading File
Finding Sources
Finding Sources
Searching PubMed
"intestinal obstruction" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Intestinal Obstruction
A complete blockage or impairment of the normal passage of intestinal contents, either due to mechanical factors or failure of intestinal motility (adynamic/functional). It is one of the most common acute surgical emergencies.
Classification
1. By Mechanism
| Type | Description |
|---|---|
| Mechanical (Dynamic) | Physical blockage of the lumen; peristalsis is active and fighting against the obstruction |
| Adynamic (Paralytic Ileus) | Failure of normal propulsive motility without a mechanical cause; occurs after surgery, peritonitis, metabolic disturbance |
| Vascular (Ischaemic) | Obstruction due to vascular occlusion leading to bowel infarction |
2. By Level
- Small bowel obstruction (SBO) - high (proximal) or low (distal)
- Large bowel obstruction (LBO)
3. By Completeness
- Complete - no passage of flatus or faeces
- Incomplete (partial/subacute) - intermittent symptoms, some passage
4. By Vascularity
- Simple - blood supply is intact
- Strangulating/Strangulated - blood supply is compromised, leading to ischaemia, infarction, gangrene, and perforation
Causes
Mechanical Causes (Extraluminal, Mural, Intraluminal)
The cause may be due to extrinsic compression, an abnormality in the bowel wall, or an obstructing foreign body in the lumen. - Pye's Surgical Handicraft, 22nd Ed.
A. Lesions Extrinsic to the Bowel Wall
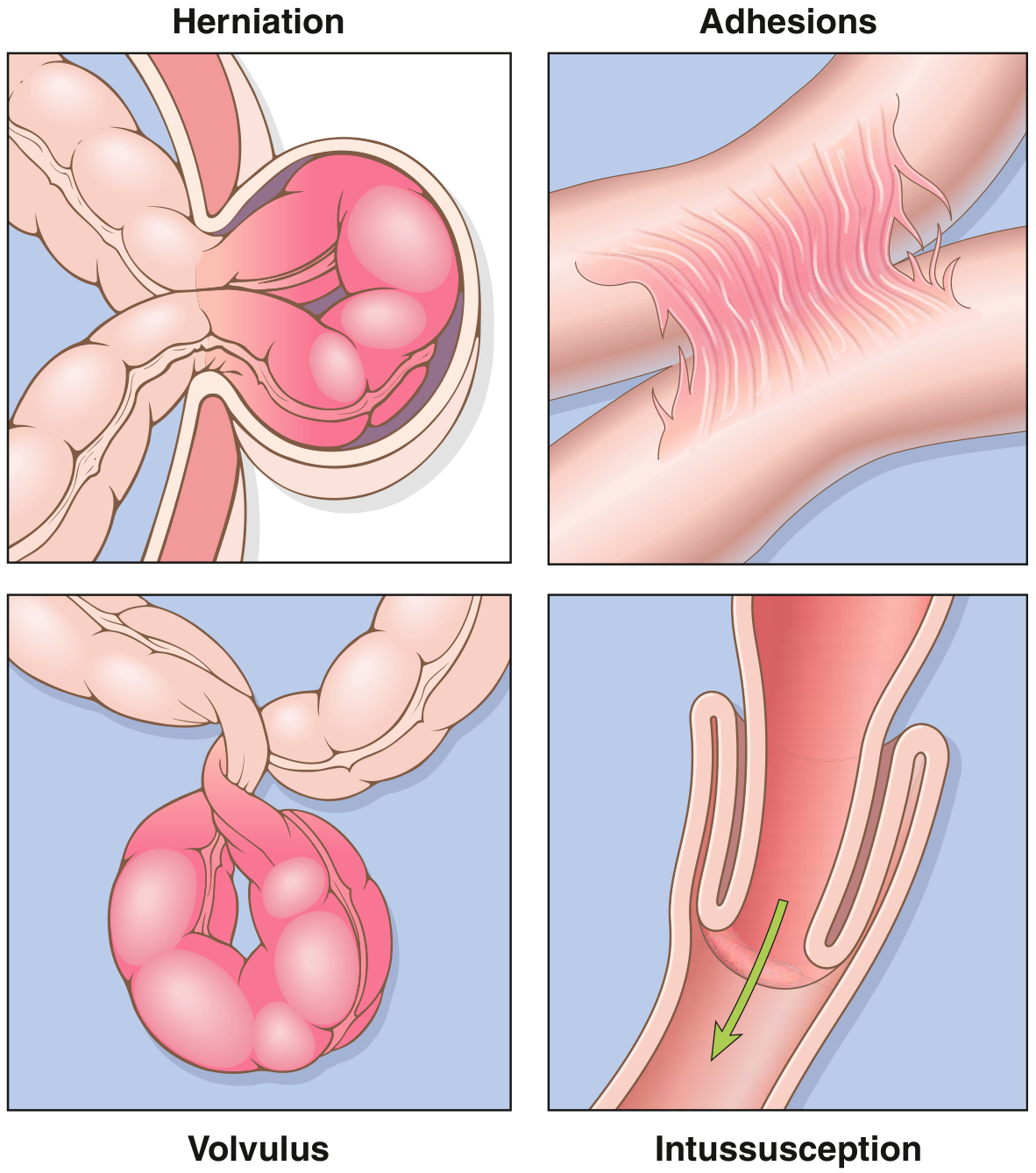
- Adhesions - most common cause in Western countries, responsible for >60% of SBO, particularly after pelvic/lower abdominal surgery (gynaecological, appendicectomy, colorectal)
- Hernias - second most common (~10%); inguinal, femoral, umbilical, ventral, obturator, internal hernias
- Neoplastic (carcinomatosis, external compression)
- Intra-abdominal abscess (from ruptured appendix, diverticular disease)
- Volvulus (sigmoid and caecal most common; sigmoid volvulus is the most common cause of LBO in sub-Saharan Africa)
B. Lesions Intrinsic to the Bowel Wall
- Congenital: malrotation, duplications, Hirschsprung disease
- Inflammatory: Crohn disease (4th leading cause of SBO, ~5%), diverticulitis, tuberculosis
- Neoplastic: primary tumours, metastatic tumours
- Radiation enteropathy/stricture
- Intussusception (most common cause in children <2 years)
C. Intraluminal / Obturator Obstruction
- Gallstone ileus, bezoar, enterolith, foreign body
Collectively, hernias, adhesions, intussusception, and volvulus account for 80% of mechanical obstructions. - Robbins & Kumar Basic Pathology
Adynamic (Paralytic) Ileus
- Post-operative (most common) - small bowel returns in 24h, colon in 3-5 days
- Peritonitis, intra-abdominal abscess, hemoperitoneum
- Electrolyte imbalance (hypokalaemia)
- Sepsis, pneumonia, retroperitoneal haematoma
- Drugs (opioids, anticholinergics)
Pathophysiology
When the small bowel is obstructed, up to 6 litres of salt-rich fluid secreted daily into the small intestine cannot be reabsorbed in the colon, leading to massive fluid and electrolyte loss either by vomiting or sequestration in the lumen ("third spacing"). - Pye's Surgical Handicraft
Consequences:
- Fluid and electrolyte depletion - dehydration, hypovolaemia, pre-renal failure
- Bowel wall oedema and distension - increased intraluminal pressure reduces venous outflow, then arterial inflow
- Bacterial overgrowth - leads to feculent vomiting; bacterial translocation across ischaemic mucosa causes sepsis
- Strangulation - obstruction to arterial supply or venous drainage causes loss of bowel viability, necrosis, gangrene, perforation
Closed-loop obstruction occurs when both ends of a bowel segment are obstructed (e.g., by adhesive band or internal hernia), producing rapid ischaemia. CT shows a "U-loop" or "coffee-bean sign" with tapering at both ends. Twisting of this loop produces a volvulus (mesenteric whirl sign). - Sabiston Textbook of Surgery
Clinical Features
The Classic Quartet (Dynamic Obstruction)
- Abdominal pain - colicky, sudden onset
- Distension
- Vomiting
- Absolute constipation (failure to pass flatus or stool)
Bailey & Love's and Pye's both emphasise that presentation varies by level and completeness.
Comparison: High SBO vs Low SBO vs LBO
| Feature | High SBO | Low SBO | LBO |
|---|---|---|---|
| Pain | Periumbilical colic | Periumbilical, prominent | Lower abdominal, less severe |
| Vomiting | Early, profuse, causes rapid dehydration | Later | Late feature |
| Distension | Minimal | Pronounced (central) | Early and pronounced (peripheral) |
| Constipation | Less dominant | Prominent | Dominant symptom |
| X-ray | Few dilated loops; paucity of gas distally | Multiple dilated small bowel loops | Dilated colon; small bowel dilated if ileocaecal valve incompetent |
| Fluid loss | Rapid and severe | Progressive | Less acute |
- Bailey & Love's Short Practice of Surgery, 28th Ed.
Strangulation Features
Strangulation must be suspected when:
- Continuous (not colicky) severe pain not controlled with IV opiates
- Fever (indicates ischaemia, perforation, or associated abscess)
- Tachycardia
- Localised tenderness, peritonism, rebound guarding
- Leukocytosis or leukopenia
- Elevated serum K+, amylase, LDH, lactate
Hypothermia indicates septicaemic shock or a neglected/late case. - Bailey & Love
Important: No clinical parameter, combination of parameters, or laboratory/radiographic examination can definitively rule in or rule out strangulation in all cases. - Sabiston Textbook of Surgery
Examination must always include: hernial orifices (inguinal, femoral, umbilical), digital rectal examination, and assessment for previous surgical scars.
Investigations
Blood Tests
- FBC: leukocytosis (strangulation); raised haematocrit (dehydration)
- U&E: hyponatraemia, hypokalaemia, raised urea/creatinine
- ABG: metabolic alkalosis (high SBO from vomiting HCl) or acidosis (ischaemia/strangulation)
- Lactate, LDH, amylase, CK - raised values suggest ischaemia but are not diagnostic
Imaging
Plain abdominal X-ray (supine + erect)
- Most common initial imaging
- Erect: multiple air-fluid levels
- Supine: identifies the type of distended bowel:
- Small bowel: valvulae conniventes (plicae semilunares) traverse the entire width of bowel, are parallel and close together
- Colon: haustra are further apart and do not traverse the full width of the bowel
- Specific findings: sigmoid volvulus = "coffee bean" sign; caecal volvulus = "comma" or kidney-shaped distended caecum displaced to left
CT Abdomen (gold standard)
- Identifies the level and cause of obstruction
- Transition zone
- Signs of strangulation: bowel wall thickening >3 mm, mesenteric oedema, fluid between loops, decreased bowel wall enhancement, pneumatosis intestinalis, portal venous gas
- Differentiates benign vs malignant obstruction
- CT enteroclysis useful for low-grade/partial SBO
Ultrasound
- Sensitivity ~85% for mechanical obstruction; no radiation; useful bedside tool
Water-soluble contrast studies
- Gastrografin follow-through has therapeutic and diagnostic value in adhesive SBO; passage to colon within 24h predicts resolution of obstruction non-operatively
Management
General Principles: "Drip and Suck"
All patients require:
- IV fluid resuscitation - isotonic solution (Hartmann's/lactated Ringer's or normal saline); add KCl once adequate urine output is established
- Urinary catheter - monitor urine output
- Nasogastric tube (NGT) - decompress the stomach, reduce vomiting and aspiration risk
- Nil by mouth
- Serial electrolytes, haematocrit, WBC
Antibiotics
Broad-spectrum antibiotics are given preoperatively if surgery is required. Routine use is not supported by substantial evidence in non-toxic patients without suspected bacterial overgrowth. - Sabiston
Conservative (Non-Operative) Management
Appropriate for:
- Adhesive SBO without signs of strangulation: a trial of non-operative management for 24-72h with close clinical monitoring
- Paralytic ileus - mainstay of treatment is bowel rest, NGT, IV fluids, correction of underlying cause
- Partial obstruction - usually resolves with conservative treatment
Gastrografin challenge: if contrast reaches the colon within 24h on follow-through, successful non-operative resolution is likely.
Surgical Indications (Urgent/Emergency)
- Signs of strangulation or peritonitis (operate without delay)
- Complete obstruction not resolving
- Closed-loop obstruction or volvulus
- Caecal dilatation >12-14 cm (risk of perforation - surgical emergency) - Harrison's Principles
- Irreducible hernia
Operative Options
- Adhesiolysis - release of obstructing adhesive bands
- Resection and anastomosis (or stoma formation if bowel non-viable or patient unfit)
- Strictureplasty - for Crohn strictures
- Hartmann's procedure - for LBO from sigmoid cancer with perforation/peritonitis
- Sigmoid volvulus: attempted endoscopic decompression with flatus tube first; recurrence rate high without elective sigmoid resection
- Intussusception in children: contrast enema reduction; surgery if mass-led (adults) or if enema fails
Palliative/Malignant Obstruction
- Self-expanding metal stents (SEMS) for colorectal, gastric outlet, duodenal obstruction to palliate without major surgery
- Venting gastrostomy for nausea/vomiting control
- Octreotide to reduce GI secretions and relieve symptoms
- Antiemetics, antispasmodics, analgesics
- Median survival with malignant bowel obstruction: 3-4 months - Harrison's Principles of Internal Medicine, 22nd Ed.
Complications
- Dehydration, hypovolaemic shock
- Electrolyte imbalance
- Aspiration pneumonia
- Bowel ischaemia, infarction, gangrene
- Perforation - peritonitis
- Sepsis, multi-organ failure
- Respiratory embarrassment (diaphragm splinting from distension)
Special Notes
Adynamic (Paralytic) Ileus vs Mechanical Obstruction
Both present with distension, nausea, vomiting, and reduced bowel sounds. Key differentiators:
- Paralytic ileus: absent bowel sounds throughout; gas present throughout the entire GI tract (including colon and rectum) on AXR; no transition point on CT
- Mechanical: high-pitched (tinkling) bowel sounds early; transition point on CT; proximal dilatation with distal collapse
Pseudo-obstruction (Ogilvie Syndrome)
- Massive colonic dilatation without mechanical obstruction, typically in elderly hospitalised patients
- Risk of caecal perforation if caecum >12 cm
- Treatment: neostigmine, colonoscopic decompression
Neonatal Intestinal Obstruction
- Cardinal symptom: bilious emesis - prompt recognition is lifesaving - Schwartz's Principles of Surgery
- Causes: Hirschsprung disease, malrotation/volvulus, duodenal atresia, meconium ileus, anorectal malformations
Sources: Robbins & Kumar Basic Pathology; Bailey & Love's Short Practice of Surgery, 28th Ed.; Sabiston Textbook of Surgery; Pye's Surgical Handicraft, 22nd Ed.; Harrison's Principles of Internal Medicine, 22nd Ed.; Tintinalli's Emergency Medicine; Schwartz's Principles of Surgery.
This is a shared conversation. Sign in to Orris to start your own chat.