I now have all the data needed for a comprehensive, well-sourced response. Let me compile it.
Molecular Markers in Cervical Cancer Screening: A Detailed Overview
Cervical cancer remains largely preventable through effective screening. The paradigm has shifted from pure morphology (Pap smear) to an integrated molecular framework - primary HPV DNA/RNA testing supplemented by a growing panel of triage biomarkers that refine risk stratification, reduce unnecessary colposcopies, and enable precision management.
1. The Biological Rationale
All common cervical cancers are driven by persistent infection with high-risk HPV (hrHPV), predominantly HPV 16 and 18. The oncoproteins E6 and E7 degrade p53 and Rb respectively, deregulating the cell cycle and driving CIN progression to invasive cancer over years to decades. This protracted natural history creates a wide window for molecular detection.
The critical limitation of primary HPV testing is high sensitivity but low specificity - most hrHPV infections are transient and do not progress. The role of molecular markers is therefore to triage HPV-positive women, distinguishing those with true high-grade lesions (CIN2+/CIN3+) requiring immediate colposcopy from those who can safely return to surveillance.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 926
2. Cervical Cytology (Papanicolaou Smear) - The Historical Foundation
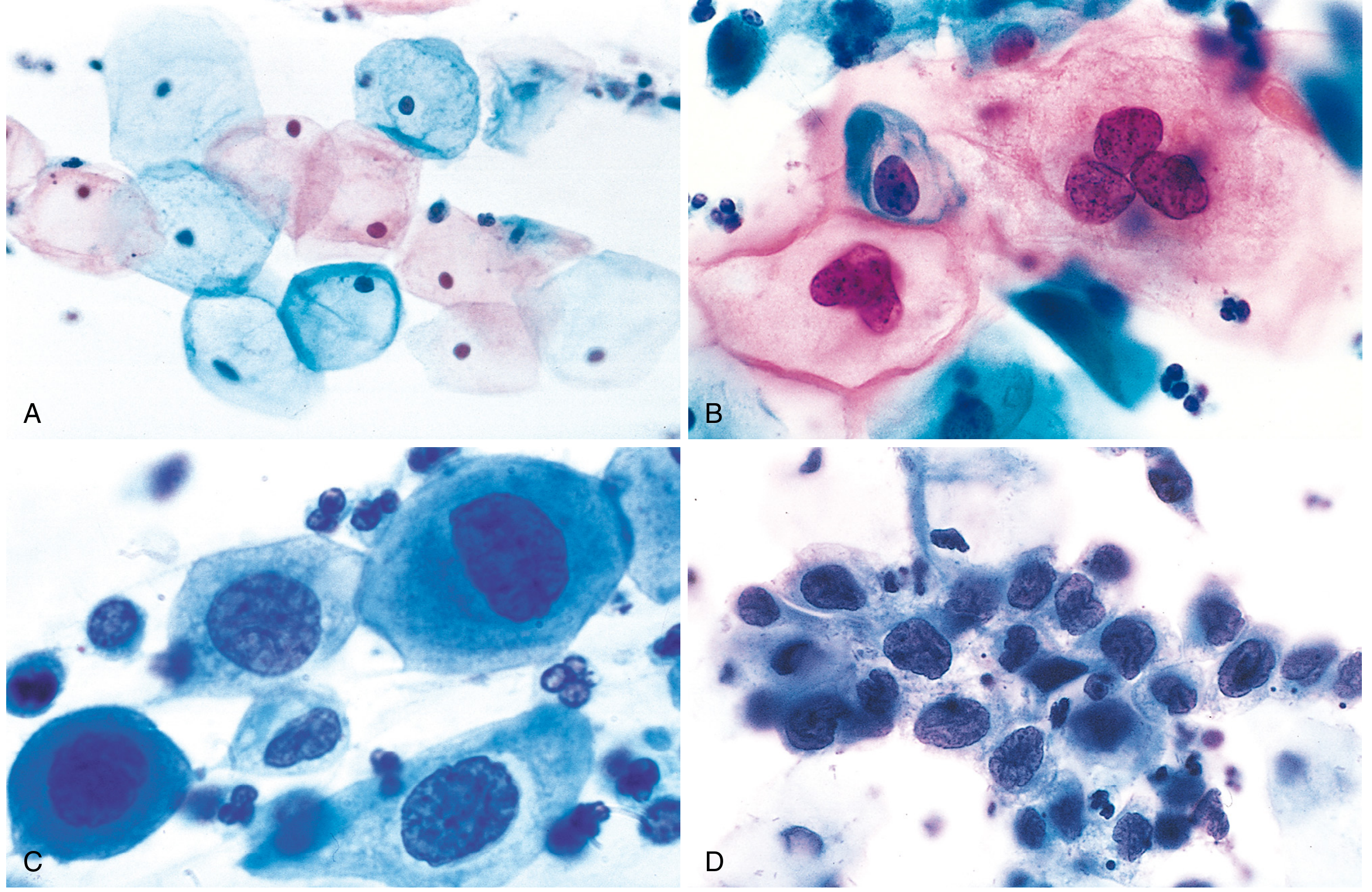
The Pap smear detects cytological evidence of viral cytopathic effect (koilocytes) and intraepithelial lesions. While not a "molecular" marker, it remains the reference comparator.
Fig. Pap smear cytology spectrum: (A) Normal superficial squamous cells, (B) LSIL - koilocytes showing perinuclear halo, (C & D) HSIL - increasing nuclear-to-cytoplasmic ratio with progressive loss of differentiation. (Courtesy Dr. Edmund S. Cibas, Brigham and Women's Hospital) - Robbins Pathology
Key performance: ~55-80% sensitivity, ~90% specificity for CIN2+. Main limitation is inter-observer variability and sampling error.
3. Primary HPV Molecular Testing
3.1 FDA-Approved Assays
| Assay | Molecular Target | Technology | Typing Capability | FDA Indications |
|---|
| Hybrid Capture 2 (HC2) | DNA (genomic) | DNA:RNA hybridization | None | ASC-US triage, Co-test |
| Cervista HPV HR | DNA | Invader technology | HPV 16/18 reflex | ASC-US triage, Co-test |
| Cobas HPV (Roche) | L1 DNA | PCR TaqMan | HPV 16/18 separate | ASC-US triage, Co-test, Primary screening |
| APTIMA HPV (Hologic) | E6/E7 mRNA | TMA | HPV 16/18/45 reflex | ASC-US triage, Co-test |
Source: Berek & Novak's Gynecology, Table 16-2
3.2 HPV DNA vs. HPV mRNA Testing
| Parameter | HPV DNA Testing | HPV E6/E7 mRNA Testing (APTIMA) |
|---|
| Mechanism | Detects viral genome (latent + active infection) | Detects transcriptional activity (oncogenic transformation) |
| Sensitivity for CIN2+ | ~96% | ~87-91% |
| Specificity for CIN2+ | Lower (detects transient infections) | Higher (active oncogenic expression) |
| Clinical utility | Primary screening, co-testing | Triage of HPV+/ASC-US results |
| Key advantage | Very high NPV | Fewer false positives; reflects active disease |
E6/E7 mRNA significance: The E6/E7 oncoproteins are the primary drivers of malignant transformation. Detecting their mRNA (as in APTIMA) rather than mere viral DNA presence more accurately identifies biologically active, transforming infections. Studies show E6/E7 mRNA positivity with NILM cytology has a low but non-negligible CIN2+ risk requiring surveillance.
4. p16^INK4a and p16/Ki-67 Dual Stain - The Most Validated Biomarker
4.1 Mechanism
p16^INK4a is a cyclin-dependent kinase inhibitor encoded by CDKN2A. In normal cervical epithelium, p16 expression is limited. In HPV-transformed cells, the E7 oncoprotein inactivates the Rb protein, which normally represses p16 transcription. The resultant Rb dysfunction causes massive upregulation of p16 as a feedback response - making p16 overexpression a surrogate marker of E7-driven cell cycle deregulation and, therefore, of transforming HPV infection.
Ki-67 is a nuclear protein expressed during all active phases of cell division (G1, S, G2, M). Normally, in stratified squamous epithelium, proliferating cells are confined to the basal layer and would not co-express p16 (which marks differentiated cells in hrHPV infection). Simultaneous p16/Ki-67 co-expression in the same cell indicates aberrant cell cycle progression and is the hallmark of high-grade transformation.
4.2 Clinical Performance (PALMS Study - Key Validation Data)
The landmark PALMS trial (n = 27,349 women) provided prospective validation:
| Metric | p16/Ki-67 Dual Stain | Cytology |
|---|
| Sensitivity for CIN2+ | 86.7% | 68.5% |
| Specificity for CIN2+ | 95.2% | 95.4% |
| p-value (sensitivity) | p < 0.001 (DS superior) | - |
| p-value (specificity) | p = 0.15 (not significant) | - |
Source: Integrating Biomarkers into Cervical Cancer Screening (PMC12731993, 2025)
4.3 ASCCP 2024 Recommendations for p16/Ki-67 Dual Stain
The Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee (Clarke MA et al., JLGTD 2024, PMID
38446575) established the following framework using CINtec PLUS Cytology:
| HPV Result | DS Result | HPV Genotype | Recommended Action |
|---|
| HPV positive | DS positive | Any genotype | Immediate colposcopy |
| HPV positive | DS negative | HPV 16 or 18 | Immediate colposcopy (genotype overrides DS) |
| HPV positive | DS negative | Other hrHPV | 1-year follow-up with HPV-based testing |
| Co-test positive | DS positive | Any | Immediate colposcopy |
| Co-test positive | DS negative | + High-grade cytology (ASC-H/HSIL) | Immediate colposcopy |
Key finding: DS requires fewer colposcopies than cytology while detecting CIN3+ earlier. Risk estimates were portable between Kaiser Permanente Northern California and Mississippi populations.
5. HPV Extended Genotyping
HPV 16 and 18 carry disproportionately high cancer risk:
- HPV 16 accounts for ~50-60% of all cervical cancers
- HPV 18 accounts for ~10-15%
- Together they represent the highest-risk genotypes
ASCCP 2025 extended genotyping guidance (Massad et al., JLGTD 2025) further refines this by stratifying individual genotypes (HPV 31, 33, 45, 52, 58 etc.) into risk tiers, guiding management thresholds. HPV 16-positive women are at sufficient risk to warrant colposcopy regardless of DS result.
6. DNA Methylation Markers
Epigenetic silencing of tumor suppressor genes via DNA methylation is an early event in cervical carcinogenesis and represents perhaps the most promising next-generation triage strategy.
6.1 Mechanism
As HPV-infected cells progress toward malignancy, host genes involved in cell adhesion, differentiation, and apoptosis become aberrantly methylated at CpG islands in their promoters. This is a host-cell response to transforming HPV infection, distinct from viral markers.
6.2 Key Methylation Targets
| Gene/Panel | Expression Change in CIN/Cancer | Notes |
|---|
| FAM19A4/miR124-2 | Methylated (silenced) | Most studied; strong correlation with CIN3+; validated in GynTect® assay |
| CADM1 | Methylated | Cell adhesion molecule; early epigenetic event |
| MAL | Methylated | Detected in CIN2+ lesions |
| PAX1 | Methylated | High AUC (0.89) for cervical cancer; sensitivity 87%, specificity 75% (meta-analysis, PMID 41229153) |
| ZNF582 | Methylated | Correlated with lesion severity; co-expression with p16/Ki-67 |
| CDKN2A (p16) | Paradoxically overexpressed | Used as IHC marker (see above) |
6.3 Pooled Performance (Systematic Review, PMID 37533074, n = 23 studies)
| Endpoint | Pooled Sensitivity | Pooled Specificity | PPV | NPV |
|---|
| CIN2+ detection | 0.68 (95% CI: 0.63-0.72) | 0.75 (95% CI: 0.71-0.80) | 51.4% | 85.7% |
| CIN3+ detection | 0.78 (95% CI: 0.74-0.82) | 0.74 (95% CI: 0.69-0.78) | 39.2% | 93.8% |
Clinical implication: The very high NPV for CIN3+ (93.8%) makes methylation markers excellent for ruling out high-grade disease in HPV-positive women, potentially obviating unnecessary colposcopy referral. The GynTect® (FAM19A4/miR124-2) assay further reduces unnecessary colposcopies and is compatible with self-sampling.
7. Serum and Circulating Tumor Markers
7.1 Squamous Cell Carcinoma Antigen (SCC-Ag)
- A serine protease inhibitor overexpressed in squamous cell carcinoma of the cervix
- Not used for primary screening (low sensitivity for early disease)
- Established role in monitoring treatment response and recurrence surveillance
- Emerging data: optimal cutoffs in combination with HPV metrics, methylation markers, and ctDNA improve early recurrence detection and personalize follow-up (PMC12731993, 2025)
7.2 Circulating Tumor DNA (ctDNA) / HPV-ctDNA
Liquid biopsy approaches detect:
- HPV circulating tumor DNA (HPV-ctDNA): fragments of HPV DNA shed from tumor cells into circulation
- Host-gene aberrations: copy number variations, somatic mutations in PI3K pathway, KRAS, TP53
| Application | Evidence Status | Key Data |
|---|
| Primary screening | Experimental | Insufficient sensitivity in precancer; blood-based HPV-ctDNA detectable mainly in invasive cancers |
| Residual disease after chemoradiation | Validated (multicenter, PMID 37972346) | High accuracy for detecting residual cervical cancer post-CRT |
| Recurrence monitoring | Promising | Earlier detection than imaging |
| Triage of HPV-positive women | Investigational | Not yet clinically implemented |
7.3 Other Tumor Markers
| Marker | Role | Notes |
|---|
| CEA | Non-specific; not useful for screening | Elevated in advanced adenocarcinoma |
| CA-125 | Adenocarcinoma of cervix | Not specific; more relevant in endometrial/ovarian disease |
| CYFRA 21-1 | Squamous cell type | Promising prognostic marker; not a screening tool |
8. Emerging and Investigational Markers
| Marker Category | Examples | Mechanism | Stage |
|---|
| microRNA panels | miR-21, miR-155, miR-218 | Post-transcriptional regulation altered by HPV | Investigational |
| Long non-coding RNA (lncRNA) | HOTAIR, MALAT1 | Chromatin remodeling, oncogenic signaling | Preclinical/early clinical |
| MCM2 (Mini-Chromosome Maintenance) | MCM2 IHC | DNA replication licensing; marks proliferating cells | Studied alongside p16/Ki-67 |
| ProExC (MCM2 + TOP2A) | ProExC assay | Cell cycle deregulation | Used in some cytology labs |
| Proteomics / multi-analyte panels | SCC-Ag + methylation + ctDNA | Composite risk scores | Early validation |
| HPV viral load | Quantitative hrHPV | Higher load correlates with lesion severity | Not yet clinically standardized |
9. Current Screening Algorithms - How Markers Are Integrated
USPSTF 2024 Draft Recommendation (USA)
| Age Group | Preferred Strategy | Acceptable Alternatives |
|---|
| 21-29 years | Cytology alone every 3 years | None |
| 30-65 years | Primary hrHPV testing every 5 years (clinician OR patient-collected) | Co-testing (HPV + cytology) every 5 years; cytology alone every 3 years |
| >65 years | Discontinue if adequate negative history | - |
Historic change (2024): Primary HPV testing every 5 years is now the preferred strategy for ages 30-65, and patient (self)-collected samples are formally recognized.
ASCCP Triage Algorithm (2024-2025)
Primary HPV Test
|
├── HPV Negative → Routine screening interval (5 years if primary HPV)
│
└── HPV Positive
|
├── HPV 16 or 18 → COLPOSCOPY (regardless of other results)
│
└── Other hrHPV
|
├── Option A: Reflex Cytology
│ ├── NILM → 1-year retest
│ └── ASC-US+ → Colposcopy
│
├── Option B: p16/Ki-67 Dual Stain
│ ├── DS+ → Colposcopy
│ └── DS- → 1-year HPV-based retest
│
└── Option C: Extended Genotyping (HPV 31/33/45/52/58)
├── High-risk genotype → Colposcopy
└── Lower-risk genotype → Surveillance
Italian Multisocietal Guideline 2025 (GRADE-Based)
- Risk-based thresholds defined using CIN3+ as surrogate cancer risk marker
- Conditional recommendation (GRADE): Combination of morphological markers (cytology or p16/Ki-67) combined with extended HPV genotyping was the only strategy with a positive recommendation versus cytology alone
- Three-tier management: immediate colposcopy / 1-year retest / 3-year retest - driven by CIN3+ risk probability
10. Comparative Summary of Molecular Markers
| Marker | Clinical Role | Sensitivity (CIN2+/3+) | Specificity | Stage of Validation | Guideline Status |
|---|
| HPV DNA (primary) | Screening | ~96% | Moderate | Routine clinical use | USPSTF preferred (30-65) |
| HPV E6/E7 mRNA | Triage / primary | ~87-91% | Higher than DNA | FDA-approved (APTIMA) | ASC-US triage, co-test |
| p16^INK4a IHC | Histopathology adjunct | High | High | Routine histology | Standard pathology practice |
| p16/Ki-67 Dual Stain | Triage of HPV+ | 86.7% (vs 68.5% cytology) | 95.2% | FDA-approved (CINtec PLUS) | ASCCP 2024 guideline |
| DNA methylation (FAM19A4/miR124-2) | Triage of HPV+ | 68-78% | 74-75% | Validated (GynTect® assay) | European guidelines; not yet US guideline |
| PAX1 methylation | Triage / risk stratification | 87% | 75% | Meta-analysis validated | Research/Asian populations |
| HPV genotyping (16/18 vs others) | Risk stratification | Reflex | High | FDA-approved | ASCCP 2024/2025 |
| SCC-Ag | Monitoring / prognosis | Low for early disease | Moderate | Routine clinical use | Not for primary screening |
| ctDNA / HPV-ctDNA | Post-treatment monitoring | Moderate (invasive only) | High | Early clinical validation | Not recommended for screening |
| microRNA / lncRNA | Screening / prognosis | Investigational | Investigational | Preclinical/early trials | Not in guidelines |
11. Special Considerations
Self-Sampling (ASCCP April 2025)
- Self-collected vaginal samples for hrHPV testing formally endorsed in clinical settings
- Performance equivalent to clinician-collected for HPV DNA detection
- Greatly improves access; molecular markers (DS, methylation) compatible with self-collected LBC samples
Low-Resource Settings
- p16^INK4a single-stain IHC on conventional smears offers a cost-effective alternative to dual stain
- HPV DNA testing with visual triage (VIA + p16) being evaluated by WHO for low-income countries
- GeneXpert (point-of-care HPV testing) increasingly deployed
HPV-Independent Cervical Cancer
- Approximately 5% of cervical cancers are hrHPV-negative
- Driven by KRAS mutations, ERBB2 amplification, or chromosomal instability
- Standard HPV-based screening will miss these; no established molecular screening strategy yet
- Represents an important gap recognized in 2024-2025 literature
Key Takeaways
- Primary hrHPV testing is now the preferred first-line molecular screening strategy for women aged 30-65 (USPSTF 2024 preferred; primary HPV testing every 5 years).
- p16/Ki-67 dual stain is the most clinically validated triage biomarker for HPV-positive women, now with formal ASCCP 2024 recommendations. It reduces unnecessary colposcopies while maintaining sensitivity.
- Extended HPV genotyping enables precise risk stratification - HPV 16 or 18 warrants immediate colposcopy regardless of other results.
- DNA methylation markers (especially FAM19A4/miR124-2 and PAX1) show excellent NPV for CIN3+, making them ideal to rule out high-grade disease and avoid overtreatment. Italian 2025 guidelines give conditional GRADE recommendation for combined biomarker + genotyping strategy.
- ctDNA and liquid biopsy approaches remain investigational for screening but are validated for post-treatment monitoring.
- The overarching goal is a risk-stratified, individualized approach - not universal colposcopy referral for HPV positivity.
Key References: