Heart failure drugs used in pregnancy and lactation
Reading File
Finding Sources
Finding Sources
Searching PubMed
heart failure treatment pregnancy
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information to construct a detailed answer. Let me compile everything into a well-organized response.
Heart Failure Drugs in Pregnancy and Lactation
Managing heart failure (HF) in pregnancy requires a careful balance between maternal benefit and fetal/neonatal safety. Drug choices differ depending on whether the patient is antepartum (still pregnant) vs. postpartum/lactating. Most cardiac drugs cross the placenta; dose should always be the lowest effective.
Key Principle: Pregnancy vs. Lactation Safety Can Differ
"Some medications (ACE inhibitors) that are contraindicated during pregnancy can be used during lactation." - Braunwald's Heart Disease
Drug safety in breastfeeding depends on the concentration in breast milk, which may differ substantially from placental transfer.
SAFE / PREFERRED Drugs in Pregnancy
1. Diuretics
- Furosemide (loop diuretic): Used for pulmonary congestion and volume overload; preferred for acute decompensation. Crosses the placenta but generally considered safe in short-term use. May cause fetal electrolyte disturbances and neonatal diuresis if used chronically.
- Hydrochlorothiazide: Can be used but may cause neonatal thrombocytopenia, hyponatremia.
- Spironolactone / Eplerenone (aldosterone antagonists): CONTRAINDICATED in pregnancy - anti-androgenic effects in first trimester, risk of feminization of male fetus. Not recommended for lactation either.
2. Beta-Blockers
- Metoprolol, carvedilol, labetalol: Generally considered safer beta-blockers. Labetalol is first-line for hypertension in pregnancy; metoprolol/carvedilol used in HF with reduced ejection fraction. May cause fetal/neonatal bradycardia, hypoglycemia, and growth restriction (small mean weight reduction ~191 g).
- Atenolol: CONTRAINDICATED - highest risk of fetal growth restriction among beta-blockers; avoid especially in the first trimester.
- Note: Doses may need to be increased during pregnancy due to higher volume of distribution.
- In lactation: All major beta-blockers are excreted in breast milk; metoprolol considered safest (lowest milk:plasma ratio).
3. Hydralazine
- Safe and preferred for afterload reduction during pregnancy (used for both hypertension and heart failure).
- Side effects: lupus-like syndrome, reflex tachycardia, thrombocytopenia.
- Crosses the placenta; compatible with breastfeeding.
4. Nitrates (Isosorbide dinitrate, nitroglycerine)
- Used for preload reduction and acute HF.
- Isosorbide dinitrate: animal studies show some adverse effects; limited human data - used for hypertension and HF.
- IV nitroglycerine: used in acute hypertensive emergencies during pregnancy.
- Nitroprusside: Causes fetal cyanide and thiocyanate toxicity - use only in life-threatening emergencies when alternatives have failed.
5. Digoxin
- Does not have teratogenic effects; considered generally safe in pregnancy and lactation.
- Used for rate control in atrial fibrillation and as positive inotrope in HF.
- Therapeutic monitoring required; pharmacokinetics altered in pregnancy.
- Excreted in breast milk in small amounts - compatible with breastfeeding.
6. Calcium Channel Blockers
- Nifedipine (extended-release): First-line antihypertensive in pregnancy; used in HF with preserved EF. Compatible with breastfeeding.
- Non-dihydropyridines (verapamil, diltiazem): Used for rate control; limited data but generally acceptable.
CONTRAINDICATED Drugs in Pregnancy
| Drug | Reason for Contraindication |
|---|---|
| ACE inhibitors (enalapril, lisinopril, etc.) | Fetal nephrotoxicity in 2nd/3rd trimester, renal tubular dysgenesis, oligohydramnios, lung hypoplasia, skeletal malformations, neonatal renal failure |
| ARBs (losartan, valsartan, etc.) | Same fetal nephrotoxicity as ACEi; 2nd trimester exposure especially dangerous |
| ARNI (sacubitril-valsartan) | Contraindicated - same as ARBs plus insufficient safety data |
| Atenolol | Highest risk of fetal growth restriction among beta-blockers |
| Spironolactone / Eplerenone | Anti-androgenic; risk of feminization of male fetus in 1st trimester |
| Statins | Potential teratogenicity (though data evolving); currently contraindicated |
| Direct oral anticoagulants (DOACs) | Insufficient safety data; contraindicated |
| Warfarin | Warfarin embryopathy at 6-12 weeks; skeletal and CNS malformations (especially >5 mg/day) |
| Amiodarone | Fetal hypothyroidism, neurodevelopmental abnormalities; reserve for emergencies only |
| Bosentan (endothelin receptor antagonist) | Mandibular malformations, cardiac defects |
Drugs Available in Postpartum / Lactation (After Delivery)
Once delivery occurs, most standard HF therapies can be reintroduced:
| Drug | Lactation Status |
|---|---|
| ACEi (enalapril, captopril) | Can be restarted postpartum - low transfer to breast milk; captopril and enalapril preferred |
| ARBs | Limited data; generally not recommended during breastfeeding |
| Metoprolol | Compatible with breastfeeding (preferred beta-blocker) |
| Furosemide | Compatible; may reduce milk production at high doses |
| Hydralazine | Compatible with breastfeeding |
| Digoxin | Compatible |
| Warfarin | Compatible - negligible transfer to breast milk |
| Heparin (UFH/LMWH) | Not excreted in breast milk - safe |
| Spironolactone/Eplerenone | Not recommended for lactation |
| Nifedipine | Compatible |
Special Case: Peripartum Cardiomyopathy (PPCM)
PPCM is the most common HF scenario in pregnancy. Drug management follows general HF guidelines with pregnancy-specific modifications:
During pregnancy:
- Diuretics for congestion (furosemide)
- Hydralazine + nitrates (substitute for ACEi/ARBs)
- Beta-blockers (metoprolol, carvedilol - avoiding atenolol)
- Digoxin as adjunct
- Anticoagulation (LMWH/UFH preferred - do not cross placenta) due to high thromboembolic risk; continue until LVEF >35%
After delivery:
- Switch to full evidence-based HF regimen: ACEi/ARB + beta-blocker + MRA + ARNI if tolerated
- Anticoagulation with warfarin acceptable postpartum (compatible with breastfeeding)
Bromocriptine (unique to PPCM):
- Mechanism: inhibits prolactin, blocking conversion to the antiangiogenic 16-kDa form thought to cause PPCM
- Two small African studies showed benefit; a small German RCT was inconclusive
- European guidelines give a Class IIb recommendation; not routinely used in the US
- Requires concurrent anticoagulation due to thromboembolic risk
- Inhibits milk production (breastfeeding is not contraindicated in stable patients without bromocriptine)
Summary Table: HF Drugs - Pregnancy vs. Lactation
| Drug Class | Pregnancy | Lactation |
|---|---|---|
| Loop diuretics | Use with caution (short-term OK) | Compatible |
| Thiazide diuretics | Use with caution | Compatible |
| Aldosterone antagonists | Contraindicated | Not recommended |
| Beta-blockers (metoprolol, carvedilol) | Safe (monitor fetus) | Compatible |
| Atenolol | Contraindicated | Acceptable |
| ACE inhibitors | Contraindicated | Compatible (restart postpartum) |
| ARBs | Contraindicated | Not recommended |
| ARNI | Contraindicated | Avoid |
| Hydralazine | Safe/preferred | Compatible |
| Nitrates | Acceptable | Limited data |
| Digoxin | Safe | Compatible |
| Calcium channel blockers | Safe (nifedipine preferred) | Compatible |
| Warfarin | Avoid (esp. 6-12 wks) | Compatible |
| UFH/LMWH | Safe (does not cross placenta) | Safe |
| DOACs | Contraindicated | Avoid |
| Amiodarone | Emergency use only | Avoid (long half-life) |
| Statins | Contraindicated | Avoid |
| Bromocriptine | Not in pregnancy | Used in PPCM (suppresses lactation) |
Key References:
- Braunwald's Heart Disease 12th ed., Ch. 92 - "Cardiovascular Disease in Pregnancy" (Braunwald's Heart Disease, pp. 1068-1069)
- Fuster and Hurst's The Heart 15th ed., Table 27-2 and Ch. 78 (Fuster and Hurst's The Heart, pp. 2211-2212)
- Fuster and Hurst's The Heart, 15th ed., Ch. 51 - "Peripartum Cardiomyopathy" (p. 1582-1584)
Can you give drugs that are used for treatment of heart failure in pregnancy and lactation. Give the drugs doses need to adjusted and suggest whether dose reduction is required
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
heart failure drugs dose adjustment pregnancy lactation furosemide digoxin beta blocker hydralazine pharmacokinetics
Reading Web Page
https://www.acc.org/latest-in-cardiology/articles/2026/05/04…
Loading Image
I now have comprehensive data from Braunwald's, Fuster & Hurst, the ACC 2026 article, and the safety classification figure. Here is the complete answer:
Heart Failure Drugs in Pregnancy & Lactation: With Dose Adjustments
Why Pharmacokinetics Change in Pregnancy
Pregnancy causes multiple physiological shifts that alter drug behavior:
- Increased plasma volume (40-50%) → dilutes drug concentration → larger volume of distribution
- Increased GFR (50% above baseline) → faster renal clearance of renally-eliminated drugs
- Altered hepatic metabolism → changes CYP enzyme activity
- Reduced plasma albumin → more free drug for protein-bound agents
- Delayed gastric emptying → altered oral absorption
The net result is that many drugs require dose increases during pregnancy to maintain therapeutic effect. After delivery, these changes reverse and doses often need to be reduced back.
Safety Classification Chart (Braunwald's Heart Disease)
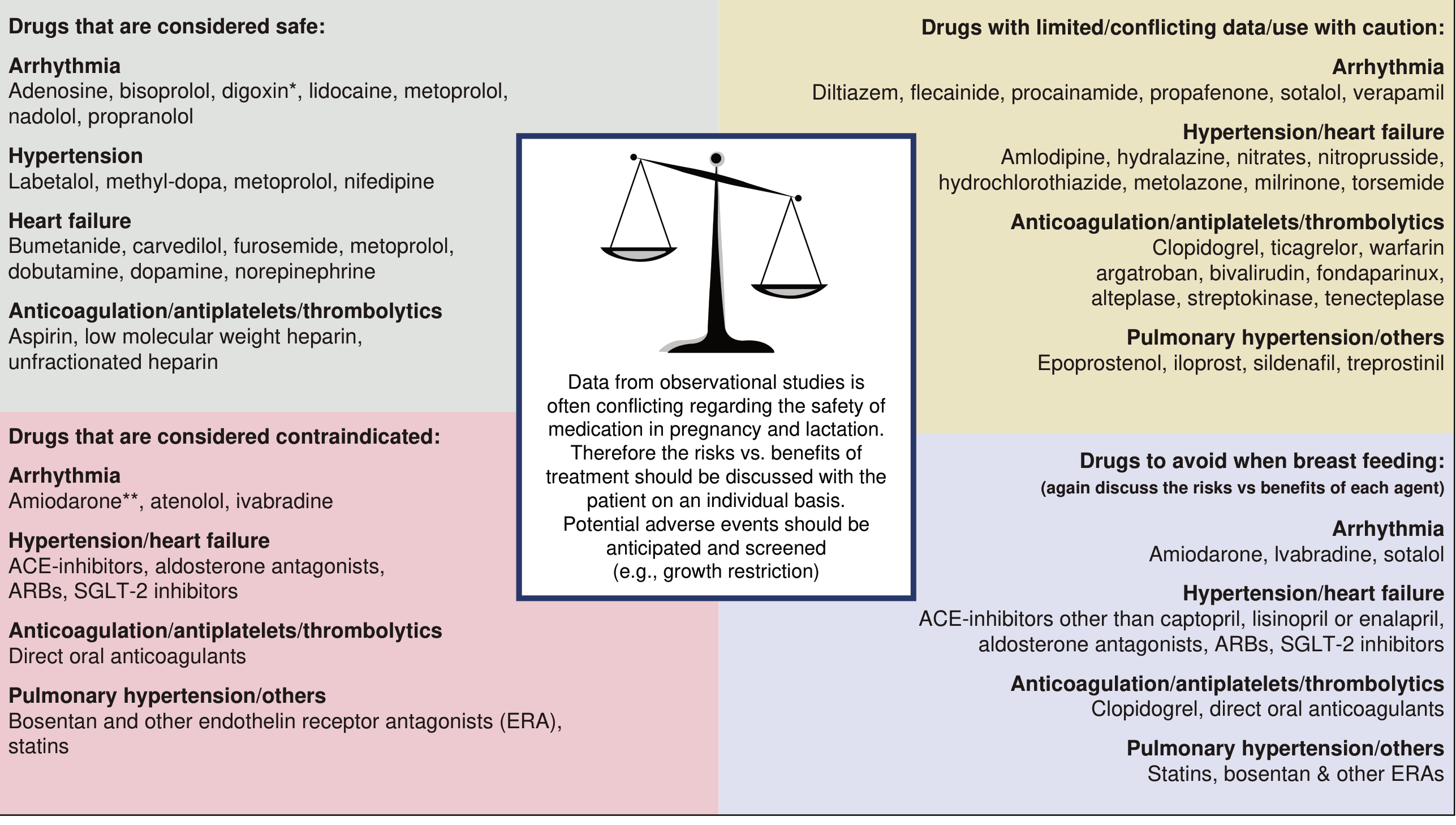
Source: Braunwald's Heart Disease, 12th ed., Fig. 92.5
Drugs USED for Heart Failure in Pregnancy - With Dose Guidance
1. Loop Diuretics (Furosemide, Bumetanide)
| Parameter | Details |
|---|---|
| Use | Pulmonary congestion, volume overload - first-line for symptomatic relief |
| Safety | Safe (Braunwald's/Fuster: listed under "considered safe" for HF) |
| Dose | Furosemide: 20-80 mg oral/IV; titrate to clinical response |
| Dose adjustment needed? | Yes - monitor carefully. Pregnancy increases GFR, so renal clearance of furosemide increases - may need higher or more frequent doses. However, over-diuresis risks placental hypoperfusion. Use the lowest effective dose. |
| Lactation | Compatible; high doses may reduce breast milk production - monitor |
2. Beta-Blockers (Metoprolol, Carvedilol, Labetalol)
| Parameter | Details |
|---|---|
| Use | HFrEF cornerstone; rate control; anti-remodeling |
| Safety | Safe (metoprolol, carvedilol, labetalol, propranolol - all preferred over atenolol) |
| Dose | Metoprolol succinate: start 12.5-25 mg once daily, target up to 200 mg/day; Carvedilol: start 3.125 mg twice daily, target 25-50 mg twice daily |
| Dose adjustment needed? | Yes - dose INCREASE often required. Braunwald's explicitly states: "The doses of some medications, such as beta blockers, may need to be increased during pregnancy to achieve heart rate or BP control" due to increased plasma volume and altered pharmacokinetics. After delivery, doses often need to be reduced. |
| Lactation | Compatible. Metoprolol has the lowest milk:plasma ratio among beta-blockers - preferred during breastfeeding |
Atenolol: CONTRAINDICATED - highest risk of fetal growth restriction
3. Hydralazine (Vasodilator)
| Parameter | Details |
|---|---|
| Use | Afterload reduction - preferred ACEi substitute in pregnancy for HFrEF |
| Safety | Use with caution/limited data (Braunwald's fig.); listed as "used for hypertension and heart failure" in Fuster's table |
| Dose | 25-50 mg orally 3-4 times daily; maximum 300 mg/day total |
| Dose adjustment needed? | Monitor and titrate. Pregnancy causes physiological vasodilation (peaks in 2nd trimester) - may need lower doses early in 2nd trimester due to existing vasodilation. Titrate to response. |
| Lactation | Compatible (excreted in breast milk; breastfeeding acceptable) |
4. Isosorbide Dinitrate / Nitrates
| Parameter | Details |
|---|---|
| Use | Preload reduction; used in combination with hydralazine as ACEi substitute |
| Safety | Use with caution (limited data; animal studies showed some adverse effects) |
| Dose | Isosorbide dinitrate: 20-30 mg 3-4 times daily; maximum 120 mg/day |
| Dose adjustment needed? | No specific pregnancy dose adjustment established - titrate to symptoms and BP. Combination hydralazine + isosorbide dinitrate is the standard substitute for ACEi/ARB in pregnancy |
| Lactation | Limited data; generally used with caution |
5. Digoxin
| Parameter | Details |
|---|---|
| Use | Rate control in AF + HF; positive inotropy in systolic HF |
| Safety | Safe (listed explicitly as safe for HF in Braunwald's figure) |
| Dose | 0.125-0.25 mg daily; target serum level 0.5-<0.9 ng/mL |
| Dose adjustment needed? | Yes - CRITICAL monitoring. Braunwald's specifically notes: "Digoxin serum levels are unreliable during pregnancy" due to increased volume of distribution and altered renal clearance. Serum levels do not accurately reflect tissue concentrations in pregnancy. Use lowest effective dose and titrate by clinical response rather than relying solely on serum levels. After delivery, renal clearance normalizes - risk of toxicity increases, so dose should be reduced/re-evaluated |
| Lactation | Compatible (low transfer into breast milk; safe) |
6. IV Inotropes (Dobutamine, Dopamine, Norepinephrine, Milrinone)
| Parameter | Details |
|---|---|
| Use | Acute decompensated HF, cardiogenic shock in pregnancy |
| Safety | Used with caution; Fuster's table: "cardiac resuscitation drugs are used similarly as non-pregnancy state" |
| Dose | Standard cardiogenic shock doses (Dobutamine: 2-20 mcg/kg/min; Milrinone: 0.375-0.75 mcg/kg/min) |
| Dose adjustment needed? | No specific adjustment - titrate to hemodynamic targets. Do not withhold in life-threatening decompensation |
| Lactation | Limited data; generally used for acute settings only |
ACEi: Contraindicated in Pregnancy → Permitted in Lactation
This is a critical distinction:
| Drug | Pregnancy | Lactation |
|---|---|---|
| Enalapril | CONTRAINDICATED (fetal nephrotoxicity, oligohydramnios) | SAFE - restart postpartum |
| Captopril | CONTRAINDICATED | SAFE - preferred ACEi for breastfeeding |
| Benazepril | CONTRAINDICATED | SAFE for breastfeeding |
| Lisinopril, Ramipril, others | CONTRAINDICATED | Avoid - higher milk transfer |
After delivery, transition from hydralazine + nitrates → restart ACEi (captopril or enalapril preferred during breastfeeding).
Timeline: Safe HF Drug Use Across Pregnancy and Breastfeeding
(Based on ACC 2026 Expert Analysis)
| Drug | T1 (Wks 1-13) | T2 (Wks 14-27) | T3 (Wks 28-40) | Breastfeeding |
|---|---|---|---|---|
| Metoprolol / Carvedilol / Labetalol | ✅ Safe | ✅ Safe | ✅ Safe | ✅ Safe |
| Loop diuretics (furosemide) | ✅ Safe | ✅ Safe | ✅ Safe | ✅ (monitor milk) |
| Digoxin | ✅ Safe | ✅ Safe | ✅ Safe | ✅ Safe |
| Bisoprolol | ⚠️ Limited data | ⚠️ Limited data | ⚠️ Limited data | ⚠️ Limited data |
| Hydralazine | ⚠️ Caution | ⚠️ Caution | ⚠️ Caution | ✅ Safe |
| Isosorbide dinitrate | ⚠️ Caution | ⚠️ Caution | ⚠️ Caution | ⚠️ Limited data |
| ACEi (captopril/enalapril) | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ✅ Safe |
| ARBs | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ⚠️ Avoid |
| ARNI (sacubitril-valsartan) | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ❌ Avoid |
| Spironolactone | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ✅ Safe postpartum |
| Eplerenone | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ⚠️ Limited data |
| SGLT2i (dapagliflozin etc.) | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated |
| Ivabradine | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ❌ Avoid |
| DOACs | ❌ Contraindicated | ❌ Contraindicated | ❌ Contraindicated | ❌ Avoid |
| UFH / LMWH | ✅ Safe | ✅ Safe | ✅ Safe | ✅ Safe |
| Warfarin | ❌ Embryopathy risk | ⚠️ Caution | ⚠️ Caution | ✅ Safe |
| Amiodarone | ❌ Emergency only | ❌ Emergency only | ❌ Emergency only | ❌ Avoid |
Dose Adjustment Summary Table
| Drug | Direction of Dose Change in Pregnancy | Reason |
|---|---|---|
| Beta-blockers | Increase (may need higher dose) | Increased plasma volume, higher Vd, enhanced renal/hepatic clearance |
| Digoxin | Use lowest dose; levels unreliable | Serum levels do not accurately reflect tissue concentration; Vd increases |
| Furosemide | Titrate carefully (may need increase) | Increased GFR accelerates renal clearance; but over-diuresis risks placental hypoperfusion |
| Hydralazine | Titrate to response (may decrease early) | Pregnancy itself causes vasodilation in T2; avoid excessive hypotension |
| Isosorbide dinitrate | Standard doses; titrate | No specific data; titrate to symptoms |
| Heparin (UFH/LMWH) | Increase (significant dose increase needed) | Increased Vd and renal clearance; requires frequent monitoring of anti-Xa levels |
Key Clinical Principles (Braunwald's Heart Disease, Ch. 92):
- Use the lowest possible dose for all drugs in pregnancy
- Benefit to mother must always be weighed against fetal risk
- Drug safety during breastfeeding depends on milk concentration, which can differ from placental transfer - these are distinct assessments
- Doses may need re-adjustment after delivery as pregnancy-related pharmacokinetic changes reverse rapidly
Sources:
- Braunwald's Heart Disease 12th ed., pp. 1002-1013 (Ch. 92, Cardiovascular Disease in Pregnancy)
- Fuster and Hurst's The Heart 15th ed., Table 27-2 and Ch. 51 (Peripartum Cardiomyopathy)
- ACC Expert Analysis, May 2026 - HF Medication Recommendations During Pregnancy and Breastfeeding
- 2022 AHA/ACC/HFSA HF Guideline (Table 14 - standard HF drug doses)
This is a shared conversation. Sign in to Orris to start your own chat.