Otoplasty
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of otoplasty drawn from authoritative otolaryngology textbooks.
Otoplasty
Overview
Otoplasty is surgery to correct prominauris (protruding ears), the most common aesthetic auricular deformity. While it carries no physiologic consequence, the psychosocial impact can be severe — studies show 77.8% of men and 55.9% of women seeking otoplasty had been teased. Correction is associated with decreased anxiety and depression and increased self-esteem and quality of life.
Anatomy
The pinna is composed of fibroelastic cartilage covered in very thin skin — closely adherent anteriorly, more loosely attached posteriorly. Key landmarks:
| Structure | Notes |
|---|---|
| Helix / Antihelix | Major prominences; antihelical fold is critical for ear projection |
| Concha (cavum + cymba) | Divided by helical crus; conchal excess drives protrusion |
| Fossa triangularis | Bounded by superior and inferior crura of antihelix |
| Lobule | Fibrofatty tissue, caudal to cartilage |
| Darwin tubercle | Normal vestigial variant at helix tip |
Normal measurements:
- Vertical height: 5.5–6.5 cm; width: 50–60% of length
- Auriculocephalic angle: 20–35° (>30° = protruding)
- Helical rim to mastoid skin: 15–20 mm
- Long axis: posteriorly rotated 15–30°
Vascular supply: Posterior auricular and superficial temporal arteries (external carotid)
Sensory innervation: CN V (auriculotemporal), CN VII, CN X (Arnold nerve), C2–C3 (great auricular, lesser occipital nerves)
Incidence & Timing
- Occurs in ~5% of the population; autosomal dominant with variable penetrance
- The most common underlying defects: insufficient antihelical fold and overdeveloped conchal bowl
- Ideal surgical timing: age 5–6 years (ear is 85–90% of adult size, cartilage has adequate strength; before school to reduce teasing)
Surgical Goals
Correct protrusion, recreate a smooth antihelical fold, avoid disturbance of the postauricular sulcus, and prevent a "plastered-down" or sharp-looking result.
Over 200 techniques have been described, most falling into two broad categories:
1. Cartilage-Sparing Techniques (Suture-Based)
- Reshape the ear by suturing; no cartilage is cut
- Mustardé technique: Permanent horizontal mattress sutures along the scapha to recreate the antihelical fold
- 2–3 sutures through cartilage and anterior perichondrium; placed before final tightening
- Limitation: Does not address conchal bowl; risk of suture exposure
- Furnas technique (conchomastoid sutures): Horizontal mattress sutures anchor the conchal bowl to the mastoid periosteum
- Placed as far posteriorly as possible to avoid narrowing the external auditory canal
- When done first, may eliminate the need for Mustardé sutures
- Advantage: Minimal cartilage damage; easier bilateral symmetry adjustment
- Disadvantage: Higher risk of loss of correction over time
2. Cartilage-Cutting Techniques
- Full- or partial-thickness cartilage injury to reshape the framework
- Techniques: Converse, Farrior, Pitanguy, Stenstrom (anterior scoring)
- Principle: Cartilage bends away from the cut side (Gibson & Davis, 1958)
- Scoring tools: needle, electrocautery, CO₂ laser, diamond file
- Particularly suited for stiff, thick cartilage
- Advantage: Less frequent loss of correction
- Disadvantage: Risk of cartilage irregularities, sharp edges, scarring
Graduated-Approach Otoplasty
A stepwise method addressing each component of the deformity systematically:
- Skin excision: Fusiform postauricular skin excision; scar positioned in sulcus
- Conchal correction (Furnas sutures): 3 horizontal mattress sutures at the fossa triangularis, cavum concha, and cymba concha
- Antihelical correction (Mustardé sutures): 1–3 sutures placed after simulating the desired fold manually; rasping/scoring reserved for stiff cartilage
- Refinements as needed: Scaphal reduction, helical trimming, lobe reduction, wedge resection (Fig. 28.5)
Incisionless Otoplasty
First described by Fritsch: suture material placed percutaneously without incisions — knots buried subcutaneously.
- 22-gauge needle used to percutaneously score the future antihelical fold
- Mustardé-type sutures placed via transcartilagenous needle passes (4-0 Ti-Cron or 3-0 Mersilene)
- Can be performed under local or general anesthesia
- Results in minimal disruption and faster recovery
Nonsurgical Otoplasty (Neonatal)
During the neonatal period, auricular cartilage is pliable due to circulating maternal estrogen (dissipates within 6–12 weeks). Options:
| Method | Details |
|---|---|
| Taping/splinting | Effective within first 6 weeks; lop ear, Stahl ear deformities |
| Tissue adhesive | Octyl-2-cyanoacrylate; recreates antihelical fold; sloughs in 1–2 weeks |
| Rigid molding (EarWell) | Anterior conformer + posterior cradle; 2–6 weeks; highest efficacy |
After 6 weeks, nonsurgical methods are generally unsuccessful.
Postoperative Care
- Pressure head dressing for 1 week
- Headband worn nightly for up to 6 weeks
Complications
Early
| Complication | Notes |
|---|---|
| Hematoma (~3%) | Pain is first symptom; drain immediately; higher with cartilage-cutting techniques; can progress to cauliflower ear |
| Infection | Typical pathogens: S. aureus, E. coli, P. aeruginosa |
| Perichondritis | Follows infection/hematoma; requires débridement + IV antibiotics |
| Cartilage necrosis | From infection, hematoma, cautery, or improper dressings |
Late
| Complication | Notes |
|---|---|
| Inadequate correction | Most common overall complication |
| Telephone ear deformity | Upper and lower poles protrude; due to mid-ear overcorrection + helical overcorrection |
| Suture extrusion/granuloma | Braided > monofilament; remove if granuloma forms (delay several months post-op) |
| Keloid/hypertrophic scar | Higher risk in younger and more pigmented patients |
| Hypoesthesia | Greater auricular nerve injury; usually resolves in weeks–months |
| Cold susceptibility | From blood supply disruption; risk of frostbite |
| Patient dissatisfaction | Asymmetry ≤2–3 mm is acceptable; overcorrection better tolerated than undercorrection |
Key Principles Summary
- Cartilage-cutting: fewer recurrences, more irregularities
- Cartilage-sparing: more recurrences, fewer irregularities
- A graduated/stepwise approach combining both when needed yields best long-term results
- Overcorrection is better tolerated than undercorrection
- Preoperative photographs (anterior full face, posterior full head, close-up bilateral ears) are mandatory
Sources: Cummings Otolaryngology Head and Neck Surgery, Ch. 28; K.J. Lee's Essential Otolaryngology, p. 1072
Can you give this answer with images too
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
All images loaded. Here is the full illustrated guide:
Otoplasty
Overview
Otoplasty corrects prominauris (protruding ears) — the most common aesthetic auricular deformity. Though physiologically harmless, the psychosocial impact is significant: 77.8% of men and 55.9% of women seeking surgery had been teased. Correction reduces anxiety, depression, and social problems while improving self-esteem and quality of life.
Anatomy
The pinna is composed of fibroelastic cartilage covered in very thin skin — closely adherent anteriorly, loosely attached posteriorly. Key landmarks: helix, antihelix, concha (cavum + cymba), fossa triangularis, lobule, and Darwin's tubercle (normal vestigial variant).
Normal measurements:
- Auriculocephalic angle: 20–35° (>30° = protruding)
- Helical rim to mastoid: 15–20 mm
- Vertical height: 5.5–6.5 cm; width: 50–60% of length
Blood supply: Posterior auricular + superficial temporal arteries (external carotid)
Innervation: CN V, VII, X; C2–C3 (great auricular, lesser occipital nerves)
Incidence & Pathology
- ~5% of population; autosomal dominant, variable penetrance
- Two most common defects:
- Insufficient antihelical fold
- Overdeveloped conchal bowl
- Ideal surgical timing: age 5–6 years (ear ~85–90% adult size; before school to minimize teasing)
Surgical Goals
Correct protrusion → recreate a smooth antihelical fold → avoid disturbance of the postauricular sulcus → prevent a "plastered-down" or unnaturally sharp result.
Over 200 techniques exist, broadly divided into two categories:
Historical Techniques
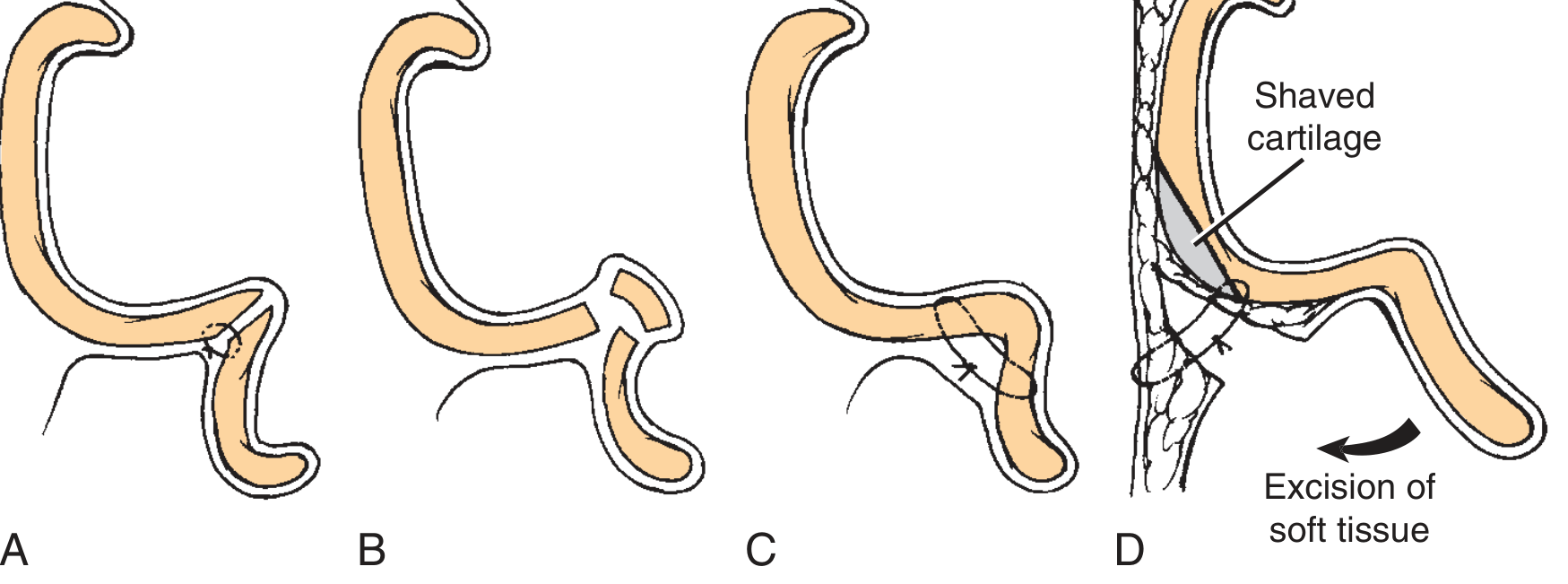
Fig. 28.2 — Historical techniques: (A) Cartilage incision to recreate antihelical fold. (B) Parallel cartilage incisions. (C) Mustardé suture technique. (D) Conchal cartilage shaving with excision of postauricular soft tissues.
Suture Techniques (Cartilage-Sparing)
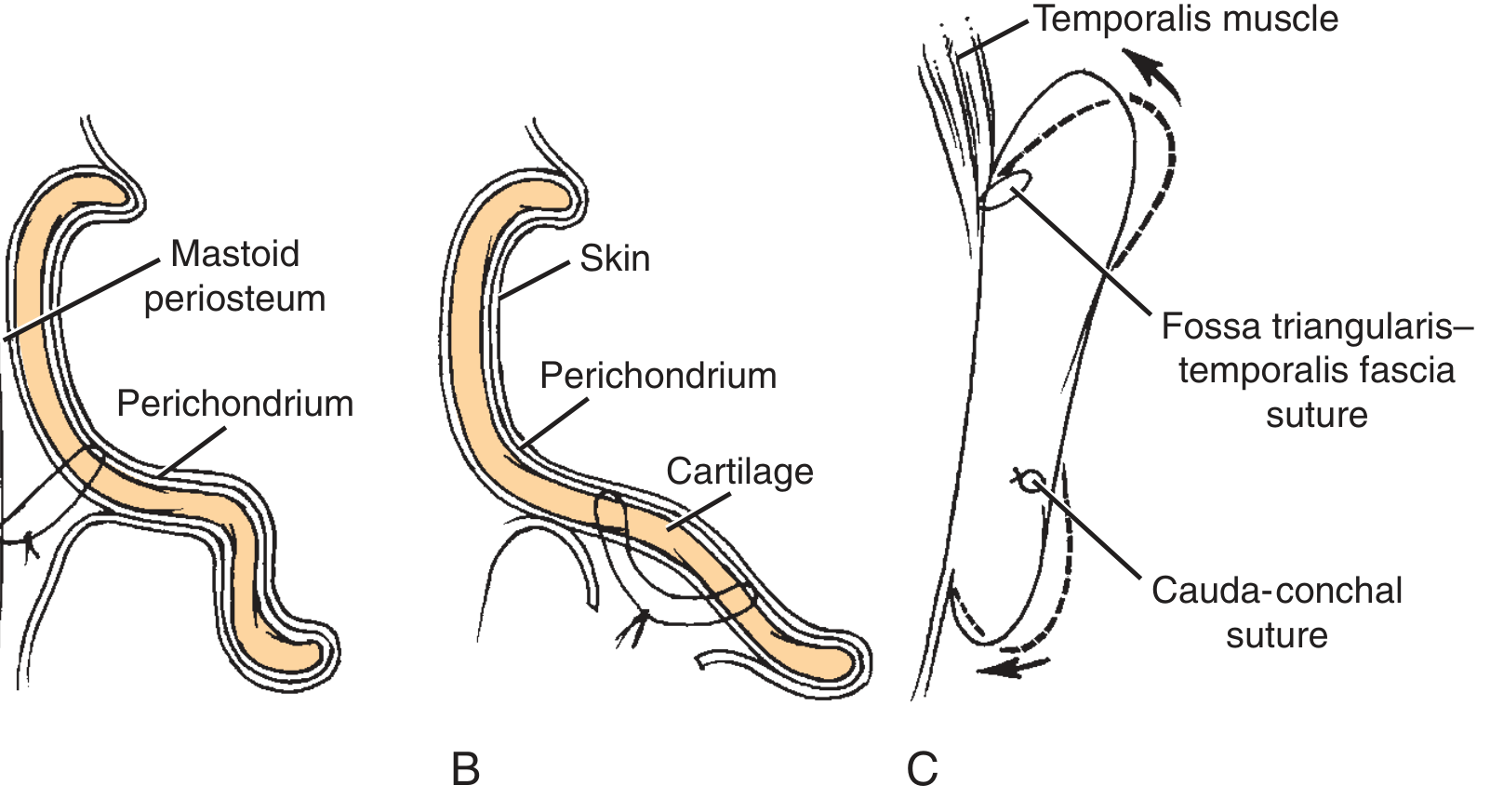
Fig. 28.3 — Suture techniques: (B) Concha-mastoid sutures anchored to mastoid periosteum. (C) Fossa triangularis–temporalis fascia and cauda-conchal sutures.
These techniques reshape without cutting cartilage:
| Technique | Mechanism | Limitation |
|---|---|---|
| Mustardé | 2–3 permanent horizontal mattress sutures along scapha to recreate antihelical fold | Does not address conchal bowl; suture exposure risk |
| Furnas | Horizontal mattress sutures anchor conchal bowl to mastoid periosteum | Risk of narrowing external auditory canal if placed too anteriorly |
- Advantage: Minimal cartilage damage; bilateral symmetry easily adjusted
- Disadvantage: Higher long-term recurrence rate
Cartilage-Cutting Techniques
Full- or partial-thickness injury to reshape the cartilage framework (Converse, Farrior, Pitanguy, Stenstrom).
Key principle (Gibson & Davis, 1958): Cartilage bends away from the cut side.
Scoring tools used: needle, electrocautery, CO₂ laser, diamond file.
- Advantage: Less frequent loss of correction over time
- Disadvantage: Risk of cartilage irregularities, sharp edges, scarring — especially for thin cartilage
Graduated-Approach Otoplasty (Stepwise)
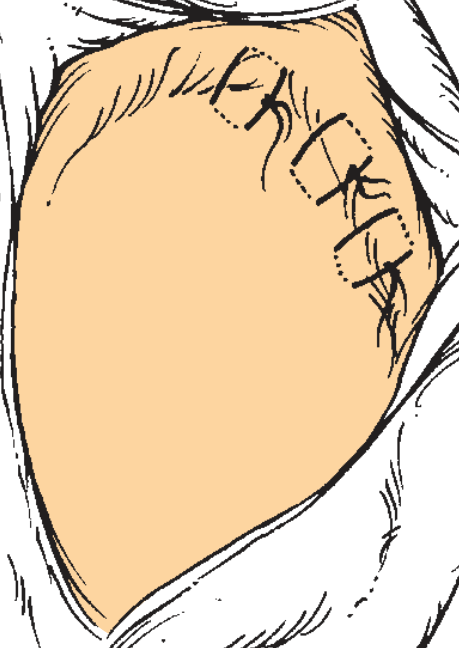
Fig. 28.4 — Scapha-concha (Mustardé) sutures: 1–3 sutures positioned along the antihelical fold.
A systematic stepwise approach addressing each deformity component:
- Postauricular skin excision — fusiform, eccentric toward posterior pinna; scar positioned in sulcus
- Furnas conchal sutures — 3 horizontal mattress sutures at fossa triangularis, cavum concha, cymba concha; avoid excessive overcorrection in middle third (prevents telephone ear)
- Mustardé antihelical sutures — 1–3 sutures after manually simulating desired fold; 4–6 mm bites through cartilage + anterior perichondrium; rasping/scoring reserved for stiff cartilage
- Refinements as needed:
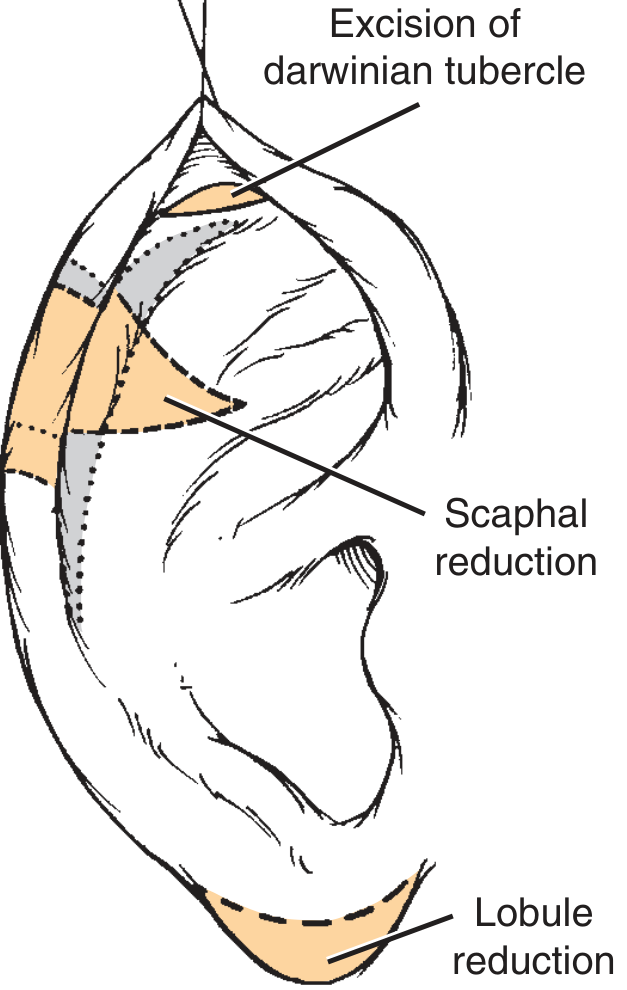
Fig. 28.5 — Refinements: wedge resection, scaphal reduction, excision of Darwin's tubercle, helical trimming, and lobule reduction as required.
Incisionless Otoplasty
First described by Fritsch: no skin incisions — sutures placed entirely percutaneously, knots buried subcutaneously.
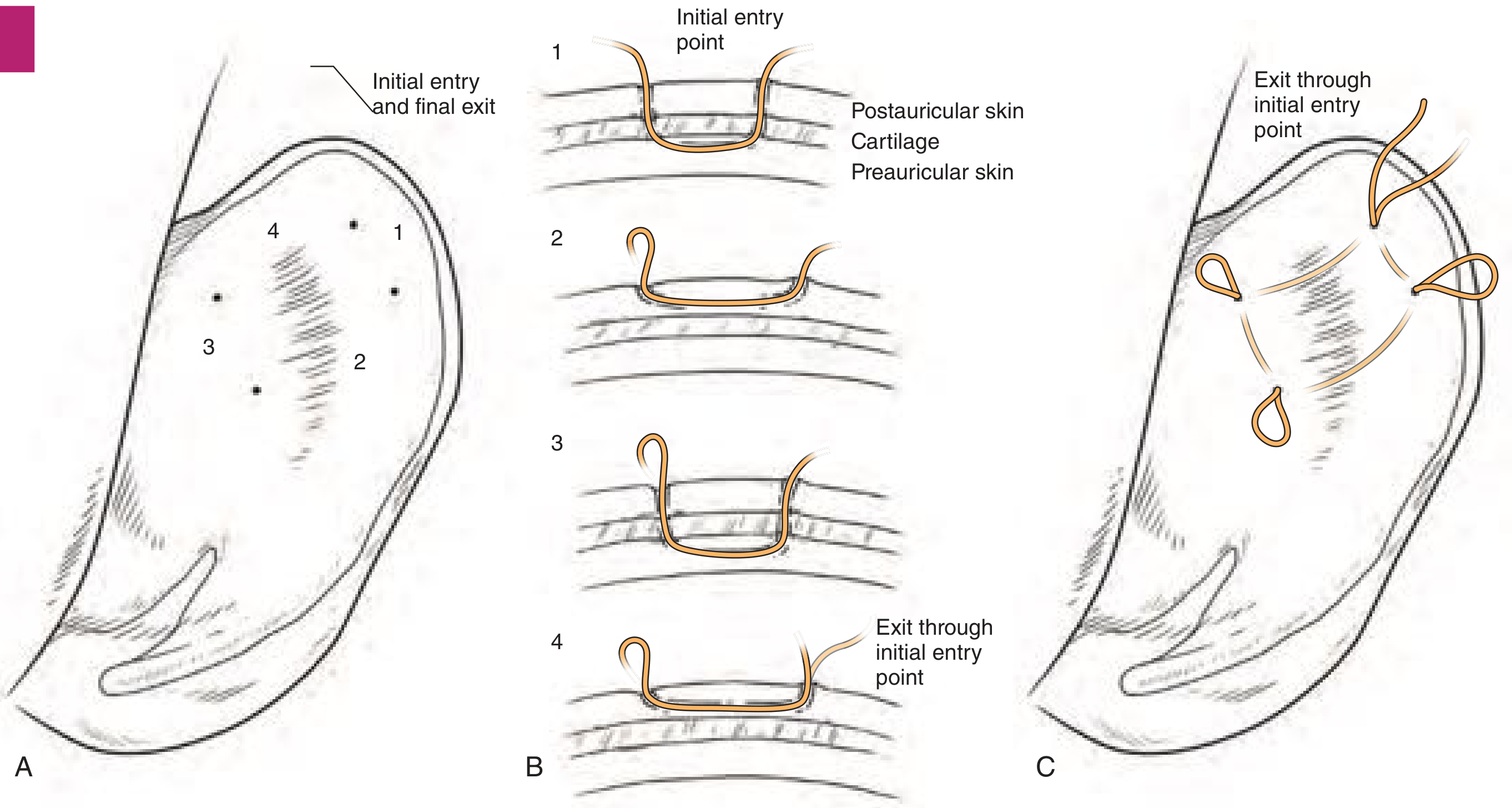
Fig. 28.6 — Incisionless suture loop placement: (A) Entry/exit points on posterior ear. (B) Step-by-step needle passes through cartilage and subperichondrial plane. (C) Multiple suture loops in place.
Technique:
- 22-gauge needle percutaneously scores the future antihelical fold (breaks cartilaginous spring)
- 4-0 Ti-Cron or 3-0 Mersilene sutures passed percutaneously in Mustardé-type horizontal mattress fashion
- Can be performed under local or general anesthesia
- Minimal disruption, faster recovery
Suture Location Summary
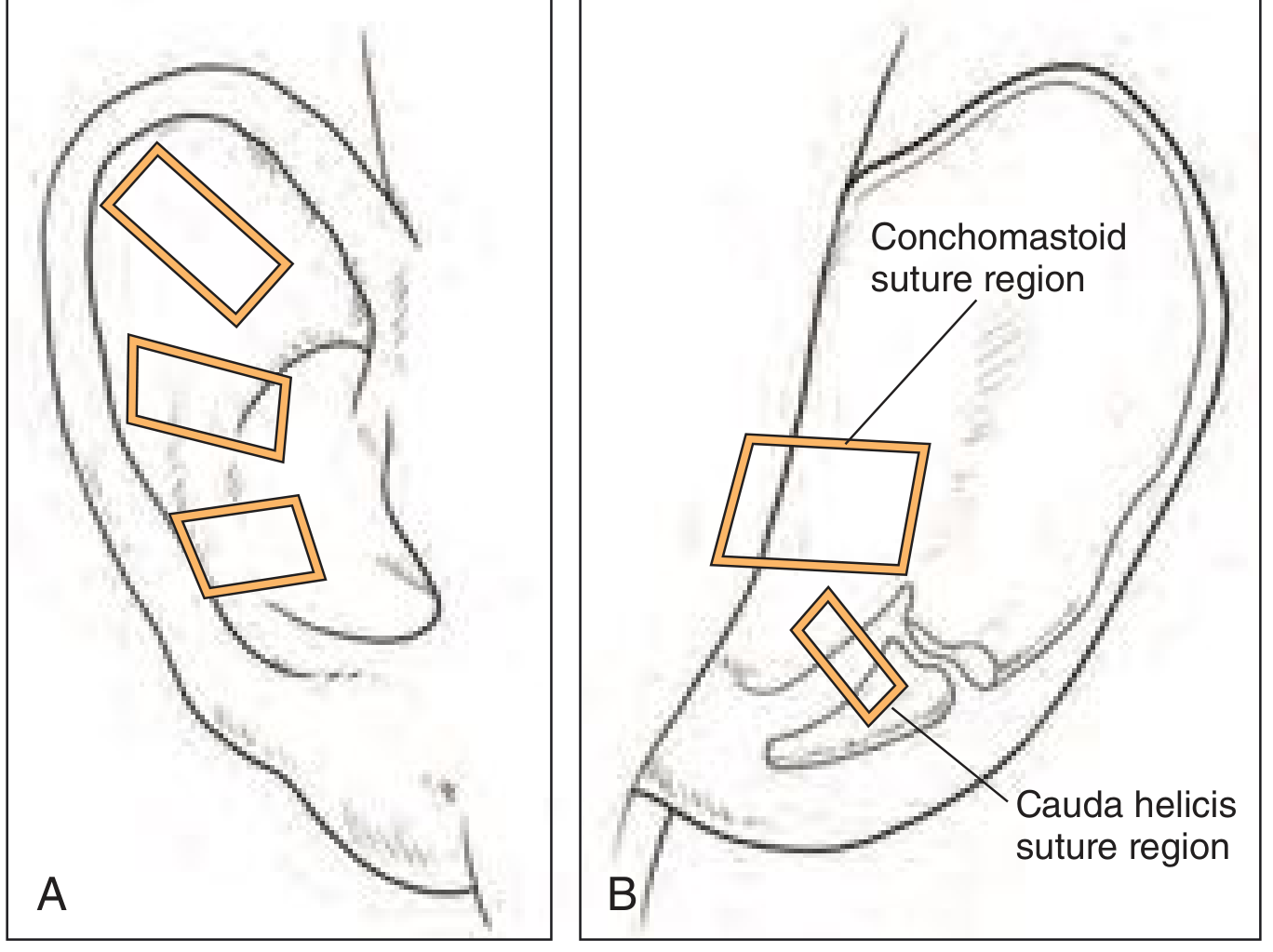
Fig. 28.7 — Suture locations: (A) Three Mustardé-type sutures along the antihelical fold. (B) Conchomastoid and cauda helicis suture regions for Furnas-type correction.
Nonsurgical Otoplasty (Neonatal)
During the neonatal period, auricular cartilage is pliable due to circulating maternal estrogen (dissipates by 6–12 weeks). After this window, nonsurgical methods are ineffective.
| Method | Notes |
|---|---|
| Taping/splinting | Wire-in-silicone tube or thermoplastic splints; 4–6 weeks; for lop ear, Stahl ear |
| Tissue adhesive | Octyl-2-cyanoacrylate; recreates fold + secures ear to mastoid; sloughs in 1–2 weeks |
| Rigid molding (EarWell) | Anterior conformer + posterior cradle; highest efficacy; effective even in 2 weeks if started early in nursery |
Postoperative Care
- Pressure head dressing for 1 week
- Headband worn at night for up to 6 weeks
Complications
Early
| Complication | Notes |
|---|---|
| Hematoma (~3%) | Pain is the first sign; drain immediately; can progress to cauliflower ear if untreated; higher rate with cartilage-cutting |
| Infection | Pathogens: S. aureus, E. coli, P. aeruginosa; treat with evacuation + antibiotics |
| Perichondritis | Follows hematoma/infection; requires débridement + IV antibiotics |
| Cartilage necrosis | From infection, hematoma, cautery, or dressing pressure |
Late
| Complication | Notes |
|---|---|
| Inadequate correction | Most common overall |
| Telephone ear deformity | Upper + lower poles protrude anteriorly; due to overcorrection of mid-ear + undercorrection of poles |
| Suture extrusion/granuloma | Braided sutures > monofilament; delay removal several months to protect cosmetic result |
| Keloid/hypertrophic scar | Higher risk in young + pigmented patients; avoid aggressive skin resection |
| Hypoesthesia | Greater auricular nerve injury; usually resolves weeks–months |
| Cold susceptibility | Disrupted blood supply → frostbite risk |
| Patient dissatisfaction | Asymmetry ≤2–3 mm acceptable; overcorrection better tolerated than undercorrection; set realistic expectations preoperatively |
Key Principles
| Approach | Recurrence | Irregularities |
|---|---|---|
| Cartilage-cutting | Lower | Higher |
| Cartilage-sparing | Higher | Lower |
| Graduated (combined) | Best long-term outcomes | Balanced |
Preoperative photography is mandatory: anterior full face, posterior full head, bilateral close-ups.
Sources: Cummings Otolaryngology Head and Neck Surgery, Ch. 28 (p. 557–560); K.J. Lee's Essential Otolaryngology, p. 1072
This is a shared conversation. Sign in to Orris to start your own chat.