I want to given presentation tomorrow on tb case tell me about tb , its cause , diagnosis, new and old mangement of Drug suitable tb , mdr tb ,xtr tb
Reading File
Finding Sources
Finding Sources
Searching PubMed
tuberculosis treatment guidelines drug resistant
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have very comprehensive data from authoritative textbooks. Let me compile the full, detailed presentation-ready response.
Tuberculosis (TB) - Complete Clinical Overview
Sources: Murray & Nadel's Respiratory Medicine, Fishman's Pulmonary Diseases, Park's Preventive & Social Medicine, Robbins & Cotran Pathologic Basis of Disease, Tintinalli's Emergency Medicine, and recent PubMed systematic reviews (2024-2025).
1. INTRODUCTION & EPIDEMIOLOGY
TB has been called the "captain of all men of death." It remains the single most common infectious cause of death worldwide.
- ~10.6 million new cases globally in 2022 (Robbins & Cotran, 2025 data)
- 1.3 million deaths annually; 167,000 in HIV-positive individuals
- India alone accounts for ~2.64 million new cases per year
- High-burden countries: India, Indonesia, China, Philippines, Pakistan, Nigeria, South Africa
- TB flourishes in settings of poverty, crowding, and debilitating illness (prisons, homeless shelters, slums)
Risk Factors for Disease Progression:
- HIV/AIDS (100-fold increased risk of progression to active TB)
- Diabetes mellitus
- Silicosis and chronic lung disease
- Chronic renal failure, malnutrition
- Immunosuppression (corticosteroids, TNF inhibitors, transplant)
- Alcohol use disorder
- Young children (<5 years) and elderly
2. ETIOLOGY & MICROBIOLOGY
Causative Organism: Mycobacterium tuberculosis (MTBC complex)
The MTBC includes:
- M. tuberculosis - responsible for the vast majority of human disease
- M. bovis - from unpasteurized milk (rare in pasteurized-milk countries)
- M. africanum - restricted to Africa
- M. canettii - rare, East Africa only
Key Microbiological Features:
- Aerobic, non-motile, non-spore-forming acid-fast bacillus (AFB)
- Identified by Ziehl-Neelsen (ZN) staining - appears red against blue background
- Very slow doubling time (~20 hours); cultures take 3-8 weeks on Lowenstein-Jensen media
- Resistant to drying, UV light, and many disinfectants
- Infectious dose: fewer than 10 bacteria
Phylogenetic Lineages:
| Lineage | Geographic Origin |
|---|---|
| 1 - Indo-Oceanic | South/SE Asia |
| 2 - East Asian (Beijing strain) | East Asia - high virulence |
| 3 - Indian/East African | India, East Africa |
| 4 - Euro-American | Europe, Americas |
| 5 & 6 - West African | West Africa (= M. africanum) |
3. TRANSMISSION
- Droplet nuclei (1-5 μm dried particles) - suspended indefinitely in air; deposit in alveoli
- Source: coughing, sneezing, speaking, singing by infectious case
- 99% reduction in sputum colony counts in first 2 weeks of effective treatment
- Patients considered non-infectious after 2 weeks of effective chemotherapy
- Environmental factors: poor ventilation, crowding, lack of UV light
- Only ~8-19% of transmission occurs within households; community contacts account for the majority in high-burden settings
4. PATHOGENESIS
(Robbins & Cotran Pathologic Basis of Disease)
Step 1 - Entry into Macrophages:
M. tuberculosis enters alveolar macrophages via phagocytosis through mannose-binding lectin and complement receptor CR3. Alveolar macrophages are the first cells infected.
Step 2 - Replication in Macrophages:
The bacterium blocks phagolysosome formation by recruiting host protein coronin, which activates calcineurin to inhibit phagosome-lysosome fusion. Bacteria replicate unchecked inside the phagosome. This produces bacteremia and seeding of multiple sites in the first 3 weeks.
Step 3 - Th1 Immune Response (3-8 weeks):
- CD4+ T cells activate macrophages via interferon-gamma (IFN-γ)
- Activated macrophages can kill bacteria
- This response also forms the basis of TST/IGRA positivity
Step 4 - Granuloma Formation:
- Granuloma = organized collection of epithelioid macrophages + multinucleated giant cells (Langhans) + lymphocytes
- Central caseous necrosis - "cheese-like" necrosis, unique to TB
- Ghon focus = primary lung lesion + Ghon complex when hilar nodes involved
Step 5 - Latency vs. Reactivation:
- 90% of immunocompetent individuals: bacteria contained, latent TB infection (LTBI)
- 5-10%: develop active disease in their lifetime; risk highest in first 2 years
- Reactivation triggered by immune compromise (HIV, immunosuppressants, aging)
5. CLINICAL FEATURES
Primary TB
- Usually asymptomatic in healthy individuals
- May cause transient fever, pleural effusion, hilar lymphadenopathy
- Residual: tiny fibrocalcific Ghon focus on CXR
Reactivation/Post-Primary Pulmonary TB
Constitutional symptoms (systemic - from TNF cytokines):
- Low-grade afternoon/evening fever (remittent pattern)
- Night sweats
- Malaise, fatigue, anorexia, weight loss
Pulmonary symptoms (as disease progresses):
- Chronic productive cough (>3 weeks - cardinal symptom)
- Hemoptysis (blood-streaked or frank blood)
- Dyspnea, pleuritic chest pain
Physical Examination:
- Often unremarkable early
- Wheezes, rales, signs of consolidation
- Signs of pleural effusion
Extrapulmonary TB (occurs more often in immunocompromised, HIV+)
| Site | Features |
|---|---|
| Lymph nodes (most common extra-pulm) | Painless enlargement, may coalesce, "scrofula" |
| Pleura | Exudative effusion, high ADA |
| CNS / Meningitis | Subacute meningitis, cranial nerve palsies, hydrocephalus |
| Pericarditis | Constrictive pericarditis risk |
| Spine (Pott's disease) | Back pain, gibbus deformity, cold abscess |
| Abdominal / GI | Ileocecal area, peritonitis, ascites |
| GU / Renal | Sterile pyuria, renal abscess |
| Miliary TB | Diffuse hematogenous spread; millet-seed lesions on CXR; high mortality |
6. DIAGNOSIS
A. Sputum Smear Microscopy (ZN Smear)
- Sensitivity: 29-60% (poor when patient cannot produce adequate sputum)
- Sensitivity improves to ~67% with proper technique (LEDFM = LED fluorescence microscopy)
- 2 specimens collected: spot + early morning (or spot-spot)
- Positive = ≥3 log colony forming units per mL needed
- Quick, cheap, widely available - but low sensitivity
B. Nucleic Acid Amplification Test (NAAT / CB-NAAT / GeneXpert MTB/RIF)
- Cartridge-Based NAAT (CB-NAAT/Xpert MTB/RIF) - WHO-endorsed, used in NTEP India
- Detects M. tuberculosis DNA AND rifampicin resistance simultaneously
- Sensitivity ~89%, specificity ~99% for pulmonary TB
- Result in 2 hours
- First-line test in most programs for presumptive TB
C. Culture (Gold Standard)
- Lowenstein-Jensen (LJ) solid media: 3-8 weeks
- MGIT (Mycobacteria Growth Indicator Tube) liquid media: 1-3 weeks
- Necessary for Drug Susceptibility Testing (DST)
- Sensitivity nearly 100% if adequate specimens
D. Tuberculin Skin Test (TST / Mantoux Test)
- Intradermal injection of 5 TU PPD; read at 48-72 hours
- Positive (induration):
- ≥5 mm: HIV+, close contacts of TB case, CXR changes
- ≥10 mm: High-risk groups (healthcare workers, immigrants, prisoners, diabetes)
- ≥15 mm: Low-risk general population
- Limitations: False-positive with BCG vaccination; false-negative in immunocompromised, miliary TB, elderly
E. Interferon-Gamma Release Assay (IGRA)
- QuantiFERON-TB Gold Plus, T-SPOT.TB
- Detects IFN-γ released by sensitized T-cells in response to ESAT-6 and CFP-10 antigens
- More specific than TST (not affected by BCG)
- Useful for LTBI diagnosis; indeterminate results common in immunocompromised
- Negative result makes TB less likely
F. Chest X-Ray (CXR)
- Primary TB: Hilar/paratracheal lymphadenopathy, Ghon complex, lower/mid-zone infiltrate
- Post-primary / Reactivation TB: Upper lobe infiltrates, cavitation, fibrosis, calcification
- Miliary TB: Diffuse bilateral 1-3 mm nodules ("millet seeds")
- Pleural TB: Unilateral effusion
G. CT Chest
- More sensitive than CXR
- Shows tree-in-bud pattern (endobronchial spread), cavities, lymphadenopathy
H. Bronchoscopy / BAL
- For smear-negative cases; BAL sent for AFB smear, culture, NAAT
I. Adenosine Deaminase (ADA)
- Elevated in TB pleural effusion (>40 U/L), TB meningitis (CSF >10 U/L), TB peritonitis
J. Histopathology
- Biopsy showing caseating granuloma with Langhans giant cells = highly suggestive
- AFB stain on tissue + culture
7. DRUG-SENSITIVE TB (DS-TB) TREATMENT
First-Line Anti-TB Drugs (OLD and STILL CORE)
| Drug | Code | Mechanism | Key Side Effects |
|---|---|---|---|
| Isoniazid | H | Inhibits mycolic acid synthesis (InhA, KatG) | Hepatotoxicity, peripheral neuropathy (prevent with pyridoxine 10-20 mg/day) |
| Rifampicin | R | RNA polymerase inhibition (rpoB) | Hepatotoxicity, flu-like syndrome, orange urine, drug interactions (CYP450 inducer) |
| Pyrazinamide | Z | Disrupts membrane energy; active against intracellular/slow-multiplying bacilli | Hepatotoxicity, hyperuricemia/gout, arthralgia |
| Ethambutol | E | Inhibits arabinosyltransferase (cell wall arabinogalactan) | Optic neuritis (dose-dependent; monitor vision) |
| Streptomycin | S | Inhibits 30S ribosomal subunit | Vestibular damage, ototoxicity, nephrotoxicity |
Standard DS-TB Regimen
2HRZE / 4HR (total 6 months)
| Phase | Duration | Drugs |
|---|---|---|
| Intensive Phase | 2 months | H + R + Z + E (4 drugs daily) |
| Continuation Phase | 4 months | H + R (2 drugs daily) |
- DOTS (Directly Observed Treatment, Short-course): health worker observes each dose; proven most cost-effective intervention globally
- NTEP (India's National TB Elimination Programme) switched from thrice-weekly intermittent to daily fixed-dose combination (FDC) regimens in 2016
Weight-Based FDC Dosing (Adults)
| Weight | HRZE (Intensive) | HR (Continuation) |
|---|---|---|
| 30-54 kg | 2 tabs | 2 tabs |
| 55-70 kg | 3 tabs | 3 tabs |
| >70 kg | 4 tabs | 4 tabs |
Monitoring During Treatment
- Monthly clinical follow-up (weight, symptoms)
- Sputum smear at end of intensive phase and end of treatment
- LFTs at baseline (and if symptomatic)
- Visual acuity (ethambutol)
8. DRUG-RESISTANT TB (DR-TB)
Definitions
| Type | Definition |
|---|---|
| Mono-resistance | Resistant to 1 first-line drug |
| Poly-resistance | Resistant to >1 first-line drug (not both H+R) |
| MDR-TB | Resistant to Isoniazid (H) + Rifampicin (R) (the 2 most potent first-line drugs) |
| RR-TB | Rifampicin-resistant (treated same as MDR-TB) |
| Pre-XDR-TB (WHO 2021) | MDR/RR-TB + resistant to any fluoroquinolone |
| XDR-TB (WHO 2021 revised) | MDR/RR-TB + resistant to fluoroquinolone + at least one of bedaquiline or linezolid |
Important Note: In 2021, WHO revised the XDR-TB definition. Previously it included resistance to fluoroquinolones + second-line injectables (amikacin/kanamycin/capreomycin). The new definition replaces injectables with bedaquiline/linezolid.
Global Burden:
- ~5% of all new TB cases and ~18% of previously treated cases are MDR-TB
- 6.2% of MDR-TB cases had XDR-TB (as of 2017-2018 data)
- Only 32% of MDR-TB patients received second-line treatment
Second-Line TB Drugs (for DR-TB)
Group A (Preferred - use all 3 unless contraindicated):
| Drug | Code | Notes |
|---|---|---|
| Levofloxacin or Moxifloxacin | Lfx / Mfx | Fluoroquinolones - backbone of MDR-TB therapy |
| Bedaquiline | Bdq | ATP synthase inhibitor - NEW; diarylquinolines class; 24 weeks typically |
| Linezolid | Lzd | Oxazolidinone - inhibits 50S; effective but toxic (bone marrow suppression, neuropathy) |
Group B (Add if needed):
| Drug | Code | Notes |
|---|---|---|
| Clofazimine | Cfz | Membrane disruption; anti-leprosy drug repurposed |
| Cycloserine / Terizidone | Cs/Trd | Inhibits cell wall synthesis; CNS side effects |
Group C (Add to complete regimen):
| Drug | Notes |
|---|---|
| Ethambutol (E) | Used in shorter regimen |
| Delamanid (Dlm) | NEW - nitroimidazole; inhibits mycolic acid; alternative to Bdq |
| Pyrazinamide (Z) | If susceptible |
| Imipenem-Cilastatin / Meropenem | Carbapenems - for highly resistant cases |
| Amikacin (Am) | Injectable; use only if susceptible + close monitoring |
| Streptomycin (S) | Only if susceptible |
| High-dose INH (Hhigh) | If certain resistance mutations |
| Ethionamide/Prothionamide (Eto/Pto) | Inhibit mycolic acid |
| PAS (para-aminosalicylic acid) | Oldest Group C agent |
9. MDR-TB MANAGEMENT (Current WHO/NTEP Guidelines)
Regimen Options (NTEP India 2019)
1. H Mono/Poly DR-TB (Rifampicin-susceptible):
- (6) Lfx R E Z - 6 months total, all oral
2. Shorter MDR-TB Regimen (9-11 months):
| Phase | Duration | Drugs |
|---|---|---|
| Intensive | 4-6 months | Mfx(h) + Km/Am + Eto + Cfz + Z + H(h) + E |
| Continuation | 5 months | Mfx(h) + Cfz + Z + E |
- Not eligible if: prior exposure to second-line drugs >1 month, resistance to fluoroquinolones or second-line injectables, pregnancy, extrapulmonary TB involving CNS/bone
3. All-Oral Longer MDR-TB Regimen (18-20 months):
(18-20) Bdq(6) Lfx Lzd Cfz Cs*
This is the preferred regimen currently, replacing injectable-based regimens.
10. XDR-TB MANAGEMENT
BPaLM Regimen - THE NEWEST (2022 WHO Endorsed)
Bedaquiline + Pretomanid + Linezolid ± Moxifloxacin
| Component | Role |
|---|---|
| Bedaquiline (B) | ATP synthase inhibition |
| Pretomanid (Pa) | Nitroimidazole; inhibits mycolic acid AND has anaerobic bactericidal activity; NEW drug approved 2019 |
| Linezolid (L) | Protein synthesis inhibition |
| Moxifloxacin (M) | Added if susceptible (makes it BPaLM) |
- Duration: 6 months (dramatically shorter than 18-24 months)
- A 2025 systematic review (PMID: 39813501) confirms BPaLM effective for MDR/RR-TB with favorable outcomes
- A 2024 network meta-analysis (PMID: 39354416) confirms shorter regimens are efficacious and safe
ZeNix and TB-PRACTECAL Trial Results
- BPaL (without moxifloxacin) showed ~89% favorable outcomes in XDR-TB in 6 months
- BPaLM may allow even shorter duration (4-6 months) for MDR-TB
11. COMPARISON: OLD vs. NEW MANAGEMENT
| Aspect | Old Approach | New Approach |
|---|---|---|
| DS-TB | Intermittent (thrice-weekly) DOTS | Daily FDC regimen |
| MDR-TB | 18-24 months with injectables (Km, Am, Cm) | All-oral 18-20 months (Bdq + Lfx + Lzd + Cfz + Cs) |
| XDR-TB | 24+ months, individualized, poor outcomes | BPaLM for 6 months |
| Key newer drugs | None | Bedaquiline (2012), Delamanid (2014), Pretomanid (2019) |
| Monitoring | Clinical only | Molecular DST, NAAT, culture conversion monitoring |
| Injectable use | Core component | Avoided where possible (toxicity) |
12. DRUG DOSES (REFERENCE)
First-Line Drug Doses (Adults)
| Drug | Daily Dose |
|---|---|
| Isoniazid (H) | 5 mg/kg (max 300 mg) |
| Rifampicin (R) | 10 mg/kg (max 600 mg) |
| Pyrazinamide (Z) | 25 mg/kg (max 2 g) |
| Ethambutol (E) | 15 mg/kg (max 1.2 g) |
| Streptomycin (S) | 15 mg/kg IM (max 1 g; 0.75 g if >50 yrs) |
Key MDR-TB Drug Doses
| Drug | Dose |
|---|---|
| Bedaquiline | 400 mg OD x 2 weeks, then 200 mg TIW x 22 weeks |
| Linezolid | 600 mg OD (or 300 mg OD to reduce toxicity) |
| Levofloxacin | 15 mg/kg OD (max 1000 mg) |
| Moxifloxacin | 400 mg OD |
| Clofazimine | 100 mg OD |
| Delamanid | 100 mg BD |
| Pretomanid | 200 mg OD |
13. PREVENTION
BCG Vaccine
- Bacille Calmette-Guérin - live attenuated M. bovis
- Given at birth (in high-burden countries like India)
- Protects against severe/disseminated TB in children (miliary TB, TB meningitis) - 75-85% efficacy
- Does NOT reliably prevent pulmonary TB in adults
- Creates TST false-positives; does NOT affect IGRA
Treatment of Latent TB Infection (LTBI)
Indicated in: HIV+, recent TB contacts, organ transplant recipients, anti-TNF therapy users
| Regimen | Duration |
|---|---|
| INH daily | 6 months (6H) or 9 months (9H) |
| INH + Rifapentine weekly | 3 months (3HP) - preferred short course |
| Rifampicin daily | 4 months (4R) |
Infection Control
- Negative pressure isolation rooms for active TB cases
- N95 respirators for healthcare workers
- UV germicidal irradiation
- Adequate ventilation
14. QUICK SUMMARY TABLE FOR PRESENTATION
| Category | Key Points |
|---|---|
| Cause | M. tuberculosis, airborne droplet nuclei |
| Pathology | Caseating granuloma, Ghon focus |
| Symptoms | Cough >3 wks, fever, night sweats, weight loss, hemoptysis |
| Diagnosis | ZN smear, NAAT/GeneXpert, Culture, TST/IGRA, CXR |
| DS-TB Rx | 2HRZE / 4HR (6 months) |
| MDR-TB Rx | Bdq + Lfx + Lzd + Cfz + Cs (18-20 months, all oral) |
| XDR-TB Rx | BPaLM - 6 months |
| New Drugs | Bedaquiline, Pretomanid, Delamanid, Linezolid |
| Prevention | BCG, DOTS, LTBI treatment, infection control |
Recent Evidence (2024-2025)
- Shorter MDR-TB regimens are efficacious - Network meta-analysis confirms shorter all-oral regimens have similar efficacy to longer injectable-containing regimens (PMID 39354416, BMC Infect Dis, 2024)
- BPaLM systematic review - Bedaquiline + pretomanid + linezolid ± moxifloxacin shows high treatment success in MDR/RR-TB (PMID 39813501, J Bras Pneumol, 2025)
Good luck with your presentation tomorrow! The most discussion-worthy current topic is the shift from injectable-based to all-oral regimens for MDR-TB, and the BPaLM regimen dramatically shortening XDR-TB treatment from 24+ months to just 6 months - this is the biggest advance in TB management in decades.
Find and compile TB chest X-ray images showing various presentations
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
All images retrieved. Here is the complete compiled image gallery with detailed radiological interpretation for your presentation.
TB Chest X-Ray & Imaging Gallery
All images sourced from authoritative medical textbooks (Murray & Nadel's Respiratory Medicine, Harrison's Principles, Goldman-Cecil Medicine).
1. PRIMARY TB - Hilar Lymphadenopathy with Lower Lobe Consolidation
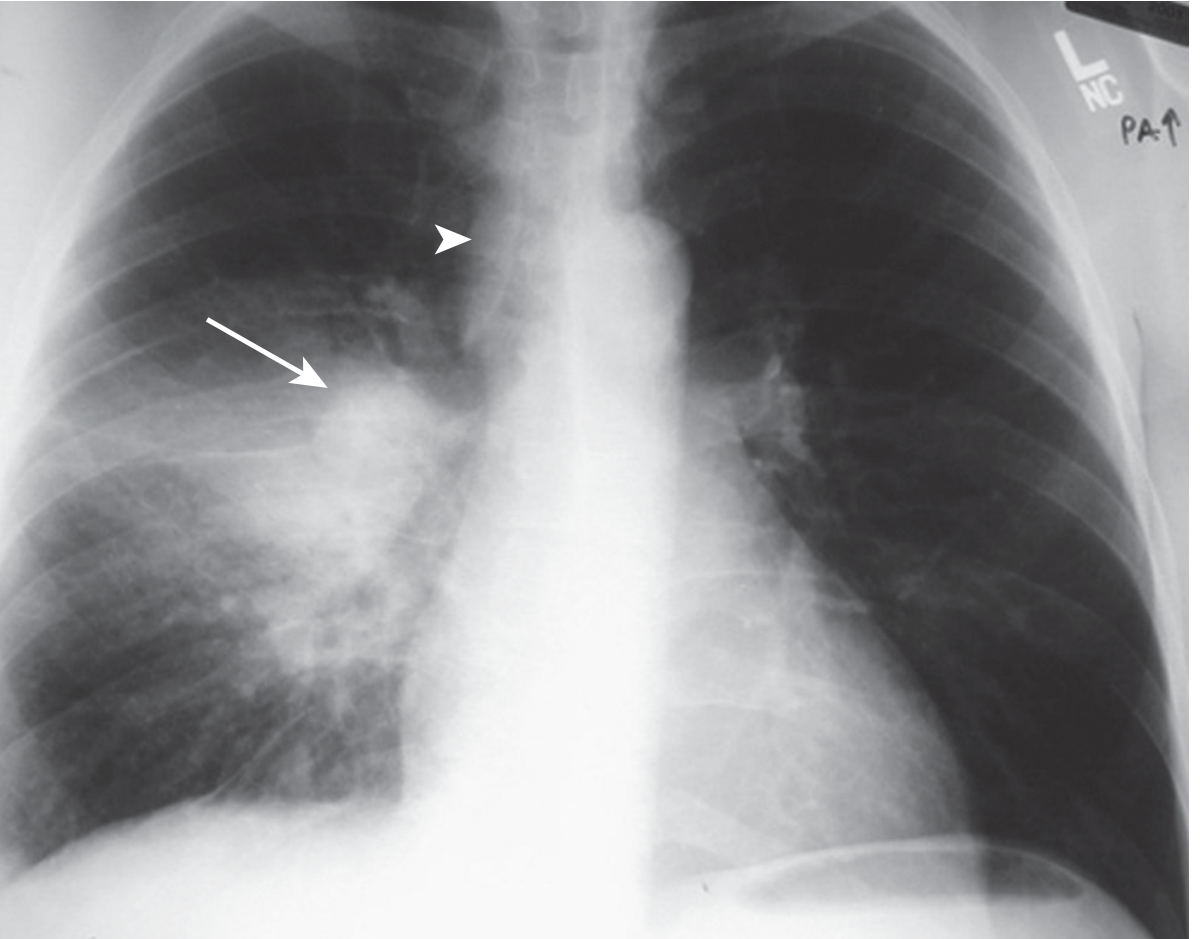
What to see: Right lower/middle zone consolidation (arrow) + right hilar lymphadenopathy (arrowhead) + mild right paratracheal node enlargement. This is the classic "Ghon complex" pattern - primary infection site in lower/mid zone with ipsilateral hilar node enlargement. Typical in children and young adults with initial TB exposure.
Source: Murray & Nadel's Textbook of Respiratory Medicine
2. PRIMARY TB in a Child - Right Hilar Lymph Node Enlargement

What to see: Prominent right hilar enlargement with infiltration into surrounding lung tissue in a child. Note the relatively clear lung fields compared to adult reactivation TB. Lymph node enlargement can compress bronchi, causing atelectasis or ball-valve hyperinflation. This is from a paediatric case (Stellenbosch University).
Source: Harrison's Principles of Internal Medicine 22E
3. REACTIVATION TB - Extensive Right Upper Lobe Cavitation
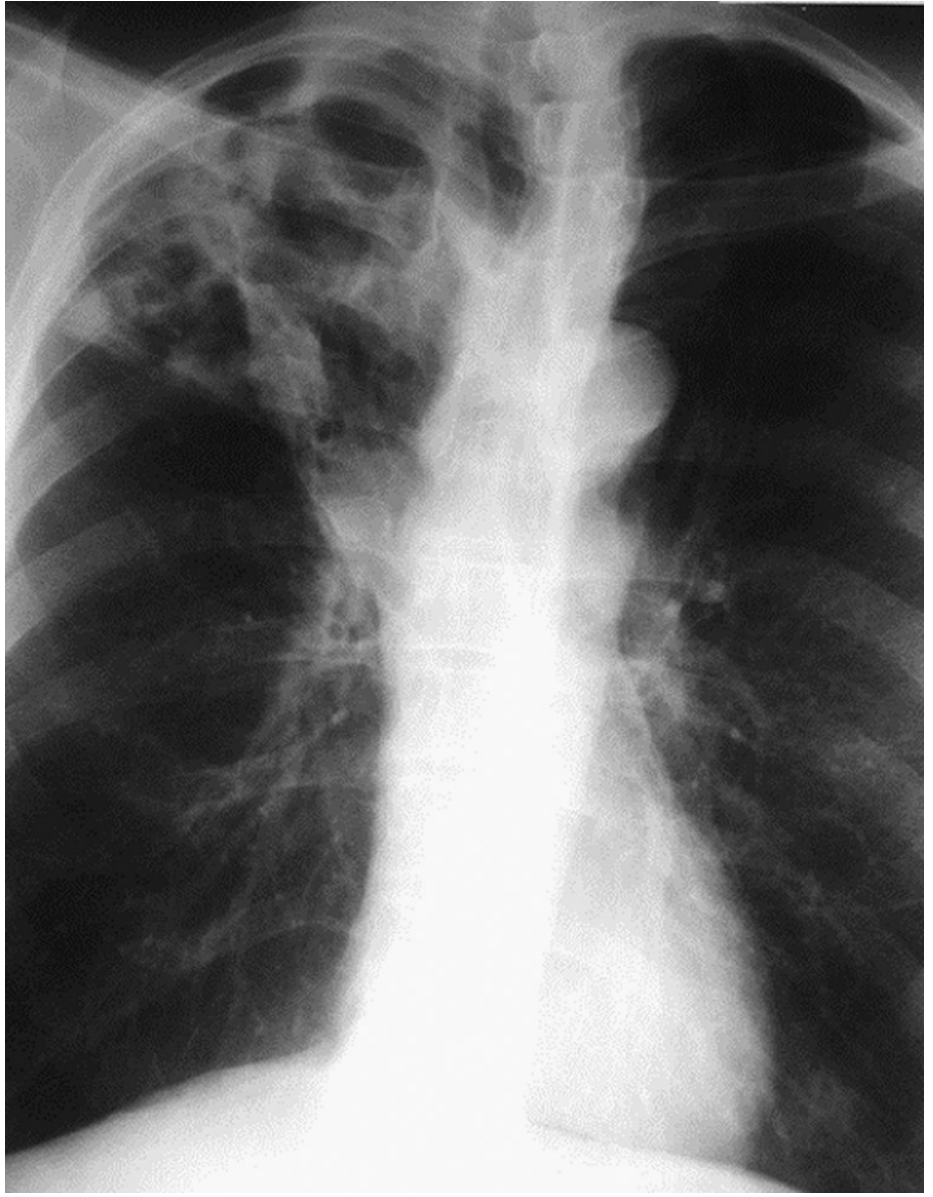
What to see: Extensive right upper lobe opacity with multiple cavities. This is the classic reactivation (post-primary) TB pattern - apical and posterior segments of right upper lobe are the most common site. Note the heterogeneous density suggesting both consolidation and cavitation. The left lung is relatively spared. Cavitation indicates high bacterial load and very infectious state.
Source: Murray & Nadel's Textbook of Respiratory Medicine
4. ACTIVE TB - Right Upper Lobe Infiltrate with Air-Fluid Level Cavity
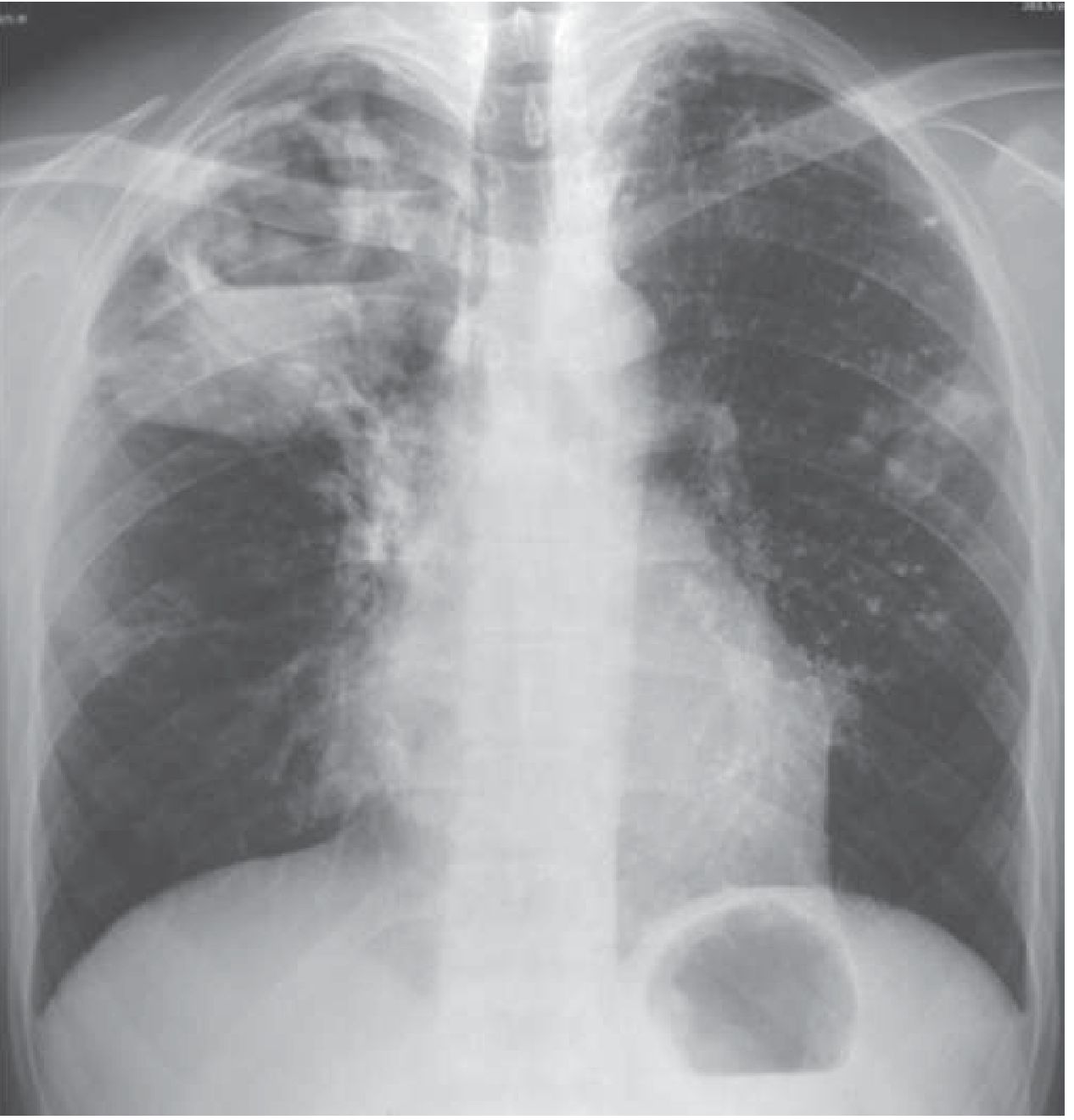
What to see: Bilateral upper zone infiltrates with confluent opacification. Right side shows extensive consolidation and cavitation. Left upper lobe also involved with nodular opacities. This bilateral disease pattern reflects bronchogenic spread from a dominant right-sided cavity to the contralateral lung - a marker of advanced, highly infectious disease.
Source: Harrison's Principles of Internal Medicine 22E
5. CAVITARY TB - CXR + CT (Air-Fluid Level)
What to see: (A) CXR showing right upper lobe cavitation with extensive opacity and left-sided nodular opacities and left hilar lymphadenopathy. A textbook cavitary TB case with contralateral bronchogenic spread.
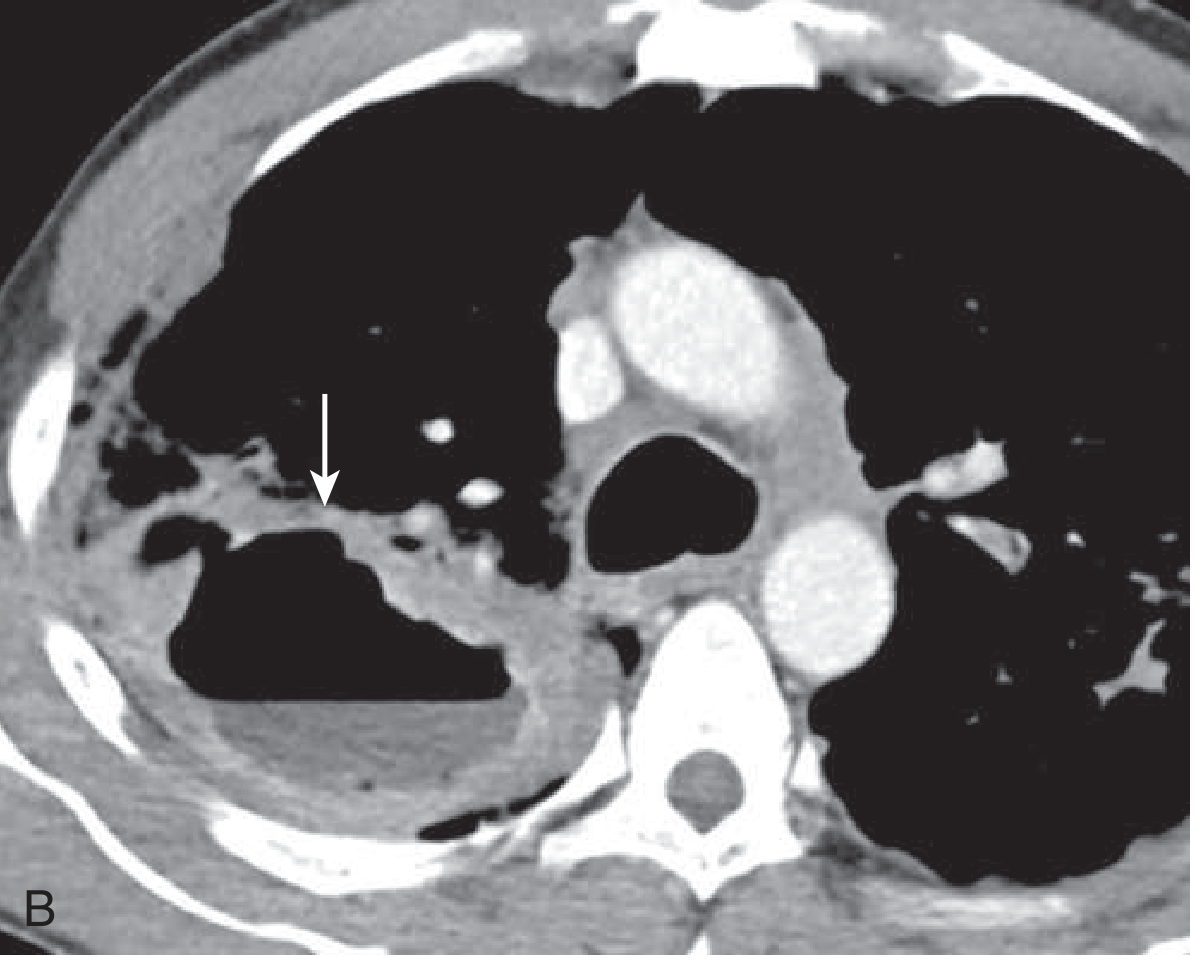
What to see: (B) Contrast-enhanced CT axial image showing the irregular cavity with an air-fluid level in the posterior right upper lobe (arrow). CT is far superior to CXR for demonstrating cavity walls, satellite nodules, and endobronchial spread.
Source: Goldman-Cecil Medicine
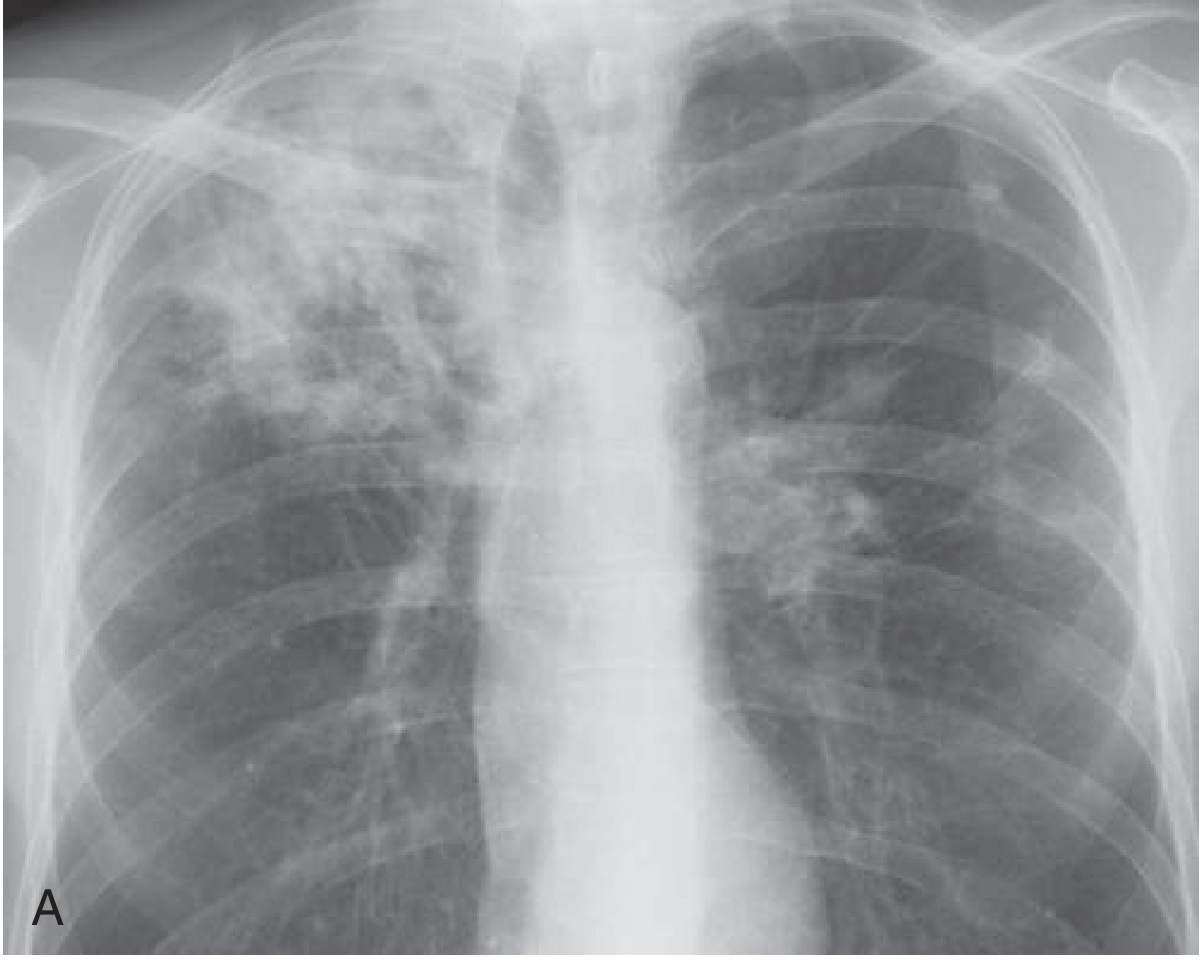
6. TB in HIV - Bilateral Hilar Lymphadenopathy + Nodular Opacities
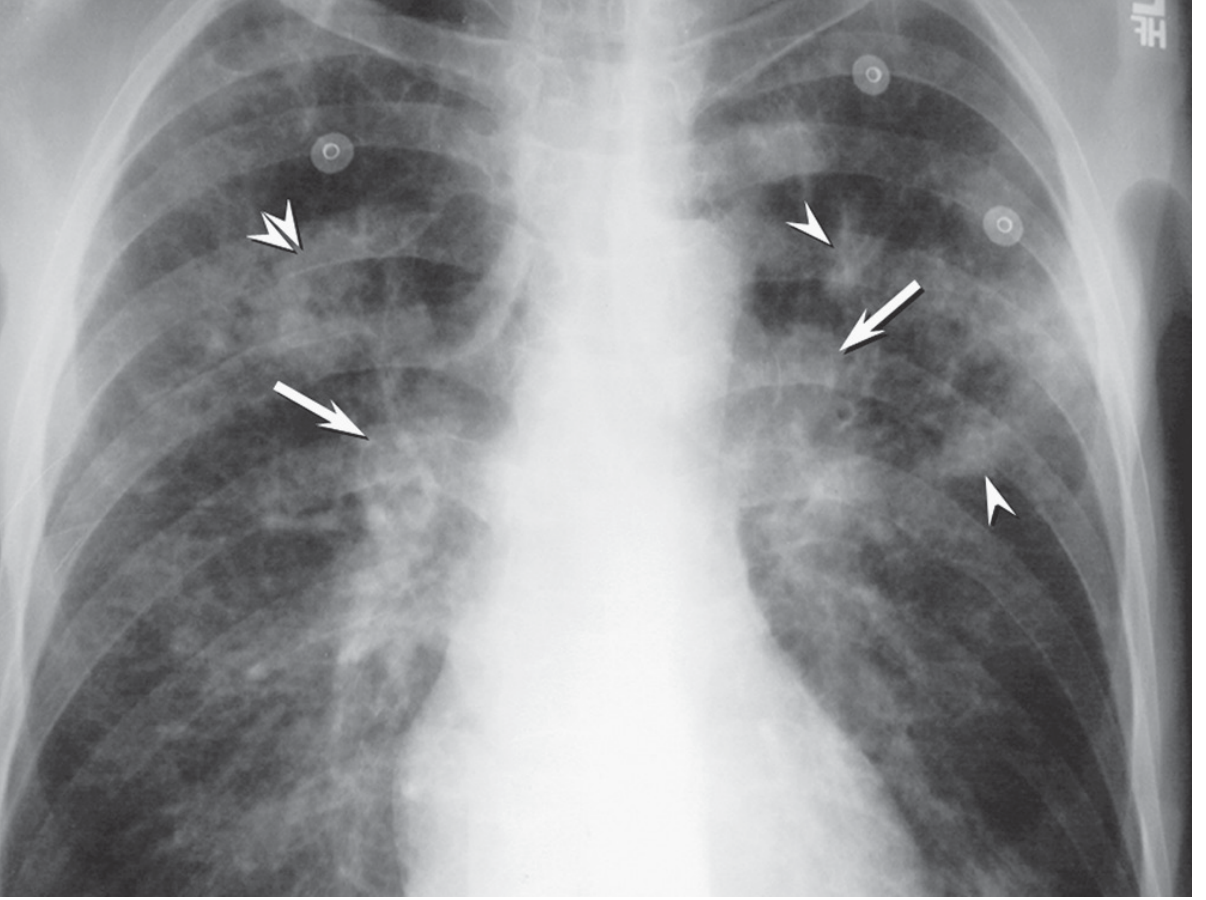
What to see: Bilateral hilar lymph node enlargement (arrows) + poorly defined parenchymal nodular opacities (arrowheads) + nodular consolidation (double arrowheads). This "atypical" pattern is characteristic of TB in immunocompromised/HIV patients with advanced CD4 depletion. Cavitation is notably absent - unlike typical reactivation TB. Lower zone involvement and mediastinal adenopathy predominate. This pattern may mimic lymphoma or sarcoidosis.
Source: Murray & Nadel's Textbook of Respiratory Medicine
7. MILIARY TB - Bilateral Micronodular Pattern (CXR)

What to see: Innumerable small, randomly distributed nodules (1-3 mm) throughout both lung fields - the "millet seed" pattern that gives miliary TB its name. The nodules are uniform in size and distribution, unlike metastatic disease which tends to be more variable. This pattern results from hematogenous dissemination. Associated with severe immunosuppression and carries high mortality if untreated.
Source: Murray & Nadel's Textbook of Respiratory Medicine
8. MILIARY TB - CXR + Coronal CT (Side by Side)
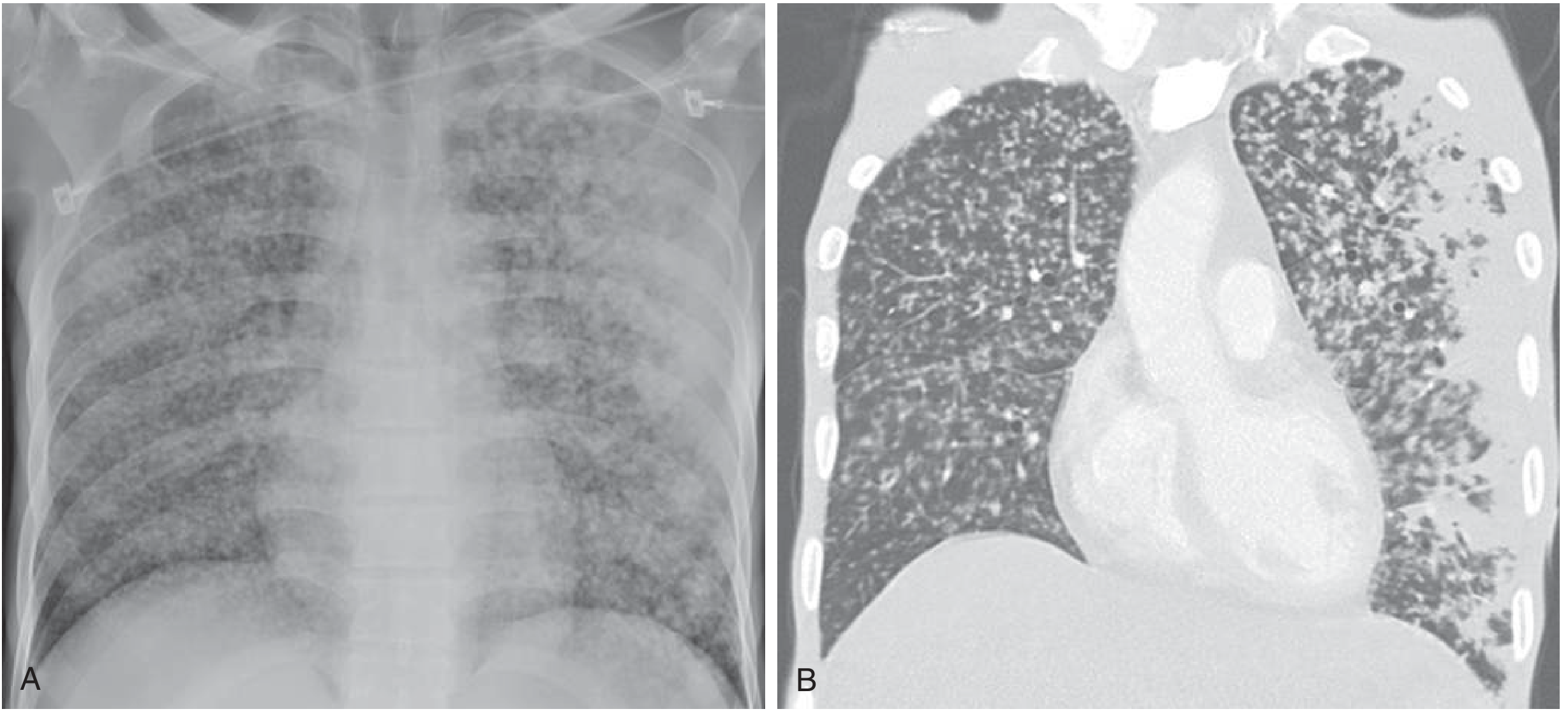
What to see: (A) CXR showing diffuse micronodular disease with more confluent peripheral consolidation bilaterally. (B) Coronal CT showing extensive, randomly distributed miliary micronodules throughout both lungs with confluent disease and consolidation at the periphery. CT demonstrates the miliary pattern far more clearly than CXR and can detect it earlier. This is from a 53-year-old man with miliary TB.
Source: Goldman-Cecil Medicine
Radiographic Pattern Summary Table
| TB Type | Typical Location | Key CXR Finding | Key Feature |
|---|---|---|---|
| Primary TB | Lower/mid zone | Hilar lymphadenopathy + consolidation | Ghon complex |
| Reactivation TB | Upper lobes (apical/posterior) | Infiltrate + cavitation | Right > Left |
| Cavitary TB | Upper lobes | Thick-walled cavity, ± air-fluid level | Highly infectious |
| Miliary TB | Bilateral, diffuse | 1-3 mm uniform nodules ("millet seeds") | Hematogenous spread |
| TB in HIV | Any zone | Adenopathy, lower lobe infiltrates, NO cavity | Atypical pattern |
| TB Pleural Effusion | Unilateral | Blunting of costophrenic angle | High ADA |
| Healed/Latent TB | Upper lobes | Fibrosis, calcification, volume loss | Ghon focus |
Key Teaching Points for Presentation:
- CXR sensitivity is only ~48% vs CT sensitivity ~96% for active TB
- A normal CXR does NOT exclude TB - up to 11% of HIV+ TB patients have a normal film
- Cavitation = infectious - treatment rapidly reduces colony counts by 99.9% in 2 weeks
- The HIV pattern mimics lymphoma - always consider TB in immunocompromised patients with mediastinal adenopathy
- CT with "tree-in-bud" pattern indicates endobronchial (bronchogenic) spread - a marker of active disease
This is a shared conversation. Sign in to Orris to start your own chat.