Poisuelli law and its significance CVS physiology for 1st year mbbs to get full marks in university exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough, exam-ready answer. Let me compile the complete response.
CVS Physiology: Complete 1st Year MBBS Guide
PART 1: POISEUILLE'S LAW (Poiseuille Equation)
The Formula
$$R = \frac{8\eta l}{\pi r^4}$$
| Symbol | Meaning |
|---|---|
| R | Resistance to blood flow |
| η (eta) | Viscosity of blood |
| l | Length of the blood vessel |
| r⁴ | Radius of the vessel raised to the 4th power |
This can also be written in terms of blood flow (Q):
$$Q = \frac{\Delta P \cdot \pi r^4}{8\eta l}$$
Where ΔP = pressure difference across the vessel.
The Three Key Relationships (MUST KNOW for exams)
1. Resistance is DIRECTLY proportional to viscosity (η)
- If hematocrit rises (polycythemia), blood viscosity increases → resistance increases → flow decreases.
2. Resistance is DIRECTLY proportional to vessel length (l)
- Longer vessels = more resistance. Clinically relevant in obesity (more tissue = longer vessels to perfuse).
3. Resistance is INVERSELY proportional to r⁴ (the MOST IMPORTANT)
- This is the critical examinable point. A small change in radius causes a massive change in resistance because of the fourth-power relationship.
- If radius is halved (reduced to 1/2), resistance increases by 2⁴ = 16-fold.
- If radius is reduced to 1/4 (75% occlusion of a vessel), resistance increases by 4⁴ = 256-fold!
Exam Tip (Costanzo Physiology): "When the radius of a blood vessel decreases by one-half, resistance does not simply increase twofold - it increases by 16-fold (2⁴)." This example is a classic MCQ/short answer.
Classic Exam Problem
A carotid artery suffers a 75% reduction in radius (radius reduced to 1/4 its original size). Original blood flow = 400 mL/min. What is the new flow?
- Resistance increases by (1/4)⁴ = 256-fold
- New flow = 400 / 256 = 1.56 mL/min (from baseline 400 mL/min)
This illustrates why even minor narrowing of coronary or cerebral vessels causes dramatic ischemia.
Significance of Poiseuille's Law
| Area | Clinical/Physiological Significance |
|---|---|
| Arteriolar tone | Arterioles are the primary resistance vessels. Vasoconstriction/dilation by them dominates peripheral resistance. The 4th-power law means small changes in arteriolar radius have huge effects on organ blood flow. |
| Hypertension | Chronic hypertension causes arteriolar wall thickening → reduced lumen radius → dramatically increased resistance → left ventricular afterload increases |
| Atherosclerosis | Plaque reducing lumen radius by even 50% increases resistance 16-fold in that vessel |
| Blood viscosity | Polycythemia, sickle cell crisis, dehydration - all increase η → increase resistance and risk of thrombosis |
| Vasoconstriction drugs | Vasoconstrictors (adrenaline, noradrenaline) reduce r → massive rise in TPR via r⁴ law |
| Vasodilators | Nitrates, ACE inhibitors dilate vessels → small increase in r → large fall in resistance |
Series vs Parallel Resistance
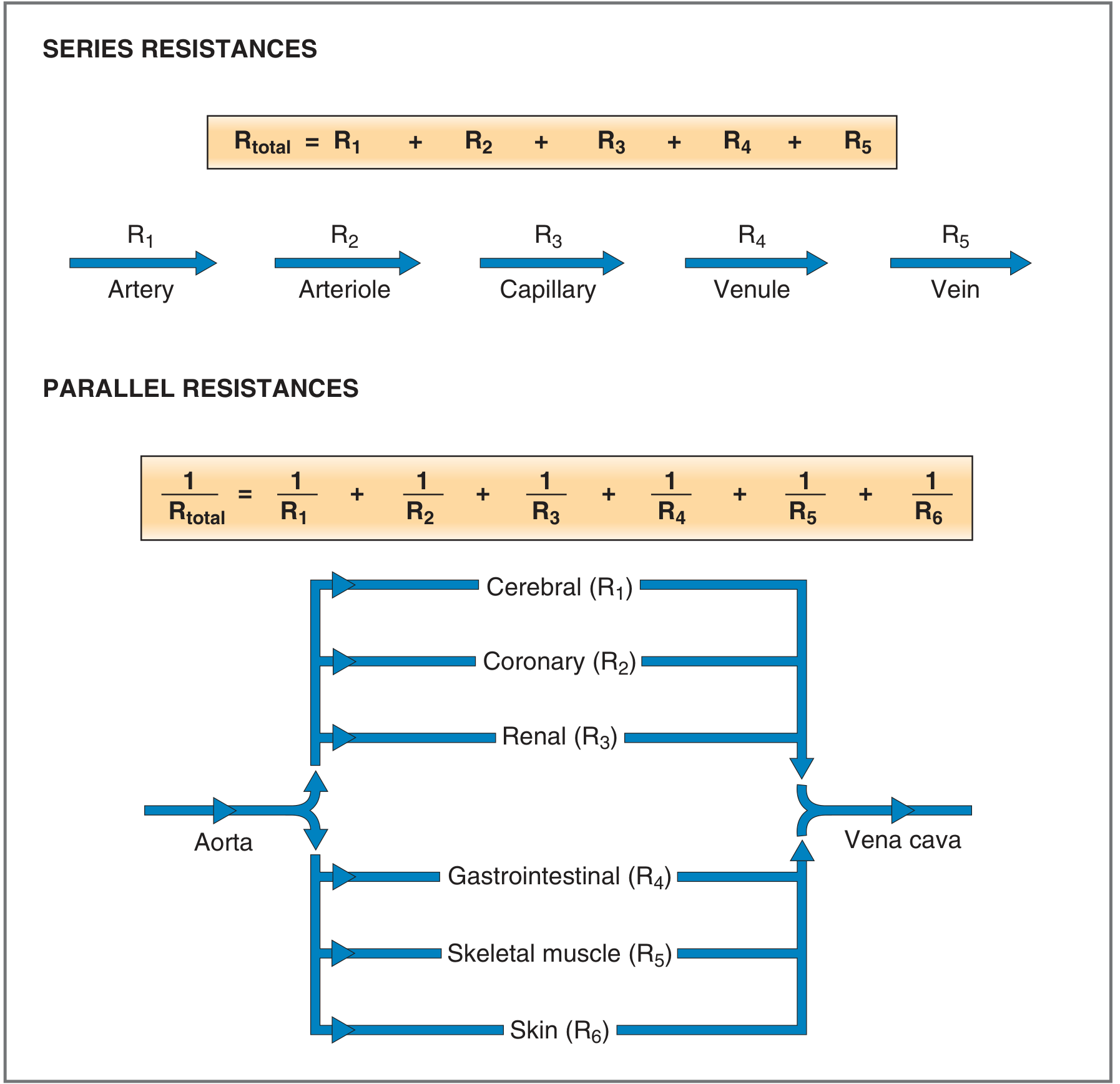
Series Resistance (within one organ):
$$R_{total} = R_{artery} + R_{arterioles} + R_{capillaries} + R_{venules} + R_{vein}$$
- Arterioles contribute the greatest resistance in series.
- Pressure drops progressively, with the biggest drop across arterioles.
Parallel Resistance (organs branching off aorta):
$$\frac{1}{R_{total}} = \frac{1}{R_1} + \frac{1}{R_2} + \frac{1}{R_3} + ...$$
- Total resistance is less than any individual resistance.
- This arrangement allows the body to distribute cardiac output to multiple organs simultaneously.
(Costanzo Physiology, 7th Ed., p. 129-130)
PART 2: CVS PHYSIOLOGY - COMPLETE FIRST YEAR MBBS
1. Blood Flow, Pressure, and Resistance (The Ohm's Law of CVS)
$$Q = \frac{\Delta P}{R}$$
- Q = Blood flow (mL/min or L/min)
- ΔP = Pressure difference (driving force)
- R = Resistance
Normal cardiac output at rest = 5,000 - 6,000 mL/min (5-6 L/min) in a 70 kg adult.
(Guyton and Hall Textbook of Medical Physiology)
2. Cardiac Output
$$CO = HR \times SV$$
| Parameter | Normal Value |
|---|---|
| Cardiac Output (CO) | 5 L/min |
| Heart Rate (HR) | 72 beats/min |
| Stroke Volume (SV) | ~70 mL/beat |
| Cardiac Index | CO / BSA = ~3.2 L/min/m² |
Factors determining Stroke Volume:
- Preload - End-diastolic volume (Frank-Starling mechanism)
- Afterload - Aortic pressure the ventricle must overcome
- Contractility - Intrinsic force of myocardial contraction (inotropy)
3. Frank-Starling Law of the Heart
"The greater the end-diastolic volume (preload), the greater the stroke volume ejected."
- As venous return increases → end-diastolic volume increases → myocardial fibers stretch → greater force of contraction → more stroke volume.
- This is the mechanism by which the heart automatically matches its output to venous return.
- It operates via the length-tension relationship of cardiac muscle (more stretch → more cross-bridge formation within physiological limits).
Exam definitions:
- Preload = End-diastolic volume (EDV) - the volume in the ventricle just before contraction
- Afterload = Aortic pressure (or arterial resistance) the left ventricle must overcome to eject blood
- Contractility (Inotropy) = Intrinsic ability of myocardium to generate force, independent of preload and afterload
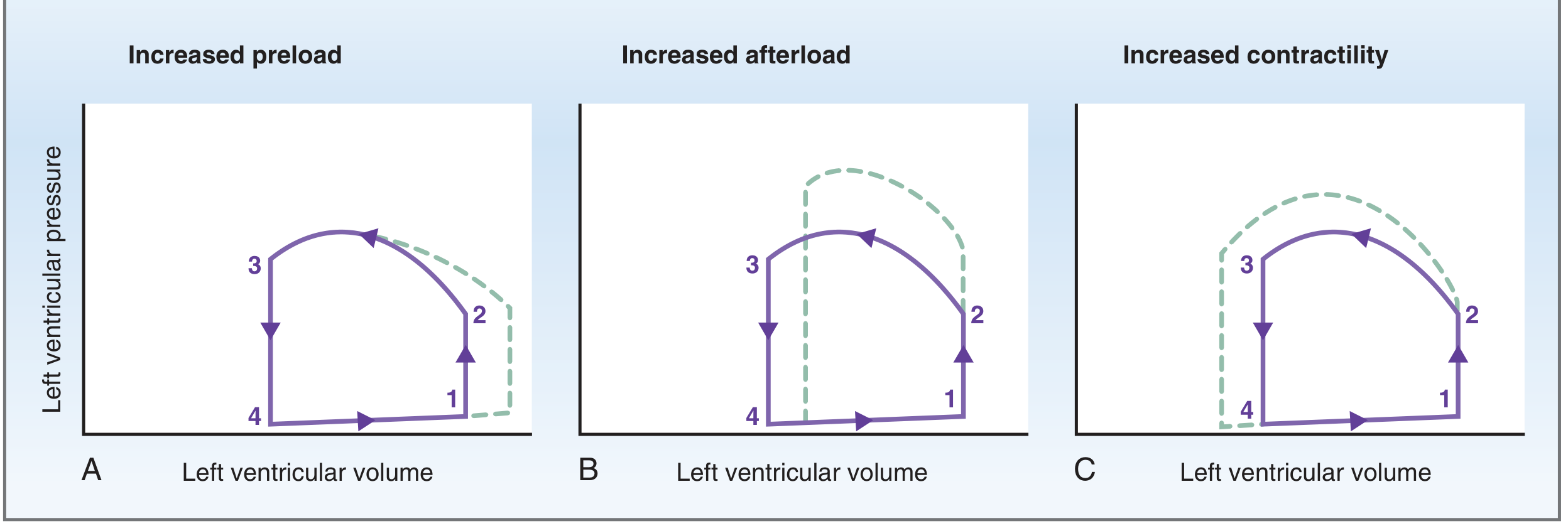
The pressure-volume loops above show:
- Increased preload (A): EDV increases → loop shifts right → wider loop = larger stroke volume
- Increased afterload (B): Ventricle must reach higher pressure → less blood ejected → stroke volume decreases, ESV increases
- Increased contractility (C): Ventricle ejects more forcefully → stroke volume increases, ESV decreases, with same preload
(Costanzo Physiology, 7th Ed., p. 158)
4. Fick Principle (Measurement of Cardiac Output)
$$CO = \frac{O_2 \text{ consumption}}{[O_2]{pulmonary vein} - [O_2]{pulmonary artery}}$$
Normal values for the calculation:
- O₂ consumption = 250 mL O₂/min
- Pulmonary venous O₂ content = 0.20 mL O₂/mL blood (= arterial)
- Pulmonary arterial O₂ content = 0.15 mL O₂/mL blood (= mixed venous)
$$CO = \frac{250}{0.20 - 0.15} = \frac{250}{0.05} = 5000 \text{ mL/min}$$
The Fick principle is based on conservation of mass: O₂ consumed by the body = O₂ delivered to tissues = CO × (arterial O₂ - venous O₂).
(Costanzo Physiology, 7th Ed.; Guyton & Hall)
5. Cardiac Cycle (Events in Sequence)
| Phase | Valves | Volume Change | Key Event |
|---|---|---|---|
| 1. Ventricular filling (diastole) | Mitral OPEN, Aortic CLOSED | Volume increases to EDV (~140 mL) | Passive + active filling |
| 2. Isovolumetric contraction | All valves CLOSED | Volume CONSTANT | Pressure builds until > aortic pressure |
| 3. Ventricular ejection (systole) | Aortic OPEN, Mitral CLOSED | Volume falls to ESV (~70 mL) | SV = 140-70 = 70 mL |
| 4. Isovolumetric relaxation | All valves CLOSED | Volume CONSTANT | Pressure falls |
Key definitions:
- EDV (End-Diastolic Volume) = 120-140 mL
- ESV (End-Systolic Volume) = 50-70 mL
- Stroke Volume = EDV - ESV = ~70 mL
- Ejection Fraction (EF) = SV/EDV = 70/140 = 50-65% (normal ≥ 55%)
6. Heart Sounds
| Sound | Timing | Cause |
|---|---|---|
| S1 ("lub") | Start of systole | Closure of mitral + tricuspid (AV) valves |
| S2 ("dub") | End of systole | Closure of aortic + pulmonary (semilunar) valves |
| S3 | Early diastole | Rapid ventricular filling (normal in children, abnormal in adults - heart failure) |
| S4 | Late diastole / presystole | Atrial contraction against stiff ventricle (hypertensive heart disease) |
7. Blood Pressure and its Regulation
Definitions:
- Systolic BP = peak pressure during ventricular ejection (~120 mmHg)
- Diastolic BP = minimum pressure during diastole (~80 mmHg)
- Pulse pressure = Systolic - Diastolic = 40 mmHg
- Mean Arterial Pressure (MAP) = Diastolic + 1/3 Pulse Pressure = 93 mmHg
$$MAP = CO \times TPR$$
Where TPR = Total Peripheral Resistance.
Baroreceptor Reflex (Short-term BP regulation):
- Baroreceptors in the carotid sinus and aortic arch
- When BP rises → baroreceptors fire → vagus/glossopharyngeal → NTS in medulla → parasympathetics increase, sympathetics decrease → HR decreases, vasodilation → BP normalizes
- When BP falls → opposite response → HR increases, vasoconstriction
8. Blood Viscosity and Turbulent Flow (Reynolds Number)
$$Re = \frac{v \cdot d \cdot \rho}{\eta}$$
Where v = velocity, d = diameter, ρ = density, η = viscosity.
- Re < 2000: Laminar flow (normal, silent)
- Re > 2000: Turbulent flow (causes audible murmurs)
- Turbulence occurs at vessel branches, in the proximal aorta during rapid ejection
(Guyton & Hall, p. 182)
Summary Table: High-Yield CVS Facts for University Exams
| Topic | Key Fact |
|---|---|
| Normal CO | 5 L/min |
| Normal SV | ~70 mL |
| Normal HR | 72/min |
| Ejection Fraction | 55-65% |
| EDV | 120-140 mL |
| ESV | 50-70 mL |
| MAP formula | DBP + 1/3 pulse pressure |
| Poiseuille: radius effect | R ∝ 1/r⁴ (4th power!) |
| Biggest resistance vessel | Arterioles |
| Frank-Starling | ↑ EDV → ↑ SV |
| Fick principle | CO = O₂ consumption / A-V O₂ difference |
| S1 | AV valve closure (start systole) |
| S2 | Semilunar valve closure (end systole) |
| Isovolumetric phases | All valves closed, no volume change |
Typical University Long-Answer Question Pattern
Q: Describe Poiseuille's law. Explain its significance in cardiovascular physiology.
- Define the law, write the equation with all variables
- State the three relationships (especially r⁴)
- Explain why arterioles are the key resistance vessels
- Give a numerical example (radius halved → 16-fold resistance increase)
- Discuss series vs parallel resistance
- Clinical significance: atherosclerosis, hypertension, vasodilator drugs
Q: What is cardiac output? Describe its regulation.
- Define CO = HR × SV
- Normal value (5 L/min)
- Frank-Starling law for SV regulation
- Preload, afterload, contractility
- Autonomic control of HR and contractility
- Fick principle for measurement
Sources: Costanzo Physiology, 7th Ed. | Guyton and Hall Textbook of Medical Physiology | Goldman-Cecil Medicine
Also do the same for peripheral resistance
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
All the content I need is in hand. Here is the complete exam-ready guide on peripheral resistance:
PERIPHERAL RESISTANCE - Complete 1st Year MBBS Guide
1. Definition and Units
Peripheral resistance (also called Total Peripheral Resistance / TPR or Systemic Vascular Resistance / SVR) is the total resistance offered by all blood vessels in the systemic circulation to blood flow.
Unit of resistance = PRU (Peripheral Resistance Unit)
1 PRU = 1 mm Hg pressure per 1 mL/sec blood flow
In CGS units:
$$R \text{ (dyne sec/cm}^5) = 1333 \times \frac{\text{mm Hg}}{\text{mL/sec}}$$
(Guyton and Hall, p. 183)
2. The Fundamental Equation
$$TPR = \frac{MAP - CVP}{CO} \approx \frac{\Delta P}{Q}$$
Where:
- MAP = Mean Arterial Pressure (~93 mmHg)
- CVP = Central Venous Pressure (~2 mmHg, often ignored)
- CO = Cardiac Output (~100 mL/sec or 5 L/min)
$$TPR = \frac{100 \text{ mm Hg}}{100 \text{ mL/sec}} = 1 \text{ PRU (normal)}$$
Rearranged - the most exam-tested form:
$$MAP = CO \times TPR$$
This is the cardiovascular equivalent of Ohm's Law (V = IR).
| Condition | TPR value |
|---|---|
| Normal resting | ~1 PRU |
| Strong vasoconstriction (e.g., shock) | up to 4 PRU |
| Massive vasodilation | down to 0.2 PRU |
3. Where Does Peripheral Resistance Arise?
Different vessel types contribute different levels of resistance:
| Vessel | % Contribution to Total Resistance |
|---|---|
| Arterioles | ~50% - the dominant resistance vessels |
| Small arteries | ~25% |
| Capillaries | ~25% |
| Veins and venules | very small |
The arteriole is the KEY resistance vessel because:
- Its radius is small (r⁴ law gives massive resistance)
- It has abundant smooth muscle that can actively constrict or dilate
- Small changes in arteriolar tone produce dramatic changes in TPR
4. Factors Determining Peripheral Resistance
From Poiseuille's Law: $R = \frac{8\eta l}{\pi r^4}$
| Factor | Effect on Resistance | Example |
|---|---|---|
| Radius (r) - most important | R ∝ 1/r⁴ | Vasoconstriction → massive ↑ resistance |
| Viscosity (η) | R ∝ η | Polycythemia → ↑ resistance |
| Vessel length (l) | R ∝ l | Obesity → longer vessels → ↑ TPR |
5. Regulation of Peripheral Resistance
Peripheral resistance is regulated at the level of arteriolar smooth muscle by four mechanisms:
A. Neural Mechanisms (Extrinsic Control)
Sympathetic nervous system is the dominant neural regulator:
- Sympathetic noradrenaline → α₁ receptors on arteriolar smooth muscle → vasoconstriction → ↑ TPR
- Sympathetic inhibition / withdrawal → vasodilation → ↓ TPR
- Epinephrine from adrenal medulla:
- α₁ receptors → vasoconstriction (skin, gut, kidneys)
- β₂ receptors → vasodilation (skeletal muscle, heart)
The arteriole has a basal sympathetic tone (partial constriction at rest). This means the SNS can both increase resistance (further constrict) AND decrease resistance (dilate by withdrawing tone).
(Costanzo Physiology, 7th Ed.)
B. Myogenic Mechanism (Intrinsic)
"When vascular smooth muscle is stretched, it contracts."
- Sudden rise in arterial pressure → arteriole wall stretched → smooth muscle contracts → ↑ resistance → blood flow stays constant (autoregulation)
- Sudden fall in pressure → less stretch → arteriole relaxes → ↓ resistance → flow maintained
- Operates via the Law of Laplace: T = P × r (wall tension = pressure × radius)
- Important in: brain, kidneys, heart, skeletal muscle (autoregulation range: ~70-175 mmHg)
(Costanzo Physiology, p. 179)
C. Metabolic Mechanism (Intrinsic - Most Important for Active Hyperemia)
Metabolically active tissues release vasodilator metabolites that reduce arteriolar resistance and increase blood flow to match O₂ demand:
| Vasodilator Metabolite | Produced When... |
|---|---|
| CO₂ ↑ / O₂ ↓ (hypoxia) | Increased tissue metabolism |
| H⁺ (acidosis) | Anaerobic activity |
| K⁺ ↑ | Muscle contraction |
| Lactate | Exercise |
| Adenosine | Cardiac ischemia (most important in coronary) |
Examples:
- Active hyperemia: exercising skeletal muscle produces lactate → arteriolar dilation → ↑ blood flow → ↑ O₂ delivery
- Reactive hyperemia: after releasing arterial occlusion, O₂ debt repaid by burst of vasodilation
Organ-specific sensitivity:
- Coronary circulation: most sensitive to PO₂ and adenosine
- Cerebral circulation: most sensitive to PCO₂
(Costanzo Physiology, 7th Ed.; Medical Physiology - Boron & Boulpaep)
D. Endothelial Mechanisms (Paracrine)
Endothelial cells release vasoactive substances in response to blood flow shear stress and chemical signals:
| Substance | Source | Effect |
|---|---|---|
| Nitric Oxide (NO) | Endothelium (eNOS) | Vasodilation (most important) |
| Endothelin-1 (ET-1) | Endothelium | Vasoconstriction |
| Prostacyclin (PGI₂) | Endothelium | Vasodilation |
| Thromboxane A₂ | Platelets | Vasoconstriction |
Shear stress from blood flow stimulates endothelial release of NO → relaxes vascular smooth muscle → ↓ resistance.
(Boron & Boulpaep Medical Physiology; Harrison's 22nd Ed.)
E. Hormonal Mechanisms (Extrinsic)
| Hormone | Effect on Resistance | Mechanism |
|---|---|---|
| Angiotensin II | ↑ TPR (vasoconstriction) | Direct VSMC constriction |
| Vasopressin (ADH) | ↑ TPR (via V₁ receptors) | Arterial vasoconstriction |
| Noradrenaline | ↑ TPR | α₁ receptors |
| Adrenaline (low dose) | ↓ TPR in muscle | β₂ dominant |
| Adrenaline (high dose) | ↑ TPR | α₁ dominant |
| ANP (Atrial Natriuretic Peptide) | ↓ TPR (vasodilation) | Released from atria with ↑ pressure |
| Histamine | ↓ arteriolar resistance | Dilates arterioles (edema) |
| Bradykinin | ↓ arteriolar resistance | Dilates arterioles (edema) |
| Serotonin | ↑ local resistance | Vasoconstriction (hemostasis) |
(Costanzo Physiology, 7th Ed., p. 181)
6. Effect of Sympathetic Tone on Blood Flow - Pressure Curve
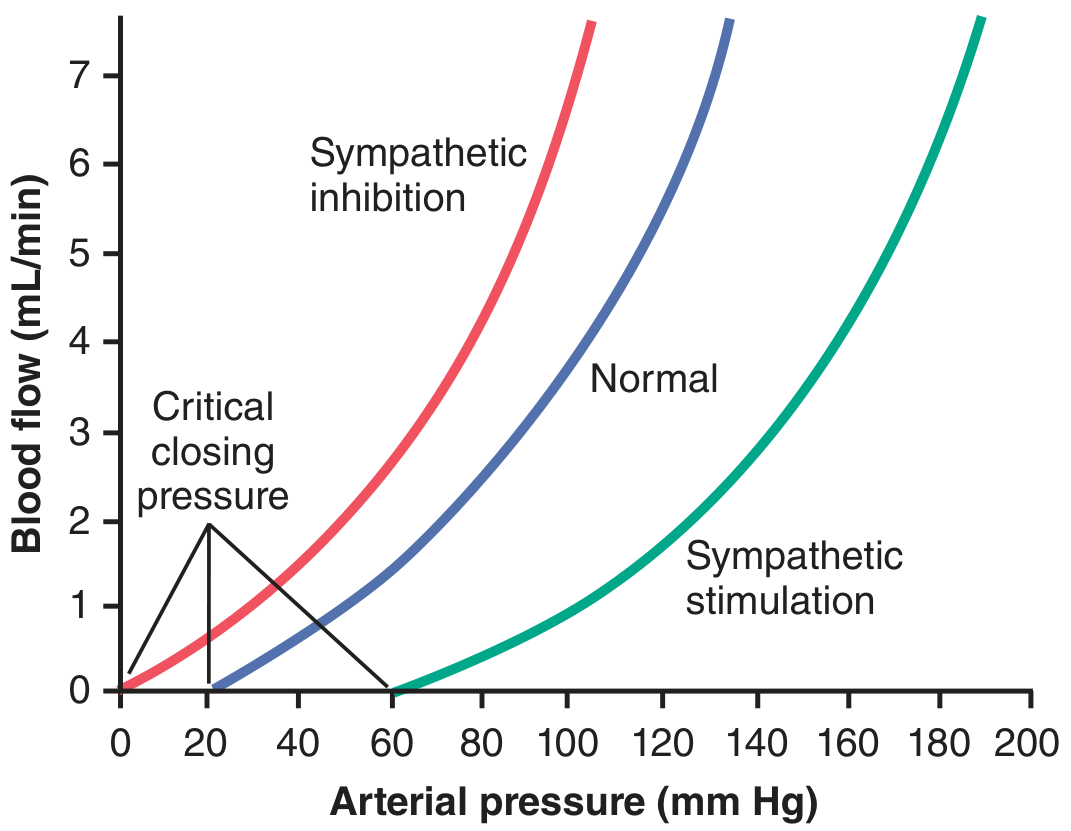
This diagram shows:
- Sympathetic stimulation (green, right): vessel constricts → more resistance → same pressure gives less flow → curve shifts right
- Normal (blue, middle): baseline
- Sympathetic inhibition (red, left): vessel dilates → less resistance → same pressure gives more flow → curve shifts left
- Critical closing pressure: the minimum pressure below which vessels collapse and flow = zero. Sympathetic stimulation raises the critical closing pressure.
(Guyton and Hall, p. 186)
7. Conductance - The Reciprocal of Resistance
$$\text{Conductance} = \frac{1}{\text{Resistance}}$$
- Conductance is measured in mL/sec per mm Hg
- Conductance ∝ Diameter⁴ (same fourth-power law)
- When vessel diameter doubles (x2), conductance increases by 2⁴ = 16-fold
- When vessel diameter quadruples (x4), conductance increases by 4⁴ = 256-fold
This is why vasodilator drugs (nitrates, calcium channel blockers) are so effective - a small increase in vessel diameter produces a huge increase in conductance and blood flow.
(Guyton and Hall, p. 183-184)
8. Autoregulation of Blood Flow
Definition: The ability of an organ to maintain constant blood flow despite changes in arterial pressure (range: ~70-175 mmHg).
Mechanisms:
- Myogenic - stretch → contract (rapid, seconds)
- Metabolic - washout of vasodilators with ↑ pressure → vasoconstriction (minutes)
Organs with strong autoregulation: Brain, kidneys, heart, skeletal muscle
Clinical significance: Even with hypertension (up to 175 mmHg), organ blood flow stays relatively constant due to autoregulation. Beyond this range, forced dilation of vessels occurs ("breakthrough perfusion"), which is dangerous (e.g., hypertensive encephalopathy).
9. Clinical Applications of Peripheral Resistance (HIGH YIELD)
| Clinical Scenario | TPR Change | Explanation |
|---|---|---|
| Hypertension | ↑ TPR | Arteriolar vasoconstriction (chronic) |
| Hypovolemic shock | ↑ TPR (compensatory) | Sympathetic activation → vasoconstriction to maintain MAP |
| Septic shock | ↓ TPR (pathological) | Massive vasodilation from cytokines/NO → hypotension |
| Exercise | ↓ TPR (skeletal muscle) | Metabolic vasodilation in exercising muscle |
| Polycythemia | ↑ TPR | ↑ blood viscosity |
| Anemia | ↓ TPR | ↓ viscosity + hypoxic vasodilation |
| ACE inhibitors | ↓ TPR | Block AngII → vasodilation → ↓ MAP |
| Calcium channel blockers | ↓ TPR | Relax arterial smooth muscle |
| Alpha-blockers | ↓ TPR | Block α₁ vasoconstriction |
10. Summary Table - High-Yield Facts for University Exams
| Fact | Value/Answer |
|---|---|
| Normal TPR | ~1 PRU |
| Unit of resistance | PRU (peripheral resistance unit) |
| Dominant resistance vessel | Arteriole |
| % contribution of arterioles | ~50% of total resistance |
| Key formula | MAP = CO × TPR |
| Conductance relationship | Conductance ∝ diameter⁴ |
| Radius-resistance relationship | R ∝ 1/r⁴ (from Poiseuille) |
| Most important vasodilator from endothelium | Nitric Oxide (NO) |
| Most important vasoconstrictor hormone | Angiotensin II |
| Autoregulation pressure range | 70-175 mmHg |
| Critical closing pressure | Pressure below which vessels collapse |
| Vasodilator metabolites | CO₂, H⁺, K⁺, adenosine, lactate |
11. Typical University Long-Answer Question
Q: What is peripheral resistance? Describe the factors regulating peripheral resistance.
Expected structure:
- Define peripheral resistance and give its unit (PRU)
- State the formula: MAP = CO × TPR
- State Poiseuille's law - role of radius (r⁴), viscosity, length
- Factors regulating resistance - use the 4 mechanisms:
- Neural (sympathetic α₁ → vasoconstriction)
- Myogenic (stretch → constriction)
- Metabolic (vasodilator metabolites)
- Endothelial (NO → vasodilation, ET-1 → constriction)
- Hormonal regulation (angiotensin II, ADH, ANP, adrenaline)
- Clinical significance (hypertension, shock, drugs)
Sources: Costanzo Physiology, 7th Ed. | Guyton and Hall Textbook of Medical Physiology | Boron & Boulpaep Medical Physiology | Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.