45 yo Single woman admitting diagnosis INVASIVE DUCTAL CARCINOMA RIGHT stage 2 B Give all the information regarding this patient About The disease The scorings ,the tables The management The pre op management Op management Post op management Comprehnsively explain
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"invasive ductal carcinoma" AND "stage II" AND management
Finding Sources
Reading File
Searching PubMed
"breast cancer" AND "neoadjuvant chemotherapy" AND surgery
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Invasive Ductal Carcinoma (IDC) Right Breast - Stage IIB
Patient: 45-year-old Single Woman
SECTION 1: THE DISEASE - WHAT IS IDC?
Definition & Classification
Invasive Ductal Carcinoma (IDC) - also called Invasive Breast Carcinoma of No Special Type (NST) - is the most common breast malignancy, accounting for ~80% of all invasive breast cancers. The term "ductal" originates from early classifications linking these tumors to ductal origin, while "no special type" distinguishes it from histologically distinct subtypes.
Unlike lobular carcinoma in situ (LCIS), ductal carcinoma in situ (DCIS) is a direct precursor to invasive ductal carcinoma. When IDC develops after untreated DCIS, it is usually an invasive ductal carcinoma in the same breast.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 978
- Schwartz's Principles of Surgery 11th ed, p. 603
Gross & Microscopic Pathology
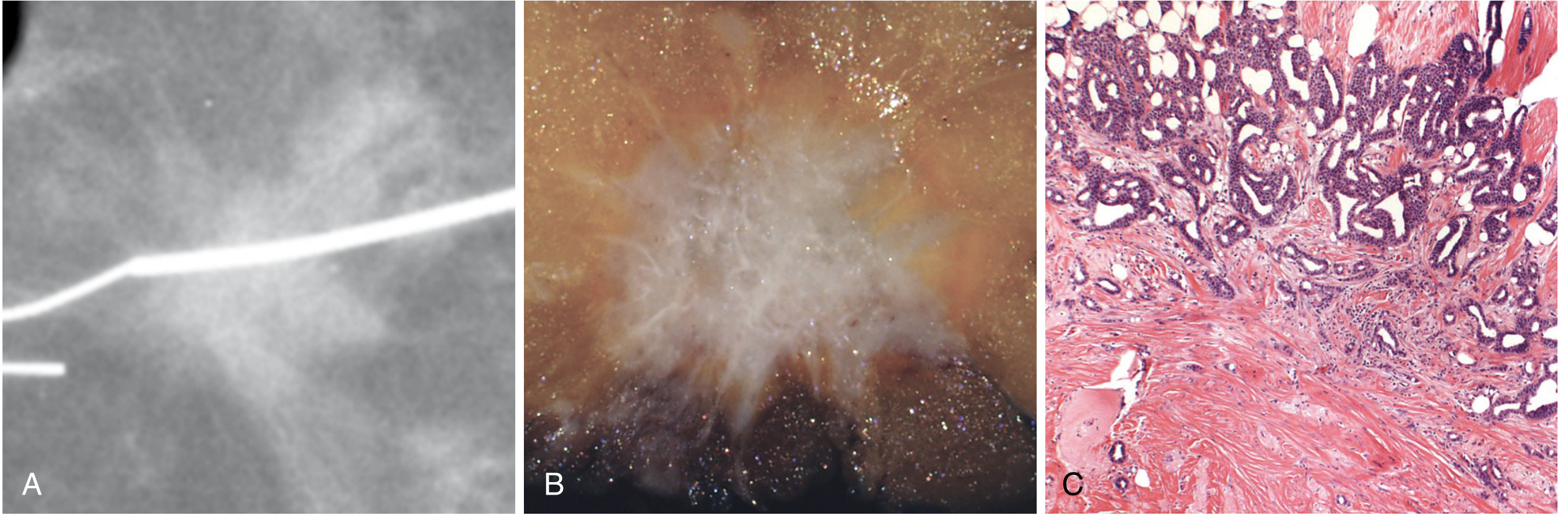
- Gross: Hard, irregular, stellate mass with gritty, chalky-white desmoplastic stroma; irregular margins on imaging and gross examination
- Microscopy: Irregular nests or sheets of pleomorphic cells invading stroma with exuberant desmoplastic response; necrosis and mitoses common in high-grade tumors
- Some IDC tumors present as well-circumscribed masses (sheets of tumor cells with scant stroma) or as scattered glands infiltrating fibrofatty tissue
SECTION 2: RISK FACTORS (Relevant to this 45-year-old woman)
| Risk Factor | Detail |
|---|---|
| Age | 45 is notable - median in Western countries ~60, but ~48 in South Asia |
| Single/Nulliparity | Nulliparity increases risk (no protective effect of early full-term pregnancy) |
| Early menarche / Late menopause | Increased estrogen exposure |
| Obesity (BMI >30) | RR = 1.29 in postmenopausal women |
| Alcohol >4 drinks/day | RR = 1.46 |
| HRT use >10 years | RR = 1.2 |
| BRCA1/BRCA2 mutation | BRCA1: 50-85% lifetime risk; BRCA2: 50-60% lifetime risk |
| No prior breastfeeding | Breastfeeding >12 months is protective |
| Age at first childbirth | Late/no first pregnancy (>35 years) increases risk |
| Family history | HBC accounts for 5-10%, FBC for 20-30% of all breast cancers |
Important for this patient: At age 45, she should be offered genetic risk evaluation - she meets criteria (breast cancer diagnosed at ≤50 years).
- Bailey and Love's Short Practice of Surgery 28th ed, p. 952
SECTION 3: STAGING - TNM SYSTEM (AJCC 8th Edition)
Stage IIB corresponds to:
| TNM Combination | Meaning |
|---|---|
| T2 N1 M0 | Tumor 2-5 cm + 1-3 positive mobile axillary LN + no distant mets |
| T3 N0 M0 | Tumor >5 cm + node negative + no distant mets |
Primary Tumor (T) Staging
| T Stage | Definition |
|---|---|
| T0 | No evidence of primary tumor |
| Tis | DCIS or Paget's without invasion |
| T1mi | ≤1 mm |
| T1a | >1 mm but ≤5 mm |
| T1b | >5 mm but ≤10 mm |
| T1c | >10 mm but ≤20 mm |
| T2 | ≥20 mm but ≤50 mm |
| T3 | ≥50 mm |
| T4a | Extension to chest wall |
| T4b | Ulceration/edema/satellite nodules of skin (not IBC) |
| T4c | Both T4a + T4b |
| T4d | Inflammatory carcinoma |
Regional Lymph Nodes - Clinical (cN)
| cN Stage | Definition |
|---|---|
| cN0 | No regional LN metastases |
| cN1 | Metastases in movable ipsilateral Level I-II axillary LN |
| cN1mi | Micrometastases (>0.2 mm but ≤2.0 mm) |
| cN2a | Axillary LN fixed/matted to each other |
| cN2b | Internal mammary LN without axillary mets |
| cN3a | Infraclavicular (Level III) LN |
| cN3c | Supraclavicular LN |
Regional Lymph Nodes - Pathologic (pN)
| pN Stage | Definition |
|---|---|
| pN0 | No LN metastasis / ITCs only |
| pN1 | 1-3 axillary LN + clinically negative internal mammary with micro/macro-mets |
| pN2 | 4-9 axillary LN |
| pN3 | ≥10 axillary LN / infraclavicular / internal mammary with axillary LN |
Distant Metastasis (M)
- M0 = No distant metastasis (this patient's stage)
- M1 = Distant metastasis present
Overall Stage Grouping
| Stage | TNM | 5-Year Survival |
|---|---|---|
| 0 | Tis N0 M0 | ~99% |
| IA | T1 N0 M0 | ~98% |
| IB | T0-1 N1mi M0 | ~98% |
| IIA | T0-1 N1 M0; T2 N0 M0 | ~91% |
| IIB | T2 N1 M0; T3 N0 M0 | ~81% |
| IIIA | T0-3 N2 M0; T3 N1 M0 | ~68% |
| IIIB | T4 N0-2 M0 | ~54% |
| IIIC | Any T N3 M0 | ~54% |
| IV | Any T Any N M1 | ~27% |
- Schwartz's Principles of Surgery 11th ed, p. 603-604
SECTION 4: HISTOLOGIC GRADING - NOTTINGHAM SCORE (Elston-Ellis)
This is the universal grading system for all invasive breast carcinomas. Three parameters are scored 1-3 each:
Scoring Parameters
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% of tumor | 10-75% | <10% |
| Nuclear pleomorphism | Small uniform nuclei | Moderate variation | Marked variation |
| Mitotic count | Depends on field area (low) | Moderate | High |
Grade Assignment (Total Score 3-9)
| Total Score | Grade | Interpretation |
|---|---|---|
| 3-5 | Grade 1 | Well differentiated - best prognosis |
| 6-7 | Grade 2 | Moderately differentiated |
| 8-9 | Grade 3 | Poorly differentiated - worst prognosis |
Grade 1: Tubular/cribriform pattern, small uniform nuclei, low mitoses
Grade 2: Solid clusters or single infiltrating cells, moderate pleomorphism
Grade 3: Ragged nests/solid sheets, enlarged irregular nuclei, high mitoses, areas of necrosis
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 978
SECTION 5: BIOMARKER SCORING / RECEPTOR STATUS
This is critical for treatment decisions in ALL IDC patients.
Receptor Subtypes and Clinical Implications
| Subtype | ER | PR | HER2 | Characteristics | Treatment |
|---|---|---|---|---|---|
| Luminal A | + | + | - | Low grade, best prognosis | Endocrine therapy ± chemo |
| Luminal B | + | +/- | +/- | Higher grade | Endocrine + chemo |
| HER2-enriched | - | - | + | Aggressive | Anti-HER2 + chemo |
| Triple Negative (TNBC) | - | - | - | Most aggressive; BRCA1 assoc | Chemo (no targeted Rx) |
HER2 Scoring (FISH/IHC)
| IHC Score | Interpretation |
|---|---|
| 0 | HER2 negative |
| 1+ | HER2 negative |
| 2+ | Equivocal → requires FISH confirmation |
| 3+ | HER2 positive |
Ki-67 Proliferation Index
| Ki-67 | Meaning |
|---|---|
| <10% | Low proliferative rate |
| 10-20% | Intermediate |
| >20% | High proliferative rate |
SECTION 6: PROGNOSTIC SCORING TOOLS
1. Oncotype DX (21-Gene RT-PCR Assay)
- Used in ER+/HER2- node-negative patients (and limited use in 1-3 node positive)
- Generates a Recurrence Score (RS):
- RS 0-10: Low risk - endocrine therapy alone (98.7% recurrence-free at 5 years)
- RS 11-25: Intermediate - endocrine ± chemotherapy
- RS >25: High risk - chemotherapy + endocrine therapy
2. MammaPrint (70-Gene Assay)
- FDA approved for Stage 1-2, node-negative, ER+ or ER- tumors
- MINDACT trial: Patients with high clinical risk but low genomic risk had 94.7% distant metastasis-free survival at 5 years without chemotherapy
- Available for FFPE tissue
3. Traditional Prognostic Factors Table
| Tumor Factors | Host Factors |
|---|---|
| Nodal status | Age |
| Tumor size | Menopausal status |
| Histologic/nuclear grade | Family history |
| Lymphovascular invasion | Previous breast cancer |
| Pathologic stage | Immunosuppression |
| Hormone receptor status | Prior chemotherapy |
| DNA ploidy/S-phase fraction | Prior radiation |
| HER2/neu expression | Nutrition |
| Extent of intraductal component | - |
- Schwartz's Principles of Surgery 11th ed, p. 607
SECTION 7: WORKUP / INVESTIGATIONS
Triple Assessment (Mandatory)
- Clinical examination - Lump characteristics (hard, irregular, fixation), nipple changes, skin changes (peau d'orange, ulceration, tethering), axillary LN
- Imaging:
- Mammography - Bilateral (two views: craniocaudal + mediolateral oblique)
- Breast ultrasound - Characterize mass, guide biopsy
- MRI breast - Assess extent of disease, contralateral breast, lymph nodes
- Pathology - Core needle biopsy (preferred over excisional biopsy)
Staging Workup for Stage IIB
| Investigation | Purpose |
|---|---|
| CT chest/abdomen/pelvis | Metastatic workup (lungs, liver, adrenals, ovaries) |
| Bone scan | Skeletal metastases (lumbar vertebrae, femur, thoracic spine, ribs, skull) |
| CBC, LFTs, ALP | Bone marrow, liver function |
| CA 15-3, CEA | Tumor markers (baseline) |
| BRCA1/BRCA2 testing | Genetic risk - MANDATORY at ≤50 years |
| Echocardiogram | Baseline cardiac function before anthracyclines |
| Receptor panel | ER, PR, HER2, Ki-67 |
| Fertility counseling | Young premenopausal woman - may need ovarian preservation |
SECTION 8: MANAGEMENT OVERVIEW
For Stage IIB (T2N1M0 or T3N0M0), treatment is multimodal:
Surgery + Chemotherapy + Radiotherapy ± Endocrine therapy ± Targeted therapy
The approach is determined by:
- Tumor size relative to breast size
- Nodal status
- Receptor subtype (ER/PR/HER2/TNBC)
- Patient's wishes, comorbidities
- BRCA status
SECTION 9: PRE-OPERATIVE MANAGEMENT
Clinical Pathway Before Surgery
A. Full Staging Workup (as above)
B. Multidisciplinary Team (MDT) Discussion
- Surgeon, medical oncologist, radiation oncologist, pathologist, radiologist, breast care nurse, reconstructive surgeon
C. Decision: Upfront Surgery vs. Neoadjuvant Chemotherapy (NACT)
| Scenario | Decision |
|---|---|
| T2N0-1, amenable to BCS | Upfront surgery |
| T3N0 (large tumor, poor BCS candidate) | NACT first to downstage |
| T2N1, triple-negative or HER2+ | Consider NACT (high response rate) |
| Locally advanced features | NACT mandatory |
Neoadjuvant Chemotherapy (NACT) for Stage IIB
Indications for NACT in this patient:
- Downstage tumor to allow breast-conserving surgery (BCS)
- Assess tumor biology and chemosensitivity in vivo
- Eradicate micrometastatic disease
Standard NACT Regimens:
| Regimen | Drugs | Cycles |
|---|---|---|
| AC-T (most common) | Doxorubicin + Cyclophosphamide → Paclitaxel | 4+4 cycles |
| TAC | Docetaxel + Doxorubicin + Cyclophosphamide | 6 cycles |
| TC | Docetaxel + Cyclophosphamide (anthracycline-sparing) | 6 cycles |
| If HER2+: Add trastuzumab ± pertuzumab | ||
| If TNBC: Pembrolizumab + AC-T (KEYNOTE-522 data) |
NACT Response Assessment:
- Breast MRI after 2-3 cycles
- Pathologic Complete Response (pCR) = no residual invasive cancer in breast or LN = excellent prognosis
D. Pre-operative Marking
- Tumor site and axillary LN marked with metal clip before NACT (in case of complete radiologic response)
- Sentinel lymph node identification planned
E. Anesthetic Assessment
- Full pre-op assessment: CBC, coagulation, renal/liver function, chest X-ray, ECG
- Cardiac echo (if anthracyclines planned)
- DVT prophylaxis planning
- Blood group & save
F. Patient Counseling
- Surgical options: BCS vs. mastectomy
- Breast reconstruction options
- Fertility preservation (patient is 45, premenopausal - ovarian reserve counseling important)
- Lymphedema risk
- Genetic testing
SECTION 10: OPERATIVE (INTRA-OPERATIVE) MANAGEMENT
Surgical Options for the Primary Tumor
A. Breast-Conserving Surgery (BCS / Lumpectomy)
Eligibility (preferred if possible for Stage IIB):
- Single tumor with adequate breast-to-tumor ratio
- No multicentric disease
- No diffuse microcalcifications suggesting DCIS
- No BRCA mutation (relative contraindication - prefer mastectomy)
- Tumor >1 cm from skin, >2 cm from nipple
- No prior breast/chest wall radiation
- No SLE or collagen vascular disease
Procedure:
- Remove tumor with 1 cm margin of normal breast tissue
- Orient specimen with sutures: "Long lateral" (L for lateral), Short superior (S for superior)
- Specimen X-ray intraoperatively to confirm excision
- Indelible India ink on specimen surfaces for margin assessment
- Negative margin = "No ink on tumor" (SSO-ASTRO 2014 consensus)
- For DCIS component: minimum 2 mm clear margin required
- Cavity shave if margins are positive
- Volume displacement oncoplasty if >20% breast volume removed
Contraindications to BCS:
- Multicentric tumor
- Diffuse microcalcifications (DCIS)
- Large tumor-to-breast ratio (volume loss >20%)
- Two positive surgical margins after re-excision
- Prior breast/chest wall radiation
- SLE or connective tissue disease
- Ankylosing spondylitis
- Severe orthopnoea (cannot lie on radiation table)
- Patient preference
B. Mastectomy
Types:
| Type | Description |
|---|---|
| Simple mastectomy | Removes breast tissue, skin, nipple-areola complex (NAC), axillary tail |
| Modified Radical Mastectomy (MRM) | Mastectomy + Level I, II, III axillary LN dissection |
| Radical mastectomy (Halsted) | MRM + both pectoralis muscles - rarely done; excessive morbidity, no survival benefit |
| Skin-sparing mastectomy | Removes breast tissue but preserves skin envelope; tumor must be >1 cm from skin |
| Nipple-sparing mastectomy | Preserves skin + NAC; tumor must be >1 cm from skin AND >2 cm from nipple |
Extent of mastectomy tissue removal:
- Superior: 2nd rib
- Medial: Parasternal edge
- Inferior: Inframammary crease
- Lateral: Anterior border of latissimus dorsi
When to choose mastectomy for this patient:
- BRCA-positive mutation
- Large tumor relative to breast (no BCS feasible)
- Patient preference for definitive removal
- Multicentric disease
C. Axillary Surgery
Step 1: Sentinel Lymph Node Biopsy (SLNB)
- Standard for clinically node-negative patients (cN0)
- Uses dual tracer: blue dye + radioisotope (Tc-99m)
- If 1-2 positive sentinel nodes (SN) AND patient is undergoing BCS with whole-breast irradiation (WBI): ALND can be omitted (ACOSOG Z0011 trial - no OS or DFS difference)
- If ≥3 positive SNs, or SNs positive in mastectomy setting: ALND required
Step 2: Axillary Lymph Node Dissection (ALND)
- Removes Level I, II, III axillary nodes
- Required for: clinically node-positive (cN2/N3), >2 positive SNs in mastectomy, or when SLNB fails
- Morbidity: lymphedema (~13% in ALND vs ~2% in SLNB alone), wound infection, seroma, paresthesias
Post-NACT Axillary Surgery:
- If N+ at diagnosis and converts to cN0 after NACT: Targeted SLNB using clipped nodes (marked pre-NACT with metal clip + India ink)
- Minimum 3 sentinel nodes should be removed; dual tracer used
- False-negative rate >10% if standard SLNB alone
D. Breast Reconstruction (if mastectomy performed)
Options:
| Type | Procedure |
|---|---|
| Implant-based | Silicone or saline implant, immediate or delayed |
| Latissimus dorsi (LD) flap | Autologous tissue from back |
| TRAM / DIEP flap | Transversus abdominis / Deep inferior epigastric perforator flap from abdomen |
| SIEA flap | Superficial inferior epigastric artery perforator flap |
For symmetry: contralateral breast may require augmentation, reduction, or mastopexy.
- Bailey and Love's 28th ed, p. 957-960
- Schwartz's Principles of Surgery 11th ed, p. 816-832
SECTION 11: POST-OPERATIVE MANAGEMENT
A. Adjuvant Chemotherapy
Indications for adjuvant chemotherapy in Stage IIB:
- Node-positive disease
- Triple-negative subtype
- HER2-positive subtype
- High Oncotype DX score (>25)
- High Ki-67, Grade 3
- Premenopausal ER+ with high risk features
If NACT was given and pCR achieved: Observation ± adjuvant endocrine therapy (if ER+)
If NACT given but residual disease:
- TNBC with residual: Capecitabine (CREATE-X trial) for 6-8 cycles
- HER2+ with residual: T-DM1 (trastuzumab emtansine) for 14 cycles
B. Adjuvant Radiotherapy (RT)
Indications (this patient - Stage IIB):
- ALL patients who had BCS (mandatory)
- Post-mastectomy if: T3/T4, N1-N3, ≥4 positive LN, positive/close margins
Fields:
- Whole breast (after BCS)
- Chest wall + supraclavicular + axillary nodal region (post-mastectomy)
- Internal mammary chain if medial tumor or N2b
- Boost to tumor bed (10-16 Gy) if high-grade or close margins
Dose:
- Conventional: 50 Gy in 25 fractions over 5 weeks + boost
- Hypofractionation: 40 Gy in 15 fractions (equivalent efficacy, fewer visits)
- Reduces locoregional recurrence and improves survival
2025 Update: Omitting regional nodal irradiation after complete response to NACT is being studied - the NSABP B-51/RTOG 1304 trial (PMID 40466065, NEJM 2025) showed potential for de-escalation.
C. Adjuvant Endocrine (Hormonal) Therapy
For ER+/PR+ disease:
| Patient Status | Drug | Duration |
|---|---|---|
| Premenopausal (this patient at 45) | Tamoxifen 20 mg/day | 5-10 years |
| Premenopausal + high risk | Tamoxifen + Ovarian Suppression (GnRH agonist: goserelin/leuprolide) | 5 years |
| Premenopausal + high risk (OFS) | Aromatase inhibitor (exemestane/anastrozole) + OFS | 5 years |
| Postmenopausal | Aromatase inhibitor (anastrozole, letrozole, exemestane) | 5-10 years |
Extended therapy (years 5-10): Letrozole (node-positive, high-risk)
D. Adjuvant Targeted Therapy
| Biomarker | Drug | Indication |
|---|---|---|
| HER2+ | Trastuzumab (Herceptin) IV | 1 year, with/after chemo |
| HER2+ high risk | Trastuzumab + Pertuzumab | Neoadjuvant + adjuvant |
| HER2+ high risk + residual disease | T-DM1 | 14 cycles post-NACT |
| BRCA1/2 mutation + HER2- | Olaparib (PARP inhibitor) | 1 year adjuvant |
| HR+/HER2-, node+, premenopausal | Abemaciclib (CDK4/6 inhibitor) | 2 years |
E. Post-Operative Wound Care & Early Recovery
- Drains: Jackson-Pratt or Blake drains placed; removed when output <30 mL/day
- Arm mobilization: Gentle shoulder exercises from Day 1-2
- Wound inspection: Daily dressing changes; suture/staple removal at 10-14 days
- DVT prophylaxis: LMWH + compression stockings for high-risk patients
- Seroma management: Aspiration if symptomatic
- Lymphedema counseling: Avoid BP cuff, blood draws, cuts on ipsilateral arm
- Pain control: Regular paracetamol ± NSAIDs; opioids if needed
F. Surveillance & Follow-Up
| Schedule | Action |
|---|---|
| Every 3-6 months × 3 years | Clinical exam, history |
| Every 6-12 months × years 4-5 | Clinical exam |
| Annually thereafter | Clinical exam |
| Annual mammography | Bilateral (or contralateral if mastectomy) |
| Annual pelvic exam | While on tamoxifen (endometrial monitoring) |
| Bone density (DEXA) | Baseline + annually if on AI |
| CA 15-3, CEA | Only if symptomatic |
| Bone scan / CT | Only if symptomatic - not routine |
SECTION 12: SPECIAL CONSIDERATIONS FOR THIS PATIENT
She is 45, Premenopausal, Single
| Issue | Action |
|---|---|
| Fertility preservation | Discuss before NACT - embryo/oocyte cryopreservation (oncofertility consult) |
| Premature menopause | NACT may cause chemotherapy-induced amenorrhea; counsel accordingly |
| Ovarian suppression | If ER+ and high risk - adds survival benefit when combined with AI |
| Bone health | If on AI + OFS: baseline DEXA, calcium + Vitamin D supplementation, bisphosphonate (zoledronic acid) |
| Psychological support | Single woman facing mastectomy - body image concerns; breast care nurse referral, psychological support |
| Genetic testing | Mandatory at ≤50 years - BRCA1/BRCA2; if positive, may need contralateral risk-reducing mastectomy |
| BRCA positive? | Bilateral risk-reducing mastectomy + BSO at 35-40 years reduces breast cancer risk by 90%, chemoprophylaxis with tamoxifen/anastrozole reduces risk by 50% |
SECTION 13: KEY LANDMARK TRIALS REFERENCED
| Trial | Key Finding |
|---|---|
| NSABP B-06 | BCS + RT = mastectomy in survival for tumors <4 cm; IBTR 14.3% (with RT) vs 39.2% (without RT) |
| Milan I | Quadrantectomy + RT = Halsted mastectomy in OS and DFS for tumors <2 cm |
| ACOSOG Z0011 | 1-2 positive SNs undergoing BCS + WBI: ALND can be omitted (no OS/DFS difference) |
| TAILORx | Oncotype DX RS 0-10: endocrine therapy alone is safe; 98.7% recurrence-free at 5 years |
| MINDACT | MammaPrint low genomic risk despite high clinical risk: 94.7% metastasis-free survival without chemo |
| NSABP B-51 (2025) | Regional nodal irradiation omission feasible after complete NACT response (PMID 40466065) |
| Mastectomy vs BCS meta-analysis (2024) | Equivalent OS; BCS + RT non-inferior to mastectomy (PMID 38758563) |
SUMMARY MANAGEMENT ALGORITHM FOR THIS PATIENT
45yo woman, IDC Right Breast Stage IIB
↓
TRIPLE ASSESSMENT + FULL STAGING WORKUP
↓
MDT Discussion
↓
ER/PR/HER2/Ki-67 / Oncotype DX (if ER+/HER2-)
↓
┌─────────────────────────────────────┐
│ Is BCS feasible upfront? │
│ (Tumor size vs breast size, │
│ single lesion, no contraindics) │
└─────────────────────────────────────┘
↓ YES ↓ NO (large tumor, BRCA+)
Upfront Surgery NACT first → Downstage
BCS + SLNB AC × 4 → T × 4 (±trastuzumab if HER2+)
↓ ↓
Post-op RT Re-assess with MRI
Adjuvant chemo → BCS or MRM + axillary surgery
Endocrine Rx
±Targeted Rx
POST-OP: RT + Endocrine Rx + Targeted Rx + Surveillance
Genetic counseling + Fertility counseling
Psychological support
Sources: Bailey and Love's Short Practice of Surgery 28th ed | Schwartz's Principles of Surgery 11th ed | Robbins, Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Fischer's Mastery of Surgery 8th ed | PubMed (PMID 38758563, 40466065, 38141462)
Add birads scoring also in the table part and reprint take most of the info from Surgical medical books
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have all the BI-RADS data from Bailey and Love's and Fischer's Mastery of Surgery. Let me compile the full reprinted comprehensive guide.
INVASIVE DUCTAL CARCINOMA (IDC) - RIGHT BREAST, STAGE IIB
Patient: 45-Year-Old Single Woman - Comprehensive Clinical Guide
SECTION 1: THE DISEASE - INVASIVE DUCTAL CARCINOMA
Definition
Invasive Ductal Carcinoma (IDC) - formally termed Invasive Breast Carcinoma of No Special Type (NST) - is the most common primary breast malignancy, accounting for ~80% of all invasive breast cancers. The term "ductal" originated from early classification systems linking these tumors to ductal origin. To qualify as a "special type" carcinoma, ≥90% of the tumor must show defining histologic features; all others are NST.
DCIS is a direct precursor - when invasive carcinoma develops after untreated DCIS, it is virtually always an IDC in the same breast.
- Schwartz's Principles of Surgery 11th ed, p. 603
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 978
Epidemiology
-
Breast cancer is the most frequent cancer among women: 2.3 million new cases worldwide in 2020, representing ~25% of all cancers in women
-
Incidence: 27/100,000 in Middle Africa vs. 92/100,000 in North America
-
In Western Europe: ~1 in 9 women will develop breast cancer
-
Lifetime risk for an American woman: 1 in 8
-
75% of breast cancers are diagnosed after age 50 (this patient at 45 is relatively young)
-
~12% of all breast cancers are caused by germline mutations; BRCA1/BRCA2 account for half
-
Bailey and Love's Short Practice of Surgery 28th ed, p. 952
-
Robbins & Kumar Basic Pathology, p. 719
Histopathology
| Feature | IDC / NST Description |
|---|---|
| Gross appearance | Hard, irregular, stellate mass; chalky-white desmoplastic stroma; grating sound on cut surface |
| Microscopy | Haphazard stromal invasion producing irregular margins; exuberant desmoplastic response |
| Low-grade (G1) | Tubular/cribriform pattern; small uniform nuclei; low mitoses |
| Intermediate (G2) | Solid clusters or single infiltrating cells; moderate nuclear pleomorphism |
| High-grade (G3) | Ragged nests/solid sheets; enlarged irregular nuclei; high mitoses; tumor necrosis; TILs |
Classification of Invasive Breast Cancer (Foote & Stewart)
| Type | Frequency |
|---|---|
| Invasive Ductal Carcinoma (NST) | ~80% |
| Invasive Lobular Carcinoma | ~10% |
| Medullary carcinoma | ~4% |
| Tubular carcinoma | ~2% |
| Mucinous (colloid) carcinoma | ~2% |
| Papillary carcinoma | ~2% |
| Rare (adenoid cystic, squamous, apocrine) | <1% |
- Schwartz's Principles of Surgery 11th ed, p. 603
SECTION 2: RISK FACTORS
| Risk Factor | Relative Risk | Notes |
|---|---|---|
| Obesity (BMI >30) | RR = 1.29 | Postmenopausal women |
| Nulliparity / first pregnancy >35 yrs | Elevated | This patient - single, likely nulliparous |
| No breastfeeding | Elevated | >12 months breastfeeding is protective |
| HRT use >10 years | RR = 1.2 | High-estrogen HRT |
| Tobacco ≥25 cigarettes/day | RR = 1.14 | |
| Alcohol - light (<1 drink/day) | RR = 1.05 | |
| Alcohol - moderate (3-4 drinks/day) | RR = 1.32 | |
| Alcohol - heavy (>4 drinks/day) | RR = 1.46 | |
| Radiation exposure | RR = 6 | Prior chest/mantle radiation |
| BRCA1 mutation (17q21) | 50-85% lifetime risk | Also 40% ovarian cancer risk |
| BRCA2 mutation (13q12.3) | 50-60% lifetime risk | Also 20% ovarian cancer risk |
| Family history (FBC) | Elevated | 20-30% of all breast cancers |
| Previous breast cancer / DCIS / LCIS | Elevated | LCIS = marker + precursor |
| Dense breasts | Elevated | Reduces mammography sensitivity |
| Early menarche / late menopause | Elevated | Extended estrogen exposure |
This patient at 45 years: Genetic risk evaluation is MANDATORY (breast cancer ≤50 years is a criterion). - Bailey and Love's 28th ed, p. 952
SECTION 3: TRIPLE ASSESSMENT
The cornerstone of breast cancer diagnosis is the triple assessment:
| Component | What It Includes |
|---|---|
| 1. Clinical assessment | History + physical examination |
| 2. Radiological assessment | Mammography + Ultrasound ± MRI |
| 3. Pathological assessment | Core needle biopsy (preferred) / FNA |
All three components must be concordant before a definitive diagnosis is made. Discordance between any two requires repeat assessment or excisional biopsy.
SECTION 4: BI-RADS SCORING SYSTEM
Background
The American College of Radiology (ACR) developed the Breast Imaging Reporting and Data System (BI-RADS) to achieve uniformity and objectivity in the interpretation and reporting of mammograms, ultrasound, and MRI.
Mammography views: Craniocaudal (CC) + Mediolateral Oblique (MLO) - at least two views per breast under compression.
BI-RADS Breast Composition Categories (Density)
| Category | Description | Clinical Significance |
|---|---|---|
| A | Almost entirely fatty | High mammography sensitivity |
| B | Scattered areas of fibroglandular density | Good sensitivity |
| C | Heterogeneously dense | May obscure small masses |
| D | Extremely dense | Lowers sensitivity of mammography - supplemental US/MRI needed |
- Fischer's Mastery of Surgery 8th ed, p. 1406
BI-RADS Assessment Categories - COMPLETE TABLE
| Category | Assessment | Probability of Malignancy | Management / Follow-up Recommendation |
|---|---|---|---|
| 0 | Incomplete - Need additional imaging / prior comparison | Not applicable | Recall for additional imaging (diagnostic mammogram, US, MRI) or comparison with prior films |
| 1 | Negative - No abnormality found | Essentially 0% | Routine annual screening mammography (women >40 years) |
| 2 | Benign finding(s) - e.g., simple cyst, fibroadenoma, lymph node | Essentially 0% | Routine annual screening mammography |
| 3 | Probably benign finding | >0% but ≤2% | Initial short-term follow-up at 6 months; if stable × 2 years, return to routine screening |
| 4a | Suspicious - Low suspicion for malignancy | >2% to ≤10% | Tissue diagnosis (biopsy) |
| 4b | Suspicious - Intermediate suspicion | >10% to ≤50% | Tissue diagnosis (biopsy) |
| 4c | Suspicious - High suspicion (moderate concern) | >50% to <95% | Tissue diagnosis (biopsy) |
| 5 | Highly suggestive of malignancy | ≥95% | Requires biopsy or surgical treatment |
| 6 | Known biopsy-proven malignancy | Not applicable | Reserved for pre-treatment planning (e.g., before NACT or surgery); surgical excision when clinically appropriate |
- Bailey and Love's Short Practice of Surgery 28th ed - Table 58.1, p. 938
- Fischer's Mastery of Surgery 8th ed - Table 52.3, p. 1409
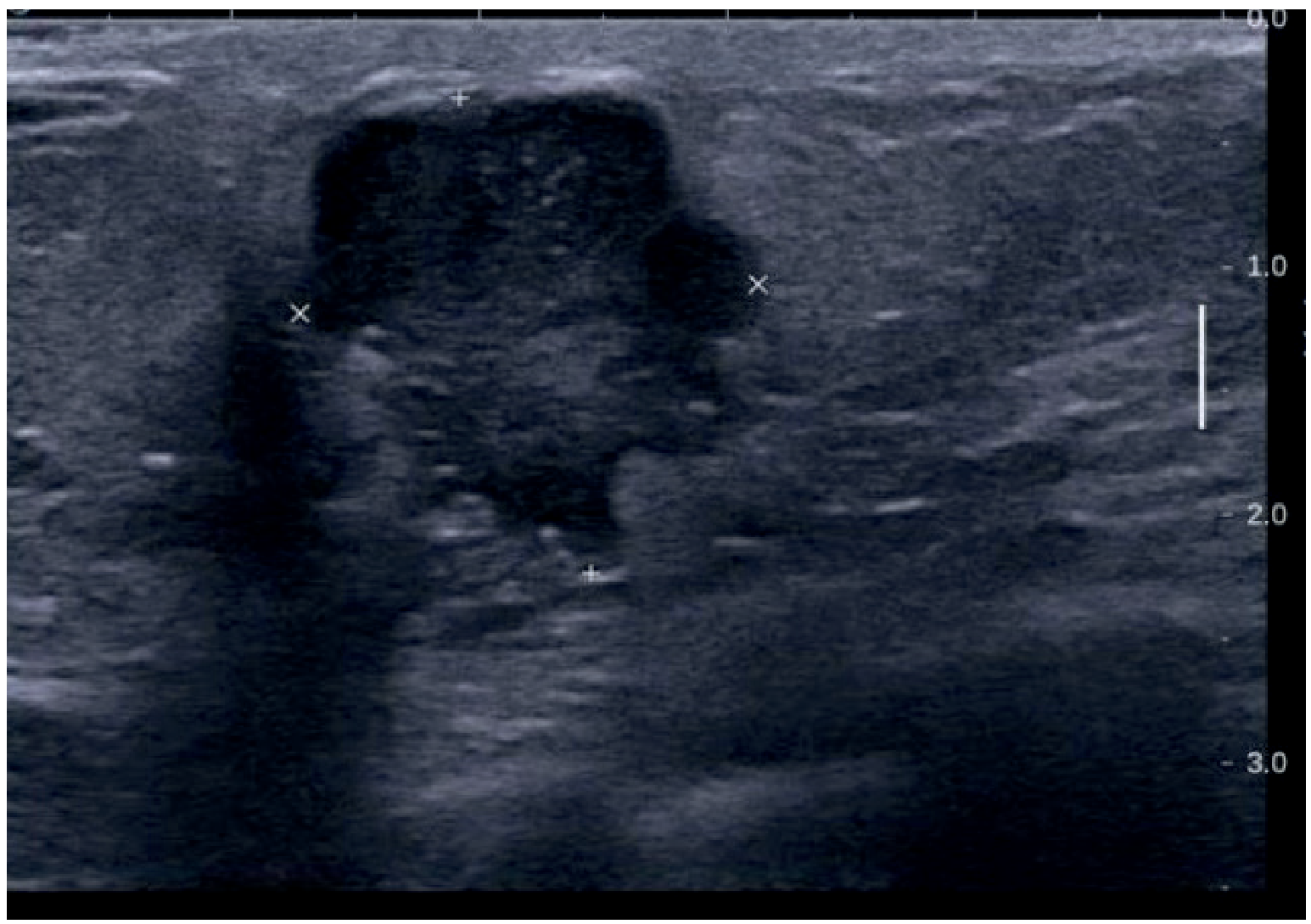
This patient's imaging: A solid, irregular-shaped mass, taller than wider, with angular/spiculated irregular margins on ultrasound = BI-RADS 5 → Requires biopsy / surgical treatment. Once biopsy confirms IDC, the category upgrades to BI-RADS 6 throughout the pre-operative/NACT phase.
Mammographic & Ultrasound Features of Breast Carcinoma
| Feature | Benign (BI-RADS 2-3) | Malignant (BI-RADS 4-5) |
|---|---|---|
| Shape | Round, oval, circumscribed | Irregular, angular, stellate |
| Margins | Well-defined, smooth | Spiculated, indistinct, microlobulated |
| Density | Equal or low density | High density |
| Orientation (US) | Wider than tall (parallel) | Taller than wide (non-parallel) |
| Posterior features (US) | Through-transmission (cyst) | Shadowing |
| Calcifications | Coarse, vascular | Fine pleomorphic / linear / segmental |
| Skin/nipple | Normal | Thickening, retraction |
| Lymph nodes | Fatty hilum preserved | Round, hypoechoic, hilum lost |
When to Use MRI of Breast
- Dense breasts or discordant/equivocal mammogram/US findings
- Distinguish scar from recurrence after BCS
- Assess extent before surgery / contralateral breast assessment
- Monitor response to NACT
- BRCA-positive women (annual screening)
- Any abnormality on MRI not seen on mammography requires focused ultrasound
SECTION 5: TNM STAGING (AJCC 8th Edition)
Stage IIB = T2N1M0 or T3N0M0
Primary Tumor (T)
| T Category | Definition |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis (DCIS) | Ductal carcinoma in situ |
| Tis (Paget) | Paget's disease without invasive carcinoma |
| T1mi | ≤1 mm |
| T1a | >1 mm but ≤5 mm |
| T1b | >5 mm but ≤10 mm |
| T1c | >10 mm but ≤20 mm |
| T2 | ≥20 mm but ≤50 mm |
| T3 | >50 mm |
| T4a | Extension to chest wall (not pectoralis muscle alone) |
| T4b | Ulceration / ipsilateral macroscopic satellite nodules / skin edema (peau d'orange) |
| T4c | T4a + T4b |
| T4d | Inflammatory carcinoma |
Regional Lymph Nodes - Clinical (cN)
| cN Category | Definition |
|---|---|
| cNX | Cannot be assessed |
| cN0 | No regional LN metastases |
| cN1 | Metastases in movable ipsilateral Level I-II axillary LN |
| cN1mi | Micrometastases (>0.2 mm but ≤2.0 mm, ~200 cells) |
| cN2a | Ipsilateral Level I-II axillary LN fixed/matted |
| cN2b | Ipsilateral internal mammary LN without axillary involvement |
| cN3a | Ipsilateral infraclavicular (Level III) LN |
| cN3b | Internal mammary + Level I-II axillary LN |
| cN3c | Ipsilateral supraclavicular LN |
Regional Lymph Nodes - Pathologic (pN)
| pN Category | Definition |
|---|---|
| pNX | Cannot be assessed |
| pN0 | No LN metastasis / ITCs only |
| pN0(i+) | Isolated tumor cells ≤0.2 mm |
| pN0(mol+) | RT-PCR positive; no ITCs |
| pN1 | Micrometastases; or 1-3 axillary LN; and/or clinically negative internal mammary + SLN micro/macrometastases |
| pN1mi | Micrometastases >0.2 mm but ≤2.0 mm |
| pN2 | 4-9 axillary LN |
| pN3 | ≥10 axillary LN / infraclavicular / internal mammary + axillary |
Distant Metastasis (M)
- M0 = No clinical/radiographic distant metastasis
- cM0(i+) = Circulating tumor cells detected, no clinical metastasis
- M1 = Distant metastasis
Overall Stage Grouping
| Stage | TNM | Approx. 5-Year Survival |
|---|---|---|
| 0 | Tis N0 M0 | ~99% |
| IA | T1 N0 M0 | ~98% |
| IB | T0-1 N1mi M0 | ~98% |
| IIA | T0-1 N1 / T2 N0 M0 | ~91% |
| IIB | T2 N1 M0 / T3 N0 M0 | ~81% |
| IIIA | T0-3 N2 / T3 N1 M0 | ~68% |
| IIIB | T4 N0-2 M0 | ~54% |
| IIIC | Any T N3 M0 | ~54% |
| IV | Any T Any N M1 | ~27% |
- Schwartz's Principles of Surgery 11th ed, p. 603-604
SECTION 6: HISTOLOGIC GRADING - NOTTINGHAM HISTOLOGIC SCORE (Elston-Ellis)
All invasive carcinomas are graded using this system.
Scoring
| Parameter | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | >75% of tumor forms tubules | 10-75% | <10% |
| Nuclear pleomorphism | Small, regular, uniform nuclei | Moderate size/shape variation | Marked variation, prominent nucleoli |
| Mitotic count | Low (field-area dependent) | Moderate | High |
Grade Assignment
| Total Score (3-9) | Grade | Differentiation | Prognosis |
|---|---|---|---|
| 3-5 | Grade 1 | Well differentiated | Best |
| 6-7 | Grade 2 | Moderately differentiated | Intermediate |
| 8-9 | Grade 3 | Poorly differentiated | Worst |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 978
SECTION 7: RECEPTOR / BIOMARKER STATUS - MOLECULAR SUBTYPES
Receptor Testing (Every IDC Must Have This)
| Receptor | Test Method | Positive Threshold | Clinical Implication |
|---|---|---|---|
| ER (Estrogen Receptor) | IHC | ≥1% nuclear staining | Eligible for endocrine therapy |
| PR (Progesterone Receptor) | IHC | ≥1% nuclear staining | Adjunct prognostic value |
| HER2 | IHC → FISH if 2+ | IHC 3+ OR FISH amplified | Eligible for anti-HER2 therapy |
| Ki-67 | IHC | >20% = high proliferation | Indicates benefit from chemo |
HER2 IHC Scoring
| IHC Score | Interpretation | Action |
|---|---|---|
| 0 | Negative | No anti-HER2 therapy |
| 1+ | Negative | No anti-HER2 therapy |
| 2+ | Equivocal | Proceed to FISH |
| 3+ | Positive | Eligible for trastuzumab |
Molecular Subtypes
| Subtype | ER | PR | HER2 | Grade | Characteristics | Preferred Treatment |
|---|---|---|---|---|---|---|
| Luminal A | + | + | - | Low | Best prognosis; low Ki-67 | Endocrine therapy alone |
| Luminal B (HER2-) | + | Low/- | - | High | Higher Ki-67; moderate risk | Endocrine + chemotherapy |
| Luminal B (HER2+) | + | +/- | + | Any | Higher risk | Endocrine + chemo + anti-HER2 |
| HER2-enriched | - | - | + | High | Aggressive | Anti-HER2 + chemotherapy |
| Triple Negative (TNBC) | - | - | - | Usually 3 | Most aggressive; BRCA1-associated | Chemotherapy (no targeted Rx available) |
SECTION 8: PROGNOSTIC SCORING TOOLS
1. Oncotype DX (21-Gene RT-PCR Assay)
Used in ER+/HER2- node-negative patients (and retrospective data in 1-3 node positive):
| Recurrence Score | Risk Category | Treatment |
|---|---|---|
| 0-10 | Low risk | Endocrine therapy alone; 98.7% recurrence-free at 5 years (TAILORx) |
| 11-25 | Intermediate | Endocrine therapy ± chemotherapy |
| >25 | High risk | Chemotherapy + endocrine therapy |
2. MammaPrint (70-Gene Assay)
FDA approved for Stage 1-2, node-negative, ER+ or ER- tumors:
- Low genomic risk despite high clinical risk: 94.7% distant metastasis-free survival at 5 years without chemotherapy (MINDACT trial)
- Available for FFPE tissue
3. Traditional Prognostic Factors
| Tumor Factors | Host Factors |
|---|---|
| Nodal status | Age |
| Tumor size | Menopausal status |
| Histologic grade | Family history |
| Lymphovascular invasion | Previous breast cancer |
| Hormone receptor status | Immunosuppression |
| HER2/neu expression | Prior chemotherapy/RT |
| DNA ploidy / S-phase fraction | Nutritional status |
| Extent of intraductal component | - |
- Schwartz's Principles of Surgery 11th ed, p. 607
SECTION 9: INVESTIGATIONS / WORKUP SUMMARY
Full Pre-Treatment Workup for Stage IIB
| Investigation | Purpose |
|---|---|
| Bilateral mammography (CC + MLO) | Characterize lesion, contralateral breast |
| Breast ultrasound | Lesion characterization; axillary LN assessment; guide biopsy |
| MRI breast | Extent of disease, contralateral breast, multifocality |
| Core needle biopsy | Tissue diagnosis (preferred over excisional biopsy) |
| ER / PR / HER2 / Ki-67 | Molecular subtype |
| Oncotype DX / MammaPrint | Chemotherapy decision in ER+/HER2- |
| CT chest / abdomen / pelvis | Metastatic workup (lung, liver, adrenals) |
| Bone scan | Skeletal metastases |
| Blood tests | CBC, LFT, ALP, renal function, Ca2+ |
| Tumor markers | CA 15-3, CEA (baseline) |
| BRCA1/BRCA2 testing | Mandatory at ≤50 years |
| Echocardiogram | Baseline cardiac function before anthracyclines |
| Fertility counseling | Premenopausal woman before NACT |
| Bone density (DEXA) | Before AI therapy |
SECTION 10: PRE-OPERATIVE MANAGEMENT
A. Multidisciplinary Team (MDT) Discussion - Mandatory
Members: Surgeon, medical oncologist, radiation oncologist, pathologist, radiologist, breast care nurse, reconstructive surgeon, genetic counselor, oncofertility specialist
B. Neoadjuvant Chemotherapy (NACT)
Indications for NACT in this Stage IIB patient:
- Downstage tumor to convert to BCS-eligible
- Assess in-vivo chemosensitivity
- Eradicate occult micrometastases early
- pCR = excellent prognostic marker
Standard NACT Regimens:
| Regimen | Drugs | Cycles | Indication |
|---|---|---|---|
| AC → T | Doxorubicin + Cyclophosphamide × 4 → Paclitaxel × 4 | 8 cycles | Standard for most IDC |
| TAC | Docetaxel + Doxorubicin + Cyclophosphamide | 6 cycles | |
| TC | Docetaxel + Cyclophosphamide | 6 cycles | Anthracycline-sparing |
| AC → THP | AC × 4 → Paclitaxel + Trastuzumab + Pertuzumab × 4 | 8 cycles | HER2+ |
| Pembrolizumab + AC → T | Immunotherapy + chemo | TNBC (KEYNOTE-522) |
Response Assessment: Breast MRI after 2-3 cycles; reassess surgical options.
C. Pre-NACT Preparations
- Metal clip placed in tumor and any positive axillary LN (targeted SLNB post-NACT)
- Permanent India ink tattoo of positive LN if clip not available
- Oncofertility referral: Embryo/oocyte cryopreservation before NACT starts
- Baseline echo (anthracycline cardiotoxicity)
- BRCA testing result must be available before surgery planning
D. Anaesthetic Pre-operative Assessment
- CBC, coagulation profile, renal/hepatic function, blood sugar
- Chest X-ray, 12-lead ECG
- Blood group and screen
- DVT risk stratification (Caprini score) → LMWH + compression stockings plan
- Lung function if indicated
- Nutritional assessment
E. Patient Counseling Before Surgery
- Choice between BCS and mastectomy
- Reconstruction options (immediate vs. delayed)
- Sentinel node biopsy vs. ALND
- Lymphedema risk and prevention
- Chemotherapy side-effects (alopecia, nausea, fatigue, premature menopause)
- Fertility implications
- Psychological support / body image
- Genetic testing results discussion
SECTION 11: OPERATIVE (INTRA-OPERATIVE) MANAGEMENT
Decision Matrix: BCS vs. Mastectomy
| Factor | Favors BCS | Favors Mastectomy |
|---|---|---|
| Tumor size vs. breast | Small-medium, good ratio | Large tumor/small breast, poor ratio |
| Focality | Unifocal | Multicentric |
| Calcifications | Localized | Diffuse on mammogram |
| BRCA status | Negative | BRCA positive |
| Margins | Achievable | Previous positive margins |
| Prior radiation | None | Previous breast/chest wall RT |
| Connective tissue disease | Absent | SLE, ankylosing spondylitis |
| Patient preference | BCS preferred | Mastectomy preferred |
| NACT response | Good downstaging | No response / persistent large tumor |
A. Breast-Conserving Surgery (BCS / Lumpectomy / WLE)
Procedure:
- Mark tumor site preoperatively (wire-guided or radioactive seed localization if impalpable)
- Place curvilinear/concentric incision in upper breast; radial incisions in lower breast
- Excise tumor with 1 cm margin of normal breast tissue
- Orient specimen: Long suture = Lateral ("L for Lateral"); Short suture = Superior ("S for Superior")
- Intraoperative specimen X-ray to confirm excision
- Apply indelible India ink to all specimen surfaces
- Negative margin = "No ink on tumor" (SSO-ASTRO 2014 consensus: wider margins do not reduce IBTR in invasive cancer)
- For any DCIS component: minimum 2 mm clear margin required
- If margin involved → cavity shave re-excision
- Volume loss ≤20%: Direct tissue approximation with absorbable sutures
- Volume loss >20% → Oncoplastic procedure required
Oncoplastic Options:
| Level | Technique | Indication |
|---|---|---|
| Level 1 (Volume displacement) | Dermoglandular pillar mobilization; therapeutic mammoplasty; round-block | Up to 20-30% volume loss |
| Level 2 (Volume replacement) | Local/distant flap (latissimus dorsi mini-flap, LICAP, TDAP) | >30% volume loss |
Contraindications to BCS (from Bailey and Love's):
- Multicentric tumor
- Diffuse microcalcifications on mammogram
- Large tumor-to-breast ratio
- Two positive surgical margins after re-excision
- Previous breast/chest wall radiation
- SLE or connective tissue disease
- Ankylosing spondylitis
- Severe orthopnoea (cannot lie on radiation table)
- Patient preference
B. Mastectomy
Types Compared:
| Operation | What Is Removed | Indication |
|---|---|---|
| Simple / Total mastectomy | All breast tissue + skin + NAC + axillary tail | Prophylactic; DCIS; when axillary surgery done separately |
| Modified Radical Mastectomy (MRM) | Mastectomy + Level I-II-III axillary LN dissection | Standard for node-positive disease requiring mastectomy |
| Skin-sparing mastectomy | Breast tissue + NAC; skin envelope preserved | Reconstruction planned; tumor >1 cm from skin |
| Nipple-sparing mastectomy | Breast tissue only; skin + NAC preserved | Tumor >1 cm from skin AND >2 cm from nipple |
| Radical (Halsted) mastectomy | Breast + all axillary LN + both pectoralis muscles | Rarely done; no survival benefit; excessive morbidity |
Extent of Simple Mastectomy (Bailey and Love's):
- Superior: 2nd rib (where anterior premammary fascia fuses with posterior pectoral fascia)
- Medial: Parasternal edge
- Inferior: Inframammary crease
- Lateral: Anterior border of latissimus dorsi
MRM adds: Removal of Level I, II, and III axillary lymph nodes.
C. Axillary Surgery
Step 1 - Sentinel Lymph Node Biopsy (SLNB):
- Dual tracer: patent blue dye + Tc-99m radioisotope
- First draining node(s) from primary tumor
- If 1-2 positive SNs + BCS + whole-breast irradiation (WBI): ALND omitted - ACOSOG Z0011 trial showed no difference in OS (91.9% vs 92.5%) or DFS (82.2% vs 83.8%) at 6-year follow-up
- ALND still required if: ≥3 positive SNs, positive SN with mastectomy, clinically node-positive
Post-NACT Targeted SLNB (for initially N+ patients):
- Requires ≥3 sentinel nodes removed
- Dual tracers mandatory
- Clipped node must be identified and removed
- Standard SLNB alone has false-negative rate >10%; targeted technique reduces this
Step 2 - Axillary Lymph Node Dissection (ALND):
- Removes Level I, II, III nodes
- Complications: Lymphedema (13% ALND vs 2% SLNB alone), wound infection, seroma (7.1%), axillary hematoma (1.4%), paresthesias (8.6%), reduced shoulder range of motion
D. Breast Reconstruction
| Type | Technique | Notes |
|---|---|---|
| Implant-based | Silicone/saline implant ± tissue expander | Immediate or delayed; simplest |
| Latissimus Dorsi (LD) flap | Autologous muscle + skin from back | Reliable; can combine with implant |
| TRAM flap | Transversus abdominis myocutaneous flap from abdomen | Pedicled or free |
| DIEP flap | Deep inferior epigastric perforator flap | Muscle-sparing free flap; best cosmesis |
| SIEA flap | Superficial inferior epigastric artery | Least donor morbidity |
Contralateral symmetrization: Augmentation, reduction mammoplasty, or mastopexy may be required. Patient should be informed multiple procedures may be needed.
- Bailey and Love's 28th ed, p. 957-962
SECTION 12: POST-OPERATIVE MANAGEMENT
A. Immediate Post-Op (Ward Management)
| Issue | Management |
|---|---|
| Wound drains | Jackson-Pratt / Blake drains; remove when output <30 mL/24h (typically 2-5 days) |
| Seroma | Most common complication; aspiration if symptomatic (needle aspiration in clinic) |
| Wound inspection | Daily dressing; suture/staple removal at 10-14 days |
| Pain control | Paracetamol + NSAIDs regular; opioids PRN; avoid excessive opioids post-day 2 |
| DVT prophylaxis | LMWH + TED stockings until fully mobile |
| Arm mobilization | Gentle shoulder/arm exercises from Day 1-2 to prevent frozen shoulder |
| Lymphedema education | Avoid BP cuff, venepuncture, IV lines on ipsilateral arm; avoid cuts/infections |
B. Pathology Report Assessment
After surgery, pathologist reports:
- Tumor size (pathologic T)
- Grade (Nottingham score)
- Margins status (distance to nearest inked margin)
- Number of nodes examined / positive nodes
- Lymphovascular invasion (LVI)
- Pathologic stage (ypTNM if post-NACT)
- Pathologic Complete Response (pCR): No residual invasive cancer in breast or nodes
C. Adjuvant Radiotherapy (RT)
| Indication | RT Field |
|---|---|
| All BCS patients | Whole breast RT (mandatory; NSABP B-06) |
| Post-mastectomy T3/T4 | Chest wall + supraclavicular nodes |
| Post-mastectomy N1-N3 | Chest wall + nodal basins |
| Medial tumors / N2b | Include internal mammary chain |
| High-grade / close margins | Tumor bed boost (10-16 Gy) |
Dose:
- Conventional: 50 Gy in 25 fractions × 5 weeks + boost
- Hypofractionation: 40 Gy in 15 fractions (equivalent efficacy, fewer visits)
Benefits: Reduces locoregional recurrence; improves disease-free and overall survival.
D. Adjuvant Chemotherapy
| Indication | Regimen |
|---|---|
| Node-positive disease | AC × 4 → T × 4 (or TAC × 6) |
| HER2+ | Add trastuzumab (± pertuzumab) to above |
| TNBC residual disease post-NACT | Capecitabine × 6-8 cycles |
| HER2+ residual disease post-NACT | T-DM1 (trastuzumab emtansine) × 14 cycles |
E. Adjuvant Endocrine (Hormonal) Therapy
For ER+ and/or PR+ tumors (most common IDC subtype):
| Patient Status | Drug | Duration |
|---|---|---|
| Premenopausal - standard risk | Tamoxifen 20 mg/day | 5-10 years |
| Premenopausal - high risk | Tamoxifen + GnRH agonist (goserelin / leuprolide) = Ovarian Function Suppression (OFS) | 5 years |
| Premenopausal - highest risk | Aromatase inhibitor (exemestane / anastrozole) + OFS | 5 years |
| Postmenopausal | AI (anastrozole / letrozole / exemestane) | 5-10 years |
This 45-year-old patient: Premenopausal → Tamoxifen ± OFS. Monitor for endometrial thickening (annual pelvic exam). If NACT induces amenorrhea, reassess menopausal status before switching to AI.
Side effects of tamoxifen: Hot flushes, endometrial cancer risk, DVT/PE risk, vaginal discharge.
F. Adjuvant Targeted Therapy
| Target | Drug | Indication | Duration |
|---|---|---|---|
| HER2 | Trastuzumab (Herceptin) | HER2+ any stage | 1 year IV infusions |
| HER2+ high risk | Trastuzumab + Pertuzumab | Neo/adjuvant | 1 year |
| HER2+ residual post-NACT | T-DM1 (ado-trastuzumab emtansine) | Replaces trastuzumab | 14 cycles |
| BRCA1/2 germline mutation | Olaparib (PARP inhibitor) | HER2-, high risk | 1 year adjuvant |
| HR+/HER2-, node+, premenopausal | Abemaciclib (CDK4/6 inhibitor) | High Ki-67 | 2 years |
G. Surveillance Schedule
| Time Point | Action |
|---|---|
| Every 3-6 months × 3 years | Clinical history + physical examination |
| Every 6-12 months × years 4-5 | Clinical exam |
| Annually thereafter (lifelong) | Clinical exam |
| Annual mammography | Bilateral (or remaining breast if mastectomy) |
| Annual pelvic exam | While on tamoxifen (endometrial monitoring) |
| DEXA bone density | Baseline + annually if on AI + OFS |
| Calcium + Vitamin D | If on AI + OFS (bone protection) |
| Zoledronic acid | If bone density declining on AI + OFS |
| Tumor markers (CA 15-3, CEA) | Only if symptomatic - not routine surveillance |
| CT scan / bone scan | Only if symptomatic - not routine |
SECTION 13: SPECIAL CONSIDERATIONS FOR THIS 45-YEAR-OLD SINGLE WOMAN
| Issue | Recommended Action |
|---|---|
| Age ≤50 = Mandatory genetic testing | BRCA1/BRCA2 testing before surgery |
| BRCA positive finding | Offer bilateral risk-reducing mastectomy (reduces risk by 90%) + BSO at completion of family (35-40 yrs); chemoprophylaxis: tamoxifen or anastrozole reduces risk 50% |
| Fertility preservation | Oncofertility referral BEFORE starting NACT; embryo or oocyte cryopreservation |
| Premature menopause from NACT | Chemotherapy-induced amenorrhea is common; reassess before starting AI |
| OFS + AI combination | Best endocrine therapy for high-risk premenopausal ER+ if amenable; add DEXA, calcium, Vit D, bisphosphonate |
| Body image / psychological | Breast care nurse referral; psycho-oncology referral; single patient may have specific support needs |
| BRCA+ + premenopausal | Discuss bilateral salpingo-oophorectomy (BSO) after family completed at ~35-40 years - also reduces ovarian cancer risk and improves breast-specific survival |
SECTION 14: KEY LANDMARK TRIALS
| Trial | Finding |
|---|---|
| NSABP B-06 | BCS + RT equivalent to mastectomy in OS/DFS for tumors <4 cm; IBTR: 14.3% (with RT) vs 39.2% (no RT) |
| Milan I | Quadrantectomy + RT = Halsted mastectomy (OS/DFS) for <2 cm tumors |
| ACOSOG Z0011 | 1-2 positive SNs + BCS + WBI: ALND can be omitted; no OS/DFS difference; lymphedema 13% (ALND) vs 2% (SLNB alone) |
| SSO-ASTRO 2014 | "No ink on tumor" is the adequate negative margin definition for IDC; wider margins do not reduce IBTR |
| TAILORx | Oncotype DX RS 0-10: 98.7% recurrence-free at 5 years on endocrine therapy alone |
| MINDACT | MammaPrint low genomic risk in high clinical-risk patients: 94.7% distant metastasis-free survival without chemo |
| NSABP B-51 / NEJM 2025 | Omitting regional nodal irradiation after NACT complete response is feasible (PMID 40466065) |
| BCS vs. Mastectomy Meta-analysis 2024 | Equivalent OS; BCS + RT non-inferior (PMID 38758563) |
QUICK REFERENCE SUMMARY CARD
PATIENT: 45yo woman | Right IDC | Stage IIB (T2N1M0 or T3N0M0)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
IMAGING → BI-RADS 5 (mammogram/US) → Core biopsy → BI-RADS 6
STAGING WORKUP → CT CAP + Bone scan + ER/PR/HER2/Ki-67 + BRCA
MDT DECISION → NACT if large/HER2+/TNBC | Upfront surgery if BCS-eligible
NACT → AC × 4 → T × 4 (±trastuzumab if HER2+)
SURGERY → BCS (if downstaged) or MRM | SLNB ± ALND
POST-OP RT → Whole breast (BCS) or chest wall + nodes (mastectomy)
CHEMO → Per molecular subtype + pCR status
ENDOCRINE → Tamoxifen ± OFS (premenopausal, ER+)
TARGETED → Trastuzumab (HER2+) | Olaparib (BRCA+) | Abemaciclib (HR+N+)
SURVEILLANCE → 3-6 monthly × 3 yrs → annual lifelong + mammography
SPECIAL → Fertility preservation | BRCA counseling | Psycho-oncology
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Primary Sources:
- Bailey and Love's Short Practice of Surgery 28th Edition (Tables 58.1, 58.3; pp. 938-963)
- Schwartz's Principles of Surgery 11th Edition (Tables 17-10, 17-12; pp. 579-832)
- Fischer's Mastery of Surgery 8th Edition (Tables 52.2, 52.3; pp. 1406-1718)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 978-985)
- Robbins & Kumar Basic Pathology (p. 719)
This is a shared conversation. Sign in to Orris to start your own chat.