Explain me 10 common heart diseases with ecg changes and ecg images of those diseases
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram myocardial infarction ST elevation
Searching Images
atrial fibrillation ECG irregularly irregular rhythm absent P waves
Searching Images
complete heart block third degree AV block ECG
Searching Images
left bundle branch block LBBB ECG
Searching Images
Wolff-Parkinson-White syndrome delta wave ECG pre-excitation
Searching Images
hyperkalemia peaked T waves wide QRS ECG
Searching Images
ventricular tachycardia wide complex tachycardia ECG
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain sinus tachycardia
Searching Images
pericarditis saddle shaped ST elevation PR depression ECG
Searching Images
left ventricular hypertrophy LVH ECG voltage criteria
Here is a comprehensive overview of 10 common heart diseases with their ECG changes and real ECG images from the medical literature.
10 Common Heart Diseases: ECG Changes & Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
What it is
STEMI results from complete occlusion of a coronary artery (most commonly the LAD, RCA, or LCx), causing full-thickness myocardial injury. It is the most time-critical cardiac emergency.
ECG Changes
| Feature | Description |
|---|---|
| ST elevation | ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in ≥2 contiguous precordial leads |
| Hyperacute T waves | Tall, broad, peaked T waves — earliest sign |
| Reciprocal ST depression | In leads opposite to the infarct territory |
| Pathological Q waves | Develop within hours–days (>40 ms wide, >25% of R-wave height) |
| ST evolution | ST → T-wave inversion → Q waves over hours |
Localisation:
- Anterior STEMI → ST↑ in V1–V4 (LAD)
- Inferior STEMI → ST↑ in II, III, aVF (RCA)
- Lateral STEMI → ST↑ in I, aVL, V5–V6 (LCx)
- Posterior STEMI → Tall R + ST depression in V1–V3 (mirror image)

Acute anterolateral STEMI: convex ST elevation V1–V6, ST elevation in I/aVL, hyperacute T waves in V2–V4, reciprocal ST depression in II/III/aVF. Proximal LAD occlusion.
2. 🫀 Atrial Fibrillation (AF)
What it is
AF is the most common sustained cardiac arrhythmia, caused by chaotic re-entrant electrical activity in the atria (often triggered from pulmonary vein foci). It affects ~1–2% of the general population and is a major stroke risk factor.
ECG Changes
| Feature | Description |
|---|---|
| Absent P waves | Replaced by irregular fibrillatory baseline (f-waves) |
| Irregularly irregular R-R intervals | Hallmark finding — no two R-R intervals are the same |
| Narrow QRS complexes | Usually <120 ms (unless aberrant conduction) |
| Fibrillatory baseline | Best seen in V1 and lead II |
| Rate | Ventricular rate 60–170 bpm depending on AV node conduction |
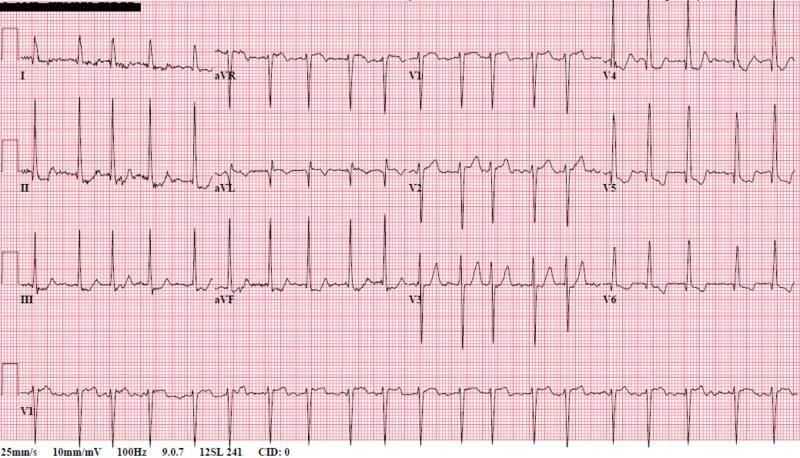
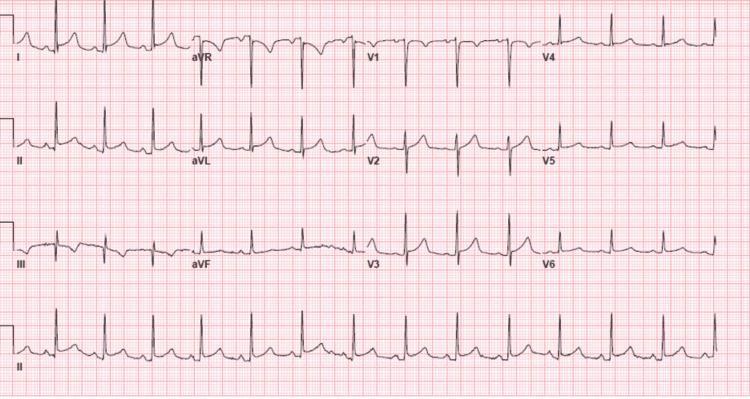
AF with RVR: absent P waves, chaotic fibrillatory baseline (best seen in V1), irregular R-R intervals, narrow QRS complexes, LVH voltage pattern in V4–V6.
3. 🫀 Complete (Third-Degree) Heart Block
What it is
Third-degree AV block is complete failure of conduction between the atria and ventricles. The atria and ventricles beat independently — the ventricles are maintained by a slow escape rhythm from the AV junction or bundle of His/Purkinje system.
ECG Changes
| Feature | Description |
|---|---|
| Complete AV dissociation | P waves and QRS complexes bear NO relationship to each other |
| Regular P-P intervals | Atrial rate 60–100 bpm, regular |
| Regular R-R intervals | Ventricular escape rate 20–40 bpm (slower than atrial) |
| P waves "march through" QRS | P waves appear before, inside, and after QRS complexes |
| Wide QRS | If escape from ventricle (>120 ms); narrow if junctional escape |
Third-degree heart block: regular ventricular escape rhythm at ~55 bpm with wide QRS (>120 ms), P waves visible but completely dissociated from QRS complexes — infra-Hisian escape focus.
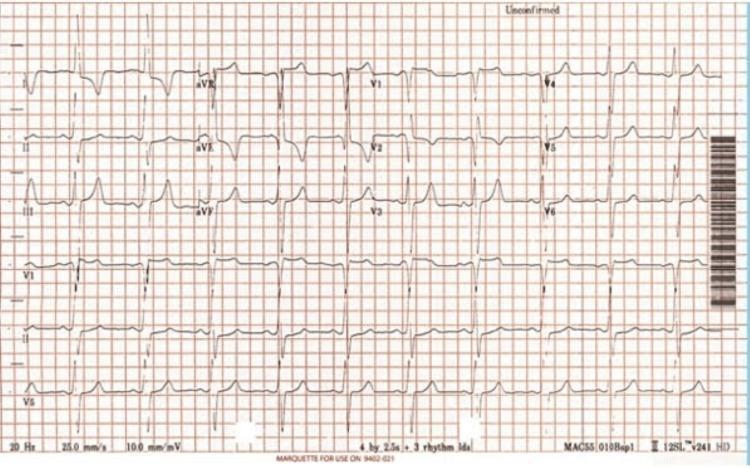
4. 🫀 Left Bundle Branch Block (LBBB)
What it is
LBBB occurs when conduction through the left bundle branch is blocked, forcing the left ventricle to depolarize late via cell-to-cell spread from the right ventricle. It is associated with structural heart disease (cardiomyopathy, CAD, hypertension) and can mask ischemia.
ECG Changes
| Feature | Description |
|---|---|
| Wide QRS | ≥120 ms |
| Broad monophasic R in I, aVL, V5–V6 | Often with notching/slurring ("M-pattern") |
| Deep QS or rS in V1–V3 | Predominantly negative deflection |
| Secondary ST-T changes | ST/T discordant to QRS — ST depression + T inversion in lateral leads; ST elevation in V1–V3 |
| No septal Q in I, V5, V6 | Absence of normal septal q waves |
Sgarbossa criteria allow detection of acute MI despite LBBB:
- Concordant ST elevation ≥1 mm in any lead
- Concordant ST depression ≥1 mm in V1–V3
- Excessively discordant ST elevation ≥5 mm
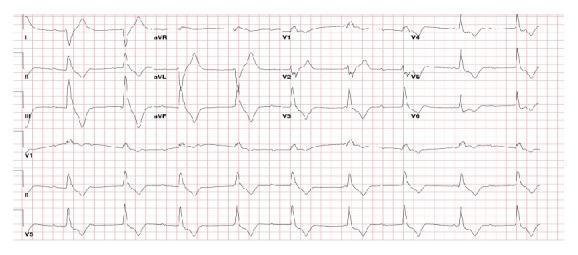
Classic LBBB in sinus tachycardia: QRS >120 ms, broad monophasic R in I/aVL/V5/V6 with slurring, deep S waves in V1–V3, discordant ST elevation in V1–V3 and ST depression/T inversion in lateral leads.
5. 🫀 Wolff-Parkinson-White (WPW) Syndrome
What it is
WPW is a pre-excitation syndrome caused by an accessory conduction pathway (Bundle of Kent) that bypasses the AV node, allowing early ventricular activation. Patients are prone to re-entrant supraventricular tachycardias (SVT) and — dangerously — rapid conduction during atrial fibrillation.
ECG Changes
| Feature | Description |
|---|---|
| Short PR interval | <120 ms — early ventricular activation bypasses AV node delay |
| Delta wave | Slurred, slow upstroke at the beginning of QRS |
| Wide QRS | >120 ms — fusion of pre-excitation + normal conduction |
| Secondary ST-T changes | Opposite to delta wave direction |
| Pseudo-Q waves | Negative delta waves can mimic infarct Q waves |
Pathway localisation by delta wave polarity:
- Left lateral: negative delta in I/aVL
- Posteroseptal: negative delta in II/III/aVF
- Right free wall: negative delta in V1, positive in I

WPW: short PR interval (<120 ms), characteristic delta waves (slurred QRS upstroke, marked by red arrows in II and III), widened QRS complexes — pre-excitation via an accessory pathway.
6. 🫀 Ventricular Tachycardia (VT)
What it is
VT is a life-threatening arrhythmia originating from ventricular myocardium, defined as ≥3 consecutive ventricular beats at rate >100 bpm. Sustained VT (>30 seconds) can degenerate into ventricular fibrillation. Most commonly occurs in structural heart disease (post-MI scar, cardiomyopathy).
ECG Changes
| Feature | Description |
|---|---|
| Wide QRS | >120 ms (typically >140 ms) |
| Regular rapid rate | Usually 140–240 bpm |
| AV dissociation | P waves march through QRS independently — most specific sign |
| Fusion beats | QRS morphology between normal and VT beat |
| Capture beats | Rare narrow QRS — momentary sinus capture |
| QRS concordance | All precordial leads positive (positive concordance) or all negative |
| Northwest axis | Negative in I and aVF simultaneously ("extreme axis deviation") |
Brugada criteria and Vereckei criteria help differentiate VT from SVT with aberrancy.

Monomorphic VT: rapid regular wide-complex tachycardia, positive QRS concordance across precordial leads (V1–V6 all positive), superior axis, no visible P waves — consistent with structural heart disease-related VT.
7. 🫀 Acute Pulmonary Embolism (PE)
What it is
Massive or submassive PE causes acute right ventricular pressure overload as the RV must pump against the obstructed pulmonary vasculature. ECG changes reflect acute RV strain and are present in ~70% of PE cases.
ECG Changes
| Feature | Description |
|---|---|
| Sinus tachycardia | Most common finding (>44% of cases) |
| S1Q3T3 pattern | S wave in lead I + Q wave in III + T-wave inversion in III |
| Right bundle branch block | Complete or incomplete RBBB — acute RV strain |
| T-wave inversion V1–V4 | Right precordial strain pattern |
| Rightward axis shift | New right axis deviation |
| P pulmonale | Tall peaked P waves >2.5 mm in II — right atrial enlargement |
| Low voltage or sinus tachycardia alone | In smaller PE |

Acute massive PE: sinus tachycardia at 116 bpm, S1Q3T3 pattern (S in lead I, Q and T inversion in III), T-wave inversion V1–V3, incomplete RBBB morphology (110 ms) — classic right ventricular strain pattern.
8. 🫀 Acute Pericarditis
What it is
Pericarditis is inflammation of the pericardial sac (usually viral — coxsackie, EBV, CMV). Inflammation extends to the epicardium causing widespread ST-segment and PR changes that differ crucially from MI.
ECG Changes (evolve through 4 stages)
| Stage | Timing | ECG Features |
|---|---|---|
| Stage I | Hours–days | Diffuse concave ST elevation (all leads except aVR, V1), PR depression |
| Stage II | Days | ST returns to baseline, T waves flatten |
| Stage III | 1–3 weeks | Widespread T-wave inversion |
| Stage IV | Weeks | ECG normalises |
Key distinguishing features from STEMI:
- Diffuse ST elevation (not in a coronary territory)
- Concave/saddle-shaped ST elevation (vs. convex in STEMI)
- PR depression in II/V4–V6 (PR elevation in aVR) — most specific sign
- No reciprocal ST depression (except aVR)
- Spodick's sign: downsloping TP segment
Acute pericarditis: diffuse concave (saddle-shaped) ST elevation across I, II, III, aVF and V2–V6, PR depression in II/III/aVF/V4–V6, reciprocal ST depression and PR elevation only in aVR — classic Stage I pericarditis.
9. 🫀 Left Ventricular Hypertrophy (LVH)
What it is
LVH results from chronic pressure overload (hypertension, aortic stenosis) or volume overload causing concentric or eccentric thickening of the left ventricle. ECG voltage criteria reflect the increased myocardial mass.
ECG Changes
| Feature | Description |
|---|---|
| Increased QRS voltage | See criteria below |
| Left axis deviation | –30° or more |
| LV strain pattern | ST depression + asymmetric T inversion in lateral leads (I, aVL, V5–V6) |
| Delayed intrinsicoid deflection | R-peak time in V5–V6 ≥55 ms |
| Repolarisation changes | Secondary to abnormal depolarisation |
Voltage Criteria:
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥35 mm
- Cornell voltage: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- R in aVL ≥11 mm alone
LVH with strain pattern: high-amplitude R in aVL + deep S in V3 meeting Cornell voltage criteria (>28 mm), deep T-wave inversions in lateral leads V4–V6 and I/aVL indicating the "strain pattern" of severe pressure-overload hypertrophy.
10. 🫀 Hyperkalemia (Cardiac Effects)
What it is
While hyperkalemia is an electrolyte disorder (usually from renal failure, medications, or tissue breakdown), its cardiac manifestations on ECG are characteristic, progressive, and potentially fatal. The ECG changes correlate roughly with the serum potassium level.
ECG Changes (Progressive with rising K⁺)
| K⁺ Level | ECG Changes |
|---|---|
| 5.5–6.5 mEq/L | Tall, narrow, peaked ("tented") T waves — earliest sign; best in V2–V5 |
| 6.5–7.5 mEq/L | PR prolongation, flat or absent P waves, widening QRS |
| 7.5–8.5 mEq/L | Progressive QRS widening, sine-wave pattern, loss of P waves (sinoventricular rhythm) |
| >8.5 mEq/L | Ventricular fibrillation or asystole |
Tall T waves in hyperkalemia vs. hyperacute T waves in STEMI: Hyperkalemia T waves are symmetric and narrow-based, not associated with ST elevation; hyperacute STEMI T waves are asymmetric and associated with ST changes.
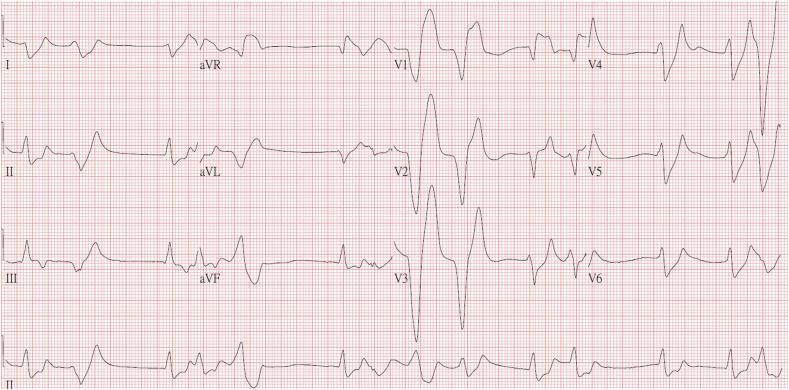
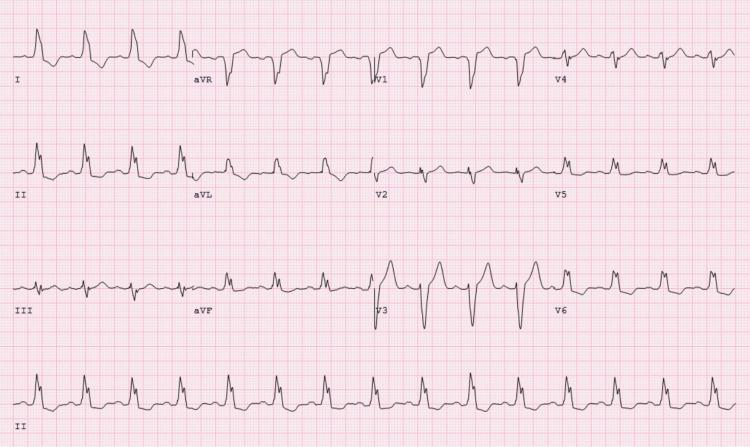
Severe hyperkalemia (K⁺ = 9.2 mEq/L): tall narrow-based peaked T waves most prominent in V2–V4, significantly widened QRS complexes across all leads, absent P waves (sinoventricular rhythm), sine-wave QRS morphology in V2–V3 — imminent risk of VF.
Quick Reference Summary
| # | Disease | Key ECG Findings |
|---|---|---|
| 1 | STEMI | Convex ST elevation + reciprocal depression + Q waves (territory-specific) |
| 2 | Atrial Fibrillation | Absent P waves + irregularly irregular RR + narrow QRS |
| 3 | Complete Heart Block | P and QRS dissociated, ventricular escape rhythm |
| 4 | LBBB | Wide QRS, broad R in V5/V6, QS in V1/V2, discordant ST-T |
| 5 | WPW | Short PR + delta wave + wide QRS |
| 6 | Ventricular Tachycardia | Wide QRS tachycardia + AV dissociation + fusion/capture beats |
| 7 | Pulmonary Embolism | Sinus tachycardia + S1Q3T3 + T inversion V1–V4 + RBBB |
| 8 | Acute Pericarditis | Diffuse saddle-shaped ST elevation + PR depression in all leads |
| 9 | LVH | High QRS voltage (Sokolow/Cornell criteria) + lateral strain pattern |
| 10 | Hyperkalemia | Peaked T waves → QRS widening → absent P waves → sine wave |
Clinical Pearl: The ECG is not a standalone diagnostic tool — always correlate with clinical history, symptoms, biomarkers (troponin, BNP), and imaging. Life-threatening patterns (STEMI, VT, complete heart block, severe hyperkalemia) require immediate action regardless of other findings.
This is a shared conversation. Sign in to Orris to start your own chat.